Chapter 1. Eating Disorders
Synopsis
Eating Disorders
Author
Martina Marquez, Fresno City College
Catherine Robertson, Grossmont College
Synopsis
This activity introduces the three main types of eating disorders and outlines the signs and symptoms for each. These illnesses pose very serious health risks, and few who suffer with these diseases receive treatment. The slight bit of good news is that there are successful treatment plans that can help those who are seriously committed to their recovery.
REFERENCES
American Association of Suicidology. “Suicide and Eating Disorders.” Retrieved July 15, 2013 from http://freepdfdb.org/pdf/suicide-and-eating-disorders-85308342.html
American Psychological Association > Psychology Help Center > Eating Disorders
http://www.apa.org/helpcenter/eating.aspx
Anorexia Nervosa and Related Eating Disorders
http://www.anred.com
Brumberg, J. (1989). Fasting girls: The history of anorexia nervosa. Boston: Harvard University Press.
Claude-Pierre, P. (1998). The secret language of eating disorders. New York: Times Books/Random House.
Dounchis, J., Hayden, H., & Wilfey, D. (2001). Obesity body image and eating disorders in ethnically diverse children and adolescents. In J. L. Thompson & L. Smolak (Ed.), Body image, eating disorders and obesity in youth (pp. 67-98). Washington, D.C.: American Psychological Association.
Eating Disorders Coalition
http://www.eatingdisorderscoalition.org
Eating Disorder Hope
http://www.eatingdisorderhope.com
Healthy Place: America’s Mental Health Channel
http://www.healthyplace.com/eating-disorders/
Hoffman, L., & Rose, L. (April 6, 2005). Costly calories. Forbes. Retrieved August 24, 2005 from
http://www.forbes.com/home/health/2005/04/06/cx_lrlh_0406costlycalories.html
Martin, J. B. (2010). The Development of Ideal Body Image Perceptions in the United States. Nutrition Today, 45 (3), 98-100.
Retrieved from http://www.nursingcenter.com/pdf.asp?AID=1023485
Miller, M., & Pumariega, A. (2005). Eating disorders: Culture and eating disorders. HealthyPlace. Retrieved August 24, 2005 from http://www.healthyplace.com/Communities/Eating_Disorders/minorities_1.asp
Mirasol Recovery Centers
http://www.mirasol.net/eating-disorders/information/eating-disorder-statistics.php
Mitchell, J., & McCarthy, H. (2000). Eating disorders. In L. Champion & M. Power (Eds.). Adult psychological problems: An introduction (2nd ed., pp. 103-130). Hove, England: Psychology Press.
Nasser, M. (1997). Culture and weight consciousness. London/New York: Routledge.
National Association of Anorexia Nervosa and Associated Disorders, Inc.
http://www.anad.org/
National Eating Disorders Association
http://www.nationaleatingdisorders.org
National Institute of Mental Health > Health & Education > Mental Health Information > Eating Disorders
http://www.nimh.nih.gov/health/topics/eating-disorders/index.shtml#part4
Something Fishy Eating Disorders Online Website (2002). Cultural Issues. Retrieved August 30, 2005, from http://www.something-fishy.org/whatarethey/anorexia.php
Office on Women’s Health, U.S. Department of Health and Human Services > Body Image > Eating Disorders
http://www.womenshealth.gov/body-image/eating-disorders/index.html
Perriello, V. A. (2001). Aiming for healthy weight in wrestlers and other athletes. Contemporary Pediatrics, 18(9), 55-74.
South Carolina Department of Mental Health
http://www.state.sc.us/dmh/anorexia/statistics.htm
Steinhausen, H.C. (2009). "Outcomes of eating disorders." Child and Adolescent Psychiatric Clinics of North America, 18 (1): 225-242.
Tene, W. (1997). Not just a woman’s disease: Misconceptions of male eating disorders keep men from getting the help they need. Daily Sundial Online. Retrieved August 30, 2005.
The ABC’s of Eating Disorders
www.abceatingdisorders.com
email: info@abceatingdisorders.com
phone: 305-607-7169
Copyright 2005 Zakto Film
The Japan Times (January 27, 2002). Eating disorders claiming ever younger victims. Retrieved July 27, 2013, from http://www.japantimes.co.jp/community/2002/01/27/general/eating-disorders-claiming-ever-younger-victims/#.UfPZpGeyFuI
The Mayo Clinic: Eating disorders
http://www.mayoclinic.com/health/eating-disorders/DS00294
Thompson, R. A., & Sherman, R. T. (1993). Helping athletes with eating disorders. Champaign, IL: Human Kinetics Publishers.
