9.3 What Are the Underlying Causes of Suicide?
Most people faced with difficult situations never try to kill themselves. In an effort to understand why some people are more prone to suicide than others, theorists have proposed more fundamental explanations for self-
The Psychodynamic View
Many psychodynamic theorists believe that suicide results from depression and from anger at others that is redirected toward oneself. This theory was first stated by Wilhelm Stekel at a meeting in Vienna in 1910, when he proclaimed that “no one kills himself who has not wanted to kill another or at least wished the death of another” (Shneidman, 1979). Some years later Sigmund Freud (1920) wrote, “No neurotic harbors thoughts of suicide which he has not turned back upon himself from murderous impulses against others.” Agreeing with this notion, the influential psychiatrist Karl Menninger called suicide “murder in the 180th degree.”
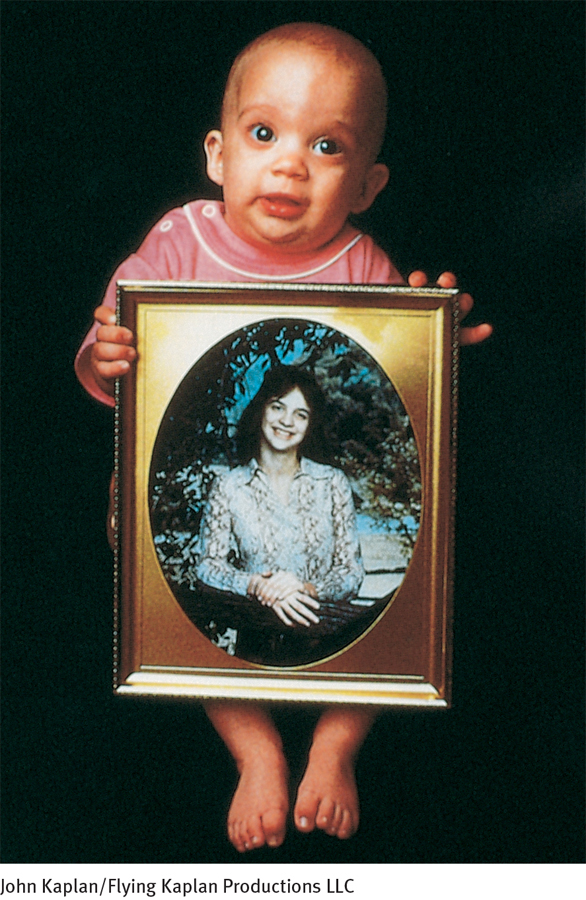
As you read in Chapter 7, Freud (1917) and Abraham (1916, 1911) proposed that when people experience the real or symbolic loss of a loved one, they come to “introject” the lost person; that is, they unconsciously incorporate the person into their own identity and feel toward themselves as they had felt toward the other. For a short while, negative feelings toward the lost loved one are experienced as self-
BETWEEN THE LINES
Most Common Killings
More suicides (38,364) than homicides (18,000) are committed in the United States each year (CDC, 2011).
A 27-
(Gill, 1982, p. 15)

In support of Freud’s view, researchers have often found a relationship between childhood losses—
Late in his career, Freud proposed that human beings have a basic “death instinct.” He called this instinct Thanatos and said that it opposes the “life instinct.” According to Freud, while most people learn to redirect their death instinct by aiming it toward others, suicidal people, caught in a web of self-
Sociological findings are consistent with this explanation of suicide. National suicide rates have been found to drop in times of war (Maris, 2001), when, one could argue, people are encouraged to direct their self-
By the end of his career, Freud himself expressed dissatisfaction with his theory of suicide. Other psychodynamic theorists have also challenged his ideas over the years, yet themes of loss and self-
Durkheim’s Sociocultural View
Toward the end of the nineteenth century, Emile Durkheim (1897), a sociologist, developed a broad theory of suicidal behavior. Today this theory continues to be influential and is often supported by research (Fernquist, 2007). According to Durkheim, the probability of suicide is determined by how attached a person is to such social groups as the family, religious institutions, and community. The more thoroughly a person belongs, the lower the risk of suicide. Conversely, people who have poor relationships with their society are at higher risk of killing themselves. He defined several categories of suicide, including egoistic, altruistic, and anomic suicide.
Why might towns and countries in past times have been inclined to punish those who attempted suicide and their relatives?
Egoistic suicides are committed by people over whom society has little or no control. These people are not concerned with the norms or rules of society, nor are they integrated into the social fabric. According to Durkheim, this kind of suicide is more likely in people who are isolated, alienated, and nonreligious. The larger the number of such people living in a society, the higher that society’s suicide rate.
Altruistic suicides, in contrast, are committed by people who are so well integrated into the social structure that they intentionally sacrifice their lives for its well-
Anomic suicides, another category proposed by Durkheim, are those committed by people whose social environment fails to provide stable structures, such as family and religion, to support and give meaning to life. Such a societal condition, called anomie (literally, “without law”), leaves people without a sense of belonging. Unlike egoistic suicide, which is the act of a person who rejects the structures of a society, anomic suicide is the act of a person who has been let down by a disorganized, inadequate, often decaying society.
