Sexual Maturation
Sexuality is a complex aspect of human development. Here we consider biological changes at puberty and some of the cultural variations and implications. Variations are discussed again in later chapters, as is sex education.
Sexual Characteristics
The body characteristics that are directly involved in conception and pregnancy are called primary sex characteristics. During puberty, every primary sex organ (the ovaries, the uterus, the penis, and the testes) increases dramatically in size and matures in function. By the end of the process, reproduction is possible.
At the same time that maturation of the primary sex characteristics occurs, secondary sex characteristics develop. Secondary sex characteristics are bodily features that do not directly affect reproduction (hence they are secondary) but that signify masculinity or femininity.
One secondary characteristic is shape. Young boys and girls have similar shapes, but at puberty males widen at the shoulders and grow about 5 inches taller than females, while girls widen at the hips and develop breasts. Those female curves are often considered signs of womanhood, but neither breasts nor wide hips are required for conception; thus, they are secondary, not primary, sex characteristics.
The pattern of hair growth at the scalp line (widow’s peak), the prominence of the larynx (Adam’s apple), and several other anatomical features differ for men and women; all are secondary sex characteristics that few people notice. As previously explained, facial hair increases in both sexes, affected by sex hormones as well as genes.
Secondary sex characteristics are important psychologically, if not biologically. Breasts are an obvious example. Many adolescent girls buy “minimizer,” “maximizer,” “training,” or “shaping” bras in the hope that their breasts will conform to an idealized body image. During the same years, many overweight boys are horrified to notice a swelling around their nipples—
Sexual Activity
The primary and secondary sex characteristics just described are not the only evidence of sex hormones. Fantasizing, flirting, hand-
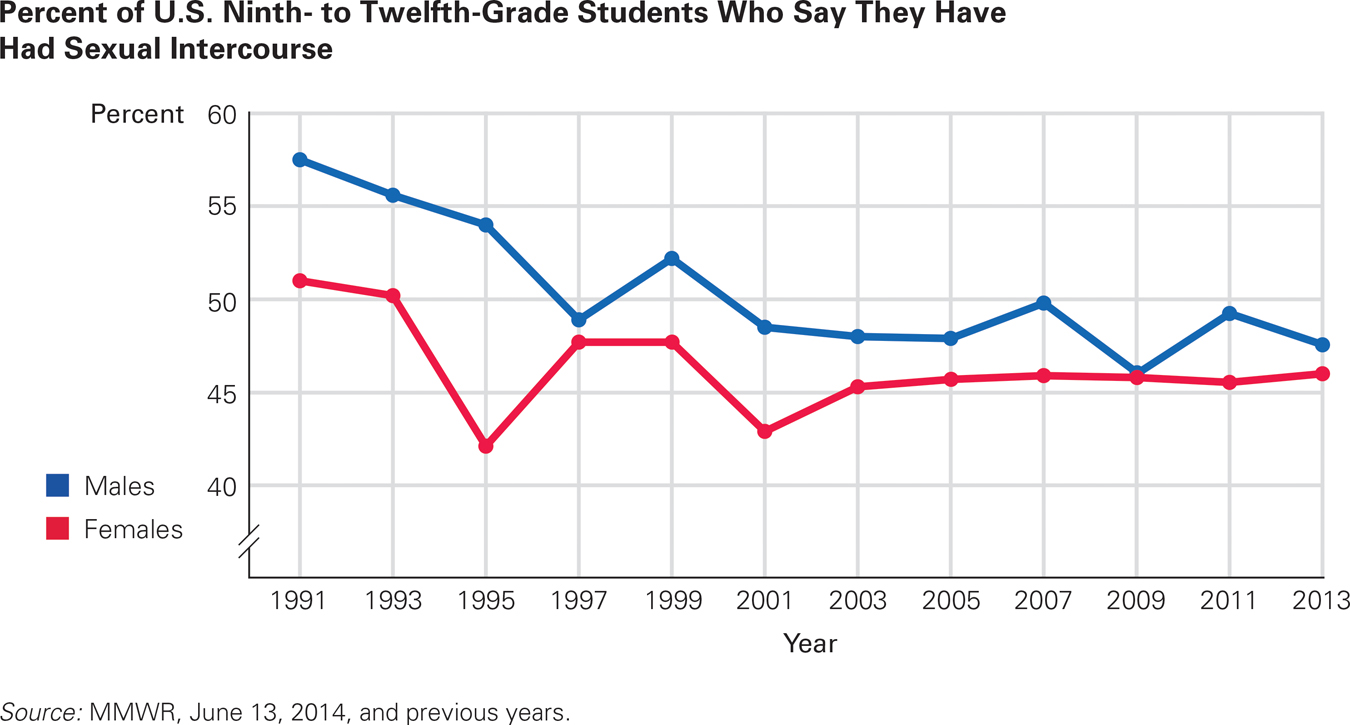
Boys and Girls Together Boys tend to be somewhat more sexually experienced than girls during the high school years, but since the Youth Risk Behavior Survey began in 1991, the overall trend has been toward equality in rates of sexual activity.
A recent study on sexual behaviors such as hand-
Regarding sex-
Everyone, however, is influenced by hormones and society, biology and culture. All adolescents have sexual interests they did not previously have (biology), which produce behaviors engaged in by teenagers in some nations that teenagers of other nations would not engage in (culture). Since only girls can become pregnant, their wish for long-