Zerbe, K. (1995). The body betrayed. Carlsbad, CA: Gurze Books.
What are Eating Disorders?

As far back as medieval times, saints like Catherine of Siena fasted as an announcement of spirituality. During Victorian times, women fasted as a protest against societal rules. Anorexia has been a known disorder since the late 19th century (Brumberg, 1989). Even so, beginning in the 1950s, it became a recognized diagnosis. Bulimia was first identified in 1979 (Miller, Pumeriega, 2005).
Eating disorders are complex conditions that have severe mental and physical health aspects. While these diseases most obviously manifest in the body, eating disorders are, in fact, mental illnesses that are outlined in the Diagnostic and Statistical Manual of Mental Disorders (DSM), which is the premier reference manual used by medical, healthcare, and health policy professionals in the U.S. There are three main types of eating disorders: anorexia nervosa, bulimia nervosa, and binge eating disorder. Eating disorder not otherwise specified is a catchall category that describes an eating disorder characterized by any combination of symptoms from the three main types while not meeting any single classification.
Types of Eating Disorders

Anorexia nervosa (also called anorexia) is literally self-imposed starvation that yields a body weight that is 85% of what is healthy for a particular age and height. Severe restriction of caloric intake and/or excessive exercise in order to burn vast quantities of calories often result in a dangerously thin individual. Anorexics commonly suffer from a distorted body image that reinforces their behaviors. They continue to see themselves as overweight in spite of their alarmingly thin reality.
Bulimia nervosa (also called bulimia) is defined by bouts of bingeing, or excessive, uncontrollable eating, followed by purging. Because feelings of being out of control accompany bingeing, bulimics compensate for their excess with purging behaviors, such as abuse of laxatives, self-induced vomiting, excessive exercise, and/or even fasting, which may help them to feel as if an element of control is being restored. The cycle continues as the bingeing becomes recurrent and repeated behavior. While bulimics may demonstrate some of the same behaviors that anorexics do, bulimics may be underweight, normal weight, or overweight because purging is not generally a successful method for losing weight.
Binge eating disorder (BED) is the newest of eating disorders. Insatiable cravings lead to bingeing. Like bulimics, the binges of those with BED may be prompted by stress, poor body image, low self-esteem, and/or other dysfunctional thoughts, but unlike bulimics, those with BED do not purge. Therefore, those with BED are generally overweight or obese.
Eating disorder not otherwise specified is a descriptor for abnormal, unhealthy eating disorders that may include some but not all of the criteria for a specific diagnosis of the three illnesses described above.
Signs and Symptoms of Anorexia
Some clinical symptoms of anorexia nervosa include:
– being at least 15% below ideal body weight accompanied by a refusal to maintain a weight that is at or above a normal body weight for height and age;
– intense fear of being fat or gaining weight;
– having a body image distortion that causes the anorexic to see self as overweight even if that is not at all the case;
– loss of at least 3 menstrual periods in women;
– growth of a downy layer of hair called lanugo, which is the body’s effort to keep itself warm.
Some behavioral signs that accompany anorexia include:
– restricting whole categories of foods, such as fats or carbohydrates, or developing food rituals, like eating foods in a certain order;
– denying hunger;
– making excuses to avoid meals;
– obsessing about control of weight and control of food;
– withdrawing from normal activities and avoiding friends and family;
– abusing laxatives and/or diet pills;
– excessive and obsessive exercising.
Meet Stephanie. Observe her to see if she demonstrates any of these symptoms and signs of anorexia.
Signs and Symptoms of Bulimia
Some clinical symptoms of bulimia nervosa include:
– binge eating large quantities of food in a short time frame accompanied by the feeling that one cannot stop eating;
– purging, such as self-induced vomiting, abusing laxatives, fasting, or exercising excessively, that follows the bingeing as perhaps a way to compensate for the bingeing;
– bingeing/purging cycle that occurs more than twice a week for at least 3 months;
– self-esteem that is too dependent upon body image.
Some physical and behavioral signs that accompany bulimia include:
– stained teeth, calluses on knuckles or hand, swelling of jaw area, broken blood vessels in eye from self-inducing vomiting;
– a rigid exercise routine that may appear excessive or obsessive;
– frequent trips to the bathroom after meals;
– abuse of laxatives and/or diet pills.
A special note: It may be difficult to identify those who suffer from bulimia because they may not necessarily demonstrate dramatic weight loss. For example, some bulimics may be within 10 pounds of their normal weight range.
Meet Rick. Observe him to see if he demonstrates any of these symptoms and signs of bulimia.