Durkheim argued that when societies go through periods of anomie, their suicide rates increase. Historical trends support this claim. Periods of economic depression may bring about some degree of anomie in a country, and national suicide rates tend to rise during such times (Noh, 2009; Maris, 2001). Periods of population change and increased immigration, too, tend to bring about a state of anomie, and again suicide rates rise (Kposowa et al., 2008).
A major change in a person’s immediate surroundings, rather than general societal problems, can also lead to anomic suicide. People who suddenly inherit a great deal of money, for example, may go through a period of anomie as their relationships with social, economic, and occupational structures are changed. Thus Durkheim predicted that societies with more opportunities for change in individual wealth or status would have higher suicide rates; this prediction is also supported by research (Cutright & Fernquist, 2001; Lester, 2000, 1985). Conversely, people who are removed from society and sent to a prison environment may experience anomie. As you read earlier, research confirms that such people have a heightened suicide rate (Fazel et al., 2011).
BETWEEN THE LINES
The Economics of Suicide
The annual cost of suicide deaths in the United States is $34 billion (lost wages and work productivity).
(AFSP, 2014)
Although today’s sociocultural theorists do not always embrace Durkheim’s particular ideas, most agree that social structure and cultural stress often play major roles in suicide. In fact, the sociocultural view pervades the study of suicide. Recall the earlier discussion of the many studies linking suicide to broad factors such as religious affiliation, marital status, gender, race, and societal stress. You will also see the impact of such factors when you read about the ties between suicide and age.
Despite the influence of sociocultural theories such as Durkheim’s, these theories cannot by themselves explain why some people who face particular societal pressures commit suicide while the majority do not. Durkheim himself concluded that the final explanation probably lies in the interaction between societal and individual factors.
The Biological View
For years, biological researchers have relied largely on family pedigree studies to support their position that biological factors contribute to suicidal behavior. They repeatedly have found higher rates of suicide among the parents and close relatives of suicidal people than among those of nonsuicidal people (Petersen et al., 2014; Roy, 2011; Brent & Mann, 2003). Such findings may suggest that genetic, and so biological, factors are at work.
Studies of twins also have supported this view of suicide. In a famous study, researchers who studied twins born in Denmark between 1870 and 1920 located 19 identical pairs and 58 fraternal pairs in which at least one twin had committed suicide (Juel-
Suicide sometimes runs in families. How might clinicians and researchers explain such family patterns?
As with all family pedigree and twin research, there are nonbiological interpretations for these findings as well. Psychodynamic clinicians might argue that children whose close relatives commit suicide are prone to depression and suicide because they have lost a loved one at a critical stage of development. Behavioral theorists might emphasize the modeling role played by parents or close relatives who attempt suicide.

In the past three decades, laboratory studies have offered more direct support for a biological view of suicide. One promising line of research focuses on serotonin. The activity level of this neurotransmitter has often been found to be low in people who commit suicide (Fabio Di Narzo et al., 2014; Pompili et al., 2010; Mann & Currier, 2007). An early hint of this relationship came from a study by psychiatric researcher Marie Asberg and her colleagues (1976). They studied 68 depressed patients and found that 20 of the patients had particularly low levels of serotonin activity. It turned out that 40 percent of the research participants with such serotonin levels attempted suicide, compared with 15 percent of those with higher serotonin levels. The researchers interpreted this to mean that low serotonin activity may be “a predictor of suicidal acts.” Later studies found that suicide attempters with low serotonin activity are 10 times more likely to make a repeat attempt and succeed than are suicide attempters with higher serotonin activity (Roy, 1992).
Subsequent studies that examined the autopsied brains of suicide victims pointed in the same direction (Fabio Di Narzo et al., 2014; Pompili et al., 2010; Stanley et al., 2000, 1986, 1982). Some of these studies found, for example, that people who committed suicide tended to have fewer receptor sites on neurons that normally receive serotonin than did people who do not commit suicide. Similarly, recent PET scan studies have revealed that people who contemplate or attempt suicide display abnormal activity in areas of the brain that comprise many serotonin-
At first glance, these and related studies may appear to tell us only that depressed people often attempt suicide. After all, depression is itself related to low serotonin activity. On the other hand, there is evidence of low serotonin activity even among suicidal people who have no history of depression (Mann & Currier, 2007). That is, low serotonin activity also seems to play a role in suicide separate from depression.
How, then, might low serotonin activity increase the likelihood of suicidal behavior? One possibility is that it contributes to aggressive and impulsive behaviors (Preti, 2011). It has been found, for example, that serotonin activity is lower in aggressive men than in nonaggressive men and that serotonin activity is often low in those who commit such aggressive acts as arson and murder (Oquendo et al., 2006, 2004; Stanley et al., 2000). Moreover, PET scan studies of people who are aggressive and impulsive (but not necessarily depressed) reveal abnormal activity in the prefrontal cortex, orbitofrontal cortex, cingulate cortex, and other serotonin-
Collectively these findings suggest that low serotonin activity helps produce aggressive feelings and impulsive behavior. In people who are clinically depressed, low serotonin activity may produce aggressive tendencies that cause them to be particularly vulnerable to suicidal thoughts and acts. Even in the absence of a depressive disorder, however, people with low serotonin activity may develop such aggressive feelings that they, too, are dangerous to themselves or to others. Still other research indicates that low serotonin activity combined with key psychosocial factors (such as childhood traumas) may be the strongest suicide predictor of all (Moberg et al., 2011).