11.1 Physical Development
Human development begins with conception, progresses for 9 months in the protection of the womb, and continues after birth when infants face a radically different environment—one in which they must eat, drink, deal with an amazing number of sights and sounds, and interact with other members of their own species. In this section, we take a brief look at prenatal development, followed by an examination of postnatal growth, focusing on another period of dramatic development in the course of the life span: puberty and adolescence.
Prenatal Development
Humans, as all mammals, are a sexually reproducing species, requiring the joining of male sperm with a female egg to begin a new life. Women typically release one egg (ovum) from one of their ovaries each month, whereas men release approximately 250 million sperm in each ejaculation (Baker & Bellis, 2007). Only one of these many millions of sperm, however, will impregnate the egg, and this will occur in the fallopian tube, which connects the ovaries to the uterus, or womb.
Zygotic, Embryonic, and Fetal Phases
1
What are the three phases of prenatal development? What are the major accomplishments of each phase?
The prenatal period is conventionally divided into three phases: the zygotic (or germinal), embryonic, and fetal phases. When sperm joins egg, combining 23 nuclear genes from the mother with 23 from the father (review the basics of genetics in Chapter 3), the zygote begins its journey to the uterus. During this time, which last about 2 weeks, the zygote divides many times, eventually implanting in the uterine wall, ending the zygotic phase and beginning the embryonic phase. We should note that it is estimated that 40 percent of zygotes do not survive this earliest phase of prenatal development, and as many as onethird of those that do become implanted are lost in later phases by spontaneous abortions, also known as miscarriages (O’Rahilly, & Müller, 2001).
415
The embryonic period extends from the third to about the eighth week after conception. During this time, all major organ systems develop. The embryo receives nutrition from the mother’s bloodstream via the umbilical cord through the placenta, which develops inside the uterus during pregnancy. The placenta also exchanges oxygen, antibodies, and wastes between the mother and embryo.
The final phase of the prenatal period, the fetal, extends from about 9 weeks until birth, which usually takes place about 38 weeks after conception. The most prominent feature of the fetal period is growth and refinement of organs and body structure. At 3 months, the fetus is about 2.5 inches long and weighs about half an ounce. Six months later, at birth, the average newborn is about 20 inches long and weighs about 7.5 pounds. The fetus also changes in proportion. The head of the fetus at 9 weeks is proportionally large relative to the rest of the body, and this decreases, with the body catching up, so to speak, by the time a baby is born. However, even at birth, an infant’s head accounts for about 20 percent of its body. In comparison, the head is about only 12 percent of the body of the average adult (Tanner, 1990). This change in proportions, with development progressing essentially from head to foot, is termed cephalocaudal development.
By the end of the 12th week after conception, all the organs are formed, though not functioning well, and are in same proportion to each other as in a fullterm newborn, just smaller. The external genitalia begin to differentiate between males and females around the 9th week but are not fully formed until about the 12th week. As early as the 8th week, the embryo begins to move, and activity increases by 12 weeks. The mother may be able to detect some of these movements, although most mothers don’t feel the baby move until the 4th or 5th month of pregnancy (Fifer, 2005).
Fetuses “behave” and are able to perceive some stimuli. For example, ultrasounds reveal that some fetuses suck their thumbs and respond to touch. By 6 months, fetuses respond to their mothers’ heartbeat and sounds from outside the womb, including language. In fact, research has shown that infants show a preference for their mothers’ voices immediately after birth, an indication that their auditory system is functioning reasonably well before birth (DeCasper & Fifer, 1980; Kisilevsky et al., 2003).