For whatever reason, the gender gap in experience is narrowing. It has already been reversed in some European nations, such as Norway, where sex education begins in childhood. By adolescence, today’s Norwegian teenagers know how to prevent the unwanted consequences of intercourse. In 1987, Norwegian boys had their first sexual intercourse almost a year younger than girls did; by 2002, the sexes flipped, with girls averaging half a year younger than boys (Stigum et al., 2010).
In the United States, rates of sexual activity are almost even, with minor gender differences. For example, among high school students, 46 percent of the girls and 47.5 percent of the boys say they have had sexual intercourse, 35 percent of the girls and 33 percent of the boys say they have had intercourse in the past 3 months, and 13 percent of the girls and 17 percent of the boys say they have had 4 or more sexual partners (MMWR, June 13, 2014).
Within nations, ethnic differences are narrowing as well, with every group less sexually active than the previous cohort. Between 1991 and 2013, according to an anonymous questionnaire, intercourse experience among African American high school students decreased 25 percent (to 61 percent); among European Americans, down 12 percent (45 percent); and among Latinos, down 9 percent (47 percent) (MMWR, June 13, 2014).
One statistic illustrates this new trend. In 1991, 62 percent of U.S. eleventh-
The trend toward later sexual activity is international, although as marriages occur later, rates of premarital sex are rising. More teenagers worldwide are virgins than was true a decade ago, a trend documented in China, where, unlike earlier, first intercourse does not occur until age 20, on average (Yu et al., 2013).
All these examples demonstrate that a universal experience (rising hormones) that produces another universal experience (growth of primary and secondary sex characteristics) is influenced by cohort, gender, and culture. Other research finds that the most powerful influence on adolescents’ sexual activity is their close friends, not national or local norms for their gender or their ethnic group.
Sexual Problems in Adolescence

Sexual interest and interaction are part of adolescence; healthy adult relationships are more likely to develop when adolescent impulses are not haunted by shame and fear (Tolman & McClelland, 2011). Although guidance is needed, teenagers are healthy and normal, not depraved or evil, in experiencing sexual urges. Before focusing on the hazards of adolescent sex, we should note that several “problems” are less troubling now than in earlier decades. Here are three specifics:
Teen births have decreased in every nation. Teen births have been declining (World Health Organization, December 1, 2012). In the United States, births to teenage mothers (aged 15 to 19) decreased 25 percent between 2007 and 2011 across race and ethnicity, with the biggest drop among Hispanic teens (Martin et al., 2010; Centers for Disease Control and Prevention, June 16, 2014). Similar declines are evident in other nations. In China, the teen pregnancy rate was cut in half from 1960 to 2010 (reducing the United Nations’ projections of the world’s population in 2050 by about 1 billion).