Signs and Symptoms of Binge Eating Disorder

Some clinical symptoms of binge eating disorder include:
– out-of-control eating;
– significant distress over binge eating;
– binge episodes that occur 1 or more times per week for 3 months or more.
Some behavioral signs that accompany binge eating disorder include:
– choosing to eat alone;
– lying about the amount of food eaten;
– hiding stashes of food in the house, at the office, or in the car.
Eating Disorder Statistics
Because of the secrecy inherent to eating disorders, many statistics available are simply educated estimates. An aspect of eating disorders is the desire to hide the illness from others in order to be able to continue the disordered behavior, and as a result, many eating disorders are not always obvious to family and friends. Therefore, those with eating disorders do not always receive or seek treatment. Often eating disorders accompany other health or mental conditions that may get treated while the eating disorder may get overlooked. All of these nuances mean that those with eating disorders are not ones to stand up and be counted easily or willingly. Statistically, only 1 in 10 men and women with eating disorders receives treatment. Furthermore, treating physicians are not required to report eating disorders to any health agency, yet another reason why statistics are difficult to obtain.
The National Eating Disorders Association cites that 20 million women and 10 million men in the U.S. have suffered from an eating disorder at some point in their lives. Estimates on how many in the U.S. actually have eating disorders vary quite a bit from 8 million according to the South Carolina Department of Mental Health to 11 million according to the Eating Disorders Coalition. According to The National Association of Anorexia Nervosa and Associated Disorders, up to 24 million are “affected by” eating disorders, and this figure may include those with the illness, family, friends, classmates, teachers, teammates, therapists, and anyone in relationship with those with eating disorders.
While this wide range of estimates is characteristic of how difficult it is to measure the number of individuals with these diseases, trends do reveal that the rate of incidence of new cases of eating disorders has been increasing regularly since 1950. Today’s culture of diets, weight loss, and thinness is surely a major contributing factor to the rise in eating disorders. To give an idea of the misrepresented body image being peddled by U.S. media, the female body type that is promoted in advertising as the ideal appears naturally in only 5% of U.S. women according to the National Association of Anorexia Nervosa and Associated Disorders. As an example of the impact of this distorted, media-promoted body image in the U.S., a study revealed that 69% of U.S. elementary school girls say that photos in magazines influence their concept of an ideal body image and that 47% of U.S. elementary school girls say that these same photos make them want to lose weight (Martin 2010). These are young girls feeling this influence!
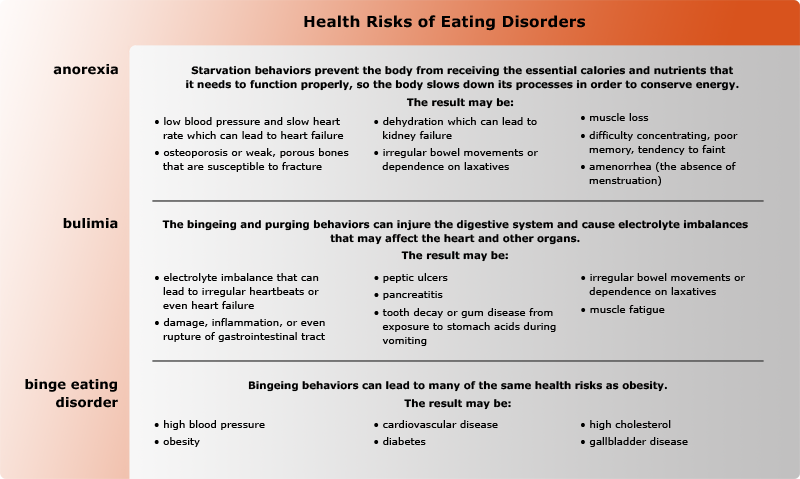
Health Risks of Eating Disorders

While eating disorders are likely to accompany other mental illnesses, such as depression, anxiety disorders, obsessive-compulsive disorder, and even substance abuse problems, there are serious physical health risks that result from the starving, fasting, bingeing, and purging behaviors of eating disorders.
Mortality and Eating Disorders
Death is a real risk of having an eating disorder. Research has found that eating disorders demonstrate the highest mortality rate of any mental illness. One study found that the mortality rate among anorexics is 18 times higher than among their peers without eating disorders. Eating disorders pose severe mental and physical health risks. For example, 20% of anorexics die prematurely from complications of their disorders. Suicide is a major cause of death among those with eating disorders. Anorexics and bulimics are 23 times more likely than the general population to commit suicide. This rate of suicide is among the highest of all mental illnesses. Since 95% of those suffering with eating disorders are between 16 and 25 years old, these young adults and adolescents may even be more susceptible to the physical and mental aspects of these illnesses since they are severely taxing bodies and minds that may not have finished developing. The mental and physical consequences of these diseases make them extremely dangerous.
Meet Isabelle Caro, a French actress and model. She has suffered from anorexia for about 12 years. In spite of the hope and thoughts of the future that she alludes to throughout the interview, she passed away 3 years after this interview at the age of 28.
Who is At Risk for Eating Disorders?

Generally, eating disorders appear in teens and young adults between the ages of 12 and 25 although they can develop later as well. Mostly girls and women are likely to suffer from eating disorders, but men with eating disorders are growing in numbers. Five to fifteen percent of those with anorexia or bulimia are male. One quarter of the preadolescent cases of anorexia is boys. There are about an equal number of men and women who struggle with binge eating disorder. There seems to be no gender, ethnicity, or socioeconomic group immune to these illnesses.
Those prone to eating disorders tend to:
– diet;
– live in societies (like the U.S.) that value being thin;
– have low self-esteem;
– have high self-expectations;
– have family history of eating disorders and/or of being overly concerned with appearance or dieting;
– have characteristics determined by genes, or a genetic predisposition, toward eating disorders;
– have trouble expressing their emotions;
– have a preoccupation with weight;
– have other emotional disorders (like depression, anxiety, obsessive-compulsive disorder) or substance abuse problems;
– maintain a distorted sense of own body image;
– participate in weight-conscious sports or careers (gymnasts, ice skaters, wrestlers, dancers, runners, jockeys, actors/actresses, models);
– be compulsive, impulsive, and/or perfectionistic;
– be dissatisfied with own appearance;
– be victims of teasing or bullying about body size or shape;
– be victims of trauma, abuse, and/or sexual trauma.
Please note that this is not a checklist of the qualities of individuals who are going to get eating disorders. However, these characteristics do represent some themes and commonalities among those who do suffer from these illnesses.
1.
Even though we do not know the complete stories behind the eating disorders of Stephanie or Rick, do you see any of these characteristics or qualities? Select either Stephanie or Rick and compare his/her story to this list. Refer to specific details from the videos to support your answer.
Treatment for Eating Disorders
Unfortunately, those with eating disorders are often reluctant to seek treatment. Statistics cite that only 1 in 10 people with eating disorders receives treatment. Men with eating disorders are the least likely to pursue treatment because of the stereotype of having a “women’s” illness. The good news is that eating disorders are treatable. The overall treatment goals for eating disorders are:
to get to and maintain a healthy body weight;
to explore and help alleviate the emotional issues that contribute to the disorder;
to investigate and hopefully eliminate the bad behaviors surrounding food.
There is no one single treatment plan for eating disorders. The greatest chance of success occurs with a treatment that is customized to the individual and his/her emotional and physical needs. There is quite an array of treatment tools available from which to design specialized treatment programs for those with eating disorders. Successful therapeutic methods for eating disorders include some, if not all, of the following:
– medication (antidepressants, antipsychotics, mood stabilizers);
– individual cognitive therapy (also called “talk therapy”) to work on improving thoughts, attitudes, behaviors, to develop a positive body image and a healthy relationship with food and eating;
– family or marital counseling to work with other members of the household;
– group therapy;
– nutritional education to learn how to nourish the body properly.
Successful and professional treatment is not a quick process. It can take months or years and may be inpatient, outpatient, or include components of both. No matter where it takes place, treatment is most likely to succeed when being administered by skilled, accredited clinicians with experience treating eating disorder patients. Early intervention is best. The earlier that the eating disorder sufferer gets into treatment, the greater the chance is of recovery.
In spite of the benefits of these methods, relapses do occur, and patients do drop out of treatment programs for various reasons, such as financial hardship, lack of insurance coverage, relapse, or lack of support from family, friends, or employers. Research demonstrates that those who commit to their treatment and who put in time and energy to get better do recover and can stay recovered.
Listen to the recovery prospects for Stephanie, Rick, and Dave. What do you think the likelihood is that they will recover and stay recovered?
Assessment: Check Your Understanding
2.
1. Eating disorders are relatively new phenomena.
Assessment: Check Your Understanding
3.
2. Which of the following statements is FALSE?
Assessment: Check Your Understanding

4.
3. Which of the following is NOT one of the recommendations for a successful treatment program for eating disorders?
Assessment: Check Your Understanding
5.
4. Based on what you have learned about eating disorders, explain four ideas for a school-based prevention program or curriculum. How would you recommend that this curriculum be implemented for maximum effect?
Congratulations! You have completed this activity.Total Score: x out of x points (x%) You have received a provisional score for your essay answers, which have been submitted to your instructor.