MedicalRF/Science Source
416
The Effects of Experience During the Prenatal Period
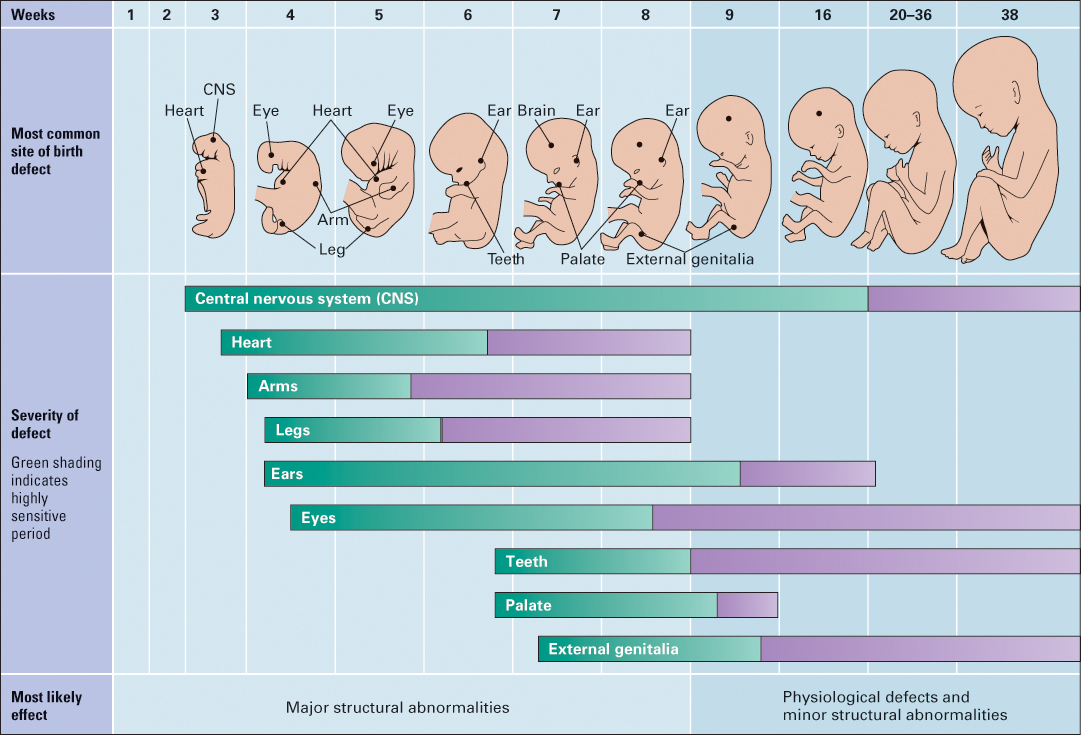
Although embryos and fetuses are sheltered from the outside world, they are nonetheless subject to the effects of experience. The types of experience that researchers have most thoroughly studied are the effects of teratogens, environmental agents that cause harm during prenatal development (see Figure 11.1). Most teratogens are in the form of substances that get into the embryo’s or fetus’s system from the mother through the umbilical cord. These include both legal and illegal drugs, including marijuana, cocaine, and heroin, and prescription drugs such as antibiotics, antidepressants, and sex hormones; as well as alcohol and tobacco—substances that a pregnant woman may not think of as “drugs.” The developing embryo or fetus can also be harmed by diseases, such as AIDS, rubella (German measles), and herpes simplex; and by environmental pollutants, such as mercury, lead, and nicotine (from second-hand smoke).
2
When is the unborn child most susceptible to the effects of teratogens, and why?
A teratogen’s potential effect on prenatal development depends on how early or late in pregnancy the exposure occurs. Recall that development of organ systems is most rapid during the embryonic period, between the 3rd and 8th weeks after conception. This is the time when an agent can most substantially alter the course of development; it may, for example, prevent an organ from developing properly, or fingers and toes from forming. Once an organ such as the kidney or hands or feet has been developed, exposure to a potential teratogen will have little or no effect on future development. This was dramatically illustrated by the drug thalidomide, which was prescribed to some women in Europe and Asia in the early 1960s to combat morning sickness. (Thalidomide was not approved for use in the United States.) When women took thalidomide during the first 8 weeks of pregnancy, the result was often babies born with deformed limbs, as well as damage to other organ systems. The drug interfered with the development of limb formation and hands and feet. However, these deformations were not found in babies born to women who took the drug later in pregnancy, after limbs and their appendages had already been developed.
417
3
How might prenatal experience “prepare” a fetus for postnatal life?