The use of “protection” has risen. Contraception, particularly condom use among adolescent boys, has increased markedly in most nations since 1990 (Santelli & Melnikas, 2010). The U.S. Youth Risk Behavior Survey found that 63 percent of sexually active ninth-
grade boys used a condom during their most recent intercourse (MMWR, June 13, 2014). The teen abortion rate is down. In general, the teen abortion rate in the United States has declined every year since abortion became legal. The rate today is about half that of 20 years earlier (Kost & Henshaw, 2013), even as the rate among older women has increased. The reason is primarily that contraception is more prevalent, so unwanted teen pregnancies are less common. Internationally, however, abortion rates among teenagers are very difficult to track. An estimated three million girls aged 15 to 19 undergo unsafe abortions each year, mostly in low-
and middle- income countries (World Health Organization, December 1, 2012).
These are positive trends, but many aspects of adolescent sexual activity remain problematic.
Sex Too Soon
Sex can, of course, be thrilling and affirming, providing a bonding experience. However, compared to a century ago, adolescent sexual activity—
Earlier puberty and weaker social taboos mean some very young teens have sexual experiences. Early sex correlates with depression and drug abuse.
Most teenage mothers have no husbands to help them. A century ago, teenage mothers were married; now, in the United States, 85 percent are unwed.
Raising a child has become more complex and expensive, and most young grandmothers are employed, so fewer of them provide full-
time care. Sexually transmitted infections are more common and dangerous.

As you just read, teen births are declining, as are teen abortions. However, the U.S. rate of adolescent pregnancy is the highest of any developed nation (true among every ethnic group). Such pregnancies are risky. If a pregnant girl is under 16 (most are not), she is more likely than pregnant teenagers who are a year or two older to experience complications—
There are many reasons in addition to age for these hazards. Poverty and lack of education correlate with teen pregnancy and with every problem just listed (Santelli & Melnikas, 2010). Beyond that, younger pregnant teenagers are often malnourished and postpone prenatal care (Borkowski et al., 2007).
After birth, adolescents are often less responsive, so insecure attachment is more common. For children as well as adults, the decline in teen pregnancy is good news. (Developmental Link: Attachment types and the importance of early attachment were discussed in Chapter 7.)
Even without pregnancy, teenagers who have sex risk psychosocial problems. A study of 3,923 adult women in the United States found that those who voluntarily had sex before age 16 were more likely to divorce later on, whether or not they became pregnant or later married their first sexual partner. The same study found that adolescents whose first sexual experience was unwanted (either “really didn’t want it” or “had mixed feelings”) were also more likely to divorce (Paik, 2011).
Forced sex is much worse, of course, as now explained.
Sexual Abuse
Teenage births are risky, but sexual abuse is devastating: It harms development lifelong. Child sexual abuse is defined as any sexual activity (including fondling and photographing) between a juvenile and an adult, with age 18 the usual demarcation (although legal age varies by state). Girls are particularly vulnerable, although boys are also at risk.
The rate of sexual abuse increases at puberty, a sensitive time because many young adolescents are confused about their own sexual urges and identity (Graber et al., 2010). Virtually every adolescent problem, including pregnancy, drug abuse, eating disorders, and suicide, is more frequent in adolescents who are sexually abused.
Especially for Parents Worried About Their Teenager’s Risk Taking You remember the risky things you did at the same age, and you are alarmed by the possibility that your child will follow in your footsteps. What should you do?
You are right to be concerned, but you cannot keep your child locked up for the next decade or so. Since you know that some rebellion and irrationality are likely, try to minimize them by not boasting about your own youthful exploits, by reacting sternly to the inevitable minor infractions so your child can rebel without disastrous consequences, and by making allies of your child’s teachers.
This is true worldwide. The United Nations reports that millions of girls in their early teens are forced into marriage or prostitution (often across national borders) each year (Pinheiro, 2006). Adolescent girls are common victims of sex trafficking, not only because their youth makes them more alluring but also because their immaturity makes them more vulnerable (McClain & Garrity, 2011). Some believe they are helping their families by earning money to support them, others are literally sold by their families (Kara, 2009).
That is less likely in developed nations, where sexual abuse of children usually occurs within homes. In the United States, the person most likely to sexually abuse a child or young adolescent is a family member, who typically isolates the victim, depriving him or her of the friendships and romances that aid in developing a healthy and satisfying life. Sometimes that family member is a biological parent, but more often it is a stepfather or uncle, trusted by the mother and therefore with access to the child. Young people who are sexually exploited tend to fear sex and to devalue themselves lifelong.
A longitudinal study in Washington, D.C. of 84 reported victims of child sexual abuse (all girls) included interviews with each of them six times over 23 years (Trickett et al., 2011). In order to isolate the effects of abuse, the researchers also followed the development of individuals from the same backgrounds (SES, ethnicity, and so on) who were not sexually abused.
Every possible problem that was studied was far more common in the victims than in their nonvictimized peers. Problems included attitudes directly related to abuse (e.g., most of those abused by their biological fathers thought of sex as dirty, shameful, and dangerous) and behaviors seemingly unconnected (e.g., although their body weight was normal in childhood, 42 percent were obese in their 20s).
Cognitive development—
Almost half of the girls who were abused became mothers. They had a total of 78 children, three of whom died in infancy and nine of whom were permanently removed from their mothers, who had severely maltreated them. These rates are much higher than rates among the nonvictimized mothers from the same income and ethnic groups.
Early in this chapter, we noted that the HPA system regulates puberty and many other physiological responses. Many of the formerly abused women had abnormal HPA regulation, with alteration of their cortisol responses. That condition produced heightened stress reactions in early adolescence but then abnormally low-
Fortunately, now that sexual abuse is reported more often, it has become less common, with “large declines in sexual abuse from 1992 to 2010” in the United States (Finkelhor & Jones, 2012, p. 3). Worldwide, about 13 percent of women say they were sexually abused as children (Stoltenborgh et al., 2011). Of course, even one instance is too many.
Our discussion of sex abuse focuses on girls, because they are the most common victims. However, teenage boys may be sexually abused as well, a direct attack on their fledgling identity as men (Dorais, 2009).
Remember that perpetrators of all kinds of abuse are often people known to the child. After puberty, although sometimes abusers are parents, coaches, or other authorities, often they are other teenagers. In the Youth Risk Behavior Survey of U.S. high school students, 14 percent of the girls and 6 percent of the boys said they had been kissed, touched, or forced to have sex within a dating relationship when they did not want to (MMWR June 13, 2014). Sex education is discussed in Chapter 16; obviously teenagers have much to learn.
Sexually Transmitted Infections
Unlike teen pregnancy and sexual abuse, the other major problem of teenage sex shows no signs of abating. A sexually transmitted infection (STI) (sometimes called a sexually transmitted disease [STD]) is any infection transmitted through sexual contact. Worldwide, sexually active teenagers have higher rates of the most common STIs—
In the United States, half of all new STIs occur in people ages 15 to 25, even though this age group has less than one-
There are hundreds of STIs. Chlamydia is the most frequently reported one; it often begins without symptoms, yet it can cause permanent infertility. Worse is human papillomavirus (HPV), which has no immediate consequences but increases the risk of “serious, life-
National variations in laws and rates of STIs are large. Rates among U.S. teenagers are higher than those in any other medically advanced nation, but lower than rates in some developing nations. HIV rates are not declining, despite increased awareness.
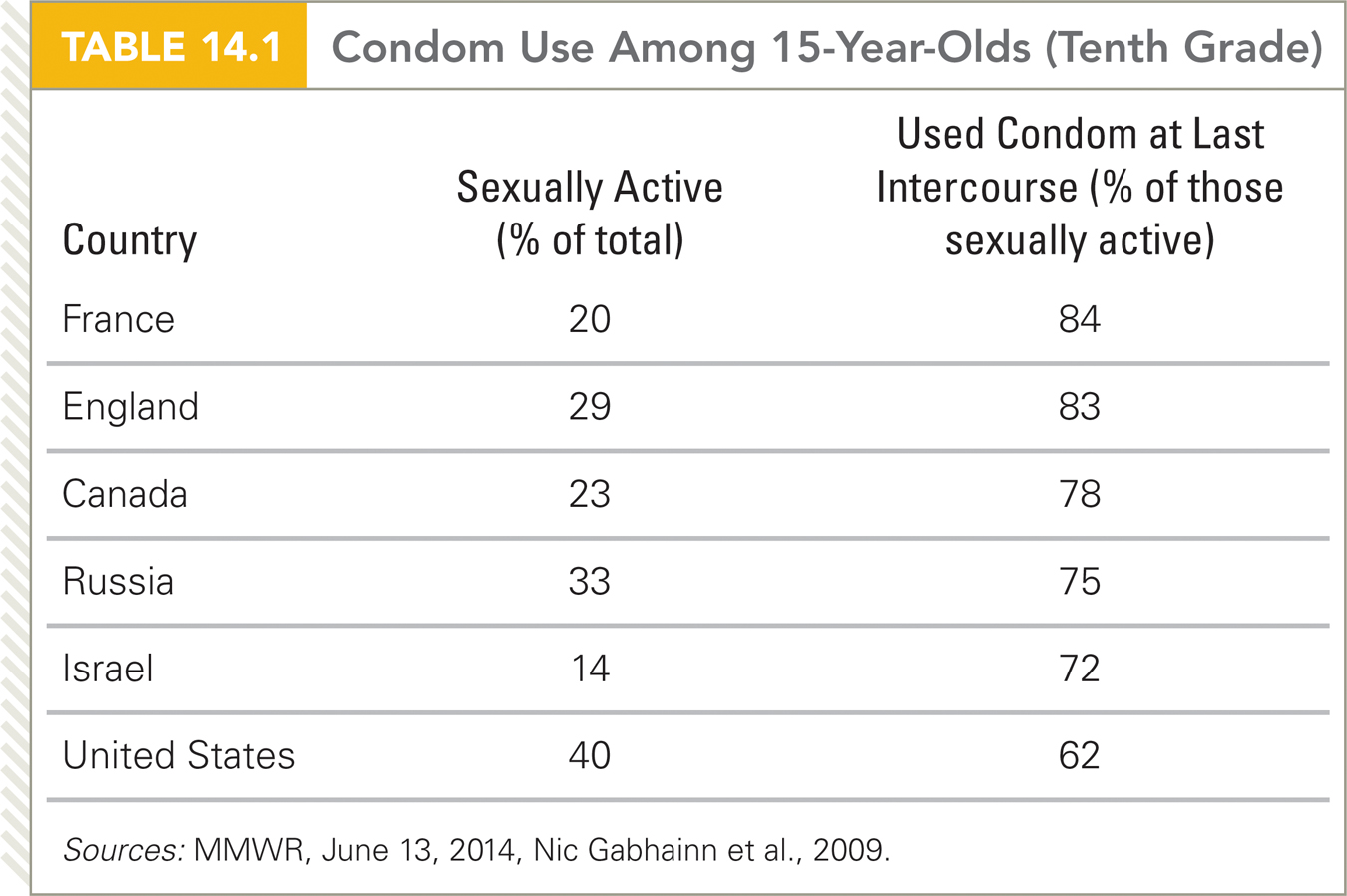
Internationally, a comparison of 30 developed nations found that French teenagers were among the most likely to use condoms, while those in the United States were least likely to do so (MMWR, June 13, 2014; Nic Gabhainn et al., 2009) (see Table 14.1). One reason French teenagers use condoms may be that, by law, every French high school (including Catholic ones) must offer free, confidential medical care and condoms. By contrast, providing either is illegal at many U.S. schools.
Once again, it is apparent that a universal experience (the biology of puberty) varies remarkably depending on culture. As we stated earlier, adolescence begins with biology and ends with culture. You will see more examples in the next chapter, as you learn that schools for adolescents vary a great deal in how and what they teach.
SUMMING UP Sexual differentiation is another example of the dramatic transformations of puberty. Primary sex characteristics, which are directly connected to reproduction, develop; so do secondary sex characteristics, which signify masculinity or femininity but are not necessary for pregnancy. Sexual interest increases as bodies mature and hormone levels rise, with differences between males and females in sexual activity more apparent in some nations than others. Early parenthood, sexual abuse, and sexually transmitted infections are increasingly hazardous. The first two of these are becoming less frequent, but STIs are alarmingly common among teenagers, especially in the United States. Untreated, some of these lead to lifelong infertility, while others lead to death in adulthood. Some nations have policies in place to help protect adolescents from such hazards, but many others do not.
WHAT HAVE YOU LEARNED?
Question 14.24
What are examples of the difference between primary and secondary sex characteristics?
Primary sex characteristics, such as menarche and spermarche, are changes that enable reproduction. Secondary sex characteristics, such as breast development and facial hair, signal reproductive capability, but are unnecessary for reproduction.Question 14.25
Why are there fewer problems caused by adolescent sexuality now than a few decades ago?
Overall, trends in sexual activity are declining. In 1991, 62 percent of U.S. eleventh graders said they had had intercourse, but in 2013 only 47 percent said so. More teenagers worldwide are virgins than was true a decade ago. In addition, teen births have decreased in every nation, the use of “protection” has risen, and the teen abortion rate is down.Question 14.26
What are the problems with adolescent pregnancy?
The U.S. rate of adolescent pregnancy is the highest of any developed nation. Such pregnancies are risky. If a pregnant girl is under 16 (most are not), she is more likely than pregnant teenagers who are a year or two older to experience complications—including spontaneous or induced abortion, high blood pressure, stillbirth, preterm birth, and an underweight newborn. There are many reasons in addition to age for these hazards. Poverty and lack of education correlate with teen pregnancy and with every problem just listed. Beyond that, younger pregnant teenagers are often malnourished and postpone prenatal care. After birth, adolescents are often less responsive, so insecure attachment is more common. Most teenage mothers have no husbands to help them. A century ago, teenage mothers were married; now, in the United States, 85 percent are unwed. Raising a child has become more complex and expensive, and most young grandmothers are employed, so fewer of them provide full– time care. Question 14.27
Among sexually active people, why do adolescents have more STIs than adults?
Biologically, teens' bodies are not as equipped to fend off STIs as adults are, with girls being more susceptible than boys. Fully developed women have some natural biological defenses against STIs. In addition, sexually active teens are hesitant to seek treatment or alert their partners. In cultures or families where teenage sex is forbidden, adolescents avoid treatment for STIs until pain requires it. Adolescents with same–sex partners are especially reluctant to find treatment if their community considers homosexuality shameful. Question 14.28
What are the effects of child sexual abuse?
A longitudinal study found that abused children grow up to have negative attitudes, regarding sex as dirty, shameful, and dangerous. Although their body weight was in the normal range in childhood, 42 percent were obese in their 20s. Cognitive development—school achievement as well as language use— was also impaired. Among the most troubling results were much higher rates of self– harm, aggression, and repeated victimization— both sexual and physical abuse.