It is not just teratogens that embryos and fetuses respond to, but other aspects of experience, such as nutrition and maternal stress. For example, we noted in Chapter 6 that women with poor diets during pregnancy tend to have low-birth-weight infants who then grow to become overweight or obese during childhood. These babies developed “thrifty phenotypes,” storing more fat than children whose prenatal diets were more nutritious. In other situations, children who were prenatally exposed to high levels of stress hormones show higher anxiety and fearfulness, temperamental difficulty, impulsivity, reduced executive functions, impaired attention, higher aggression, and risk taking (Glover, 2011; Pluess & Belsky, 2011). Although these can all be viewed as negative consequences of prenatal stress, some of these characteristics (for example, high levels of aggression and risk taking) may be well suited for children growing up in high-stress environments. Along these lines, Marco Del Giudice (2012) suggests, “The developing fetus can use this information as a ‘forecast’ of the environmental conditions it will eventually face after birth, and start adjusting its physiological and behavioral profile to match the requirements of the world it will probably encounter” (p. 1615).
Infancy, roughly the first 18 to 24 months after birth, is the time of most rapid developmental change, change that lays the foundation for further development. Human infants are born especially immature in comparison to other primates, in large part because of their big brains. If prenatal development lasted much longer, a newborn’s brain would be too large to fit through the birth canal. This means that much brain development that occurs prenatally in other primates occurs after birth in humans. But before we discuss how infants learn about the world into which they emerge, let’s look at physical development after birth, focusing on another period of dramatic physical development—puberty and adolescence.
Physical Development: Puberty and Adolescence
4
To what extent do different parts of the body develop at different rates?
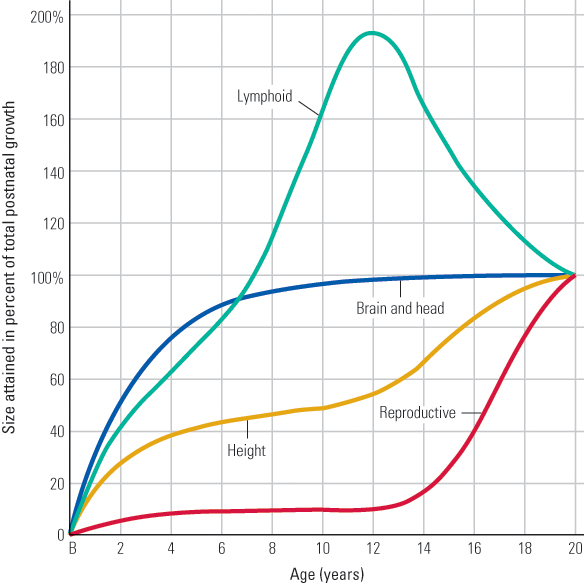
When we think of physical growth, we think of body height and weight, and people certainly get taller and heavier with age. It is not difficult to observe that body growth is relatively rapid during infancy and the preschool years, becomes more gradual over childhood, and accelerates in adolescence. However, there are other parts of the body that are less obviously visible, and they develop at different rates than height, as shown in Figure 11.2. As you can see, the curve for height displays the pattern we just described, but the head and brain grow rapidly over the first 5 or 6 years and approach adult levels by age 10. The lymphoid system, which includes the thymus and lymph glands, develops rapidly early in life, greatly exceeding adult dimensions by about age 12, and just as rapidly decreases over adolescence. At the bottom of the graph is the reproductive system, which shows little growth until adolescence.
418

It is this dramatic upswing in reproductive development that characterizes some of the most studied changes in physical development—those that occur with the onset of puberty. Puberty refers to the developmental stage leading up to adolescence when glands associated with the reproductive system begin to enlarge, bringing about changes in physical appearance and behavior. Increases in hormones in both males (androgens, especially testosterone) and females (estrogens and progesterone) contribute to changes in physical stature (adolescent growth spurt, which typically begins about a year earlier in girls than boys), reproductive ability (the production of sperm in males and viable eggs in females), and emotions and behavior related to sexual attraction.
Puberty does not happen all at once, but is actually a series of related events, typically spanning 4 or 5 years. For example, in females, initial breast development begins at about 11 years and is mostly completed by 15 or 16 years. A girl’s first menstrual period (termed menarche) typically occurs about 13 years of age, although many girls do not become fertile (able to conceive a child) until about age 15 or 16 because eggs are not always produced in the first 2 or 3 years of menstrual cycles. A girl’s growth spurt starts around age 12, with skeletal growth being complete between 14 and 15 years of age. Similarly, for boys, testes begin to increase in size between 11 and 12 years of age, and the penis increases in size beginning about 13 years, shortly before the male adolescent growth spurt begins. Boys typically have their first nocturnal emission at 14 and develop facial hair between the ages of 15 and 16 (Tanner, 1990). The male voice change begins on average at about age 13, and by age 15 most boys have developed their adult male voice.
419
5
How has the emergence of different aspects of puberty changed over historical time? What is responsible for these changes?
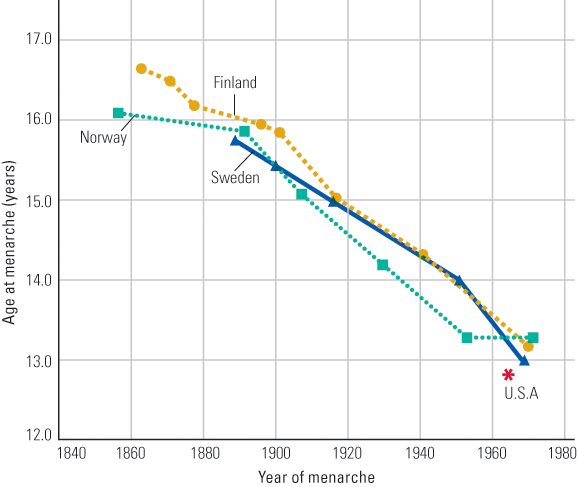
These are all average age-of-attainment values, of course, with individual boys and girls showing very wide variation. Nevertheless, on average, the age of menarche has shown substantial decreases over recent historical times. This is illustrated in Figure 11.3, which shows the average age of menarche in three European countries over the past 150 years or so, along with the average age in the United States around 1965. As you can see, there was a steady decline in the average age of menarche from 1860 to about 1960 (Tanner, 1990). This trend is generally attributed to better nutrition, and indeed, today girls who are overweight attain menarche sooner than other girls, and diet may be associated with other signs of earlier puberty. However, the average age of menarche has not changed substantially in the last 50 years or so. In the United States today, the average age of menarche is 12.6 years for Caucasian females and 12.1 years for African-American females (Steingraber, 2007).
Other pubertal events continue to change over time, most notably breast development. This is clearly shown in a large-scale study conducted by Marcia Herman-Giddens and her colleagues (1997), who studied pubertal development in more than 17,000 girls in the United States between the ages of 3 and 12 years of age. They reported that although the age of menarche remained unchanged since the 1950s, the average age of breast development and presence of pubic hair continues to decline. For example, they found that the average age for breast development was 9.96 years for white girls and 8.87 years for African-American girls, with some girls (1 percent of white girls and 3 percent of African-American girls) showing signs of breast development as early as age 3. Researchers have identified several candidates for the cause of this accelerated development, including exposure to passive tobacco smoke, insecticides, arsenic, polybrominated biphenyls (a fire retardant), and chemicals used in common plastics (Blanck et al., 2000; Herman-Giddens et al., 1997). However, as with menarche, hormonal changes associated with obesity are the top potential cause of early breast development.
SECTION REVIEW
Physical development is perhaps most dramatic during the prenatal and pubescent stages of life.
Prenatal development
- The prenatal period is divided into three phases: the zygotic (or germinal), the embryonic, and the fetal.
- Development is most rapid in the head region, with the rest of the body catching up in size later; this is termed cephalocaudal development.
- The embryonic phase is the time when the effects of teratogens are apt to be most severe because major organ systems are being formed during this time.
- Other prenatal experiences, such as the availability of nutrition, seem to prepare the fetus for postnatal life.
Physical Development: Puberty and Adolescence
- Different body systems show different patterns of change from infancy to adulthood.
- Major changes in physical development occur at puberty, with different aspects of puberty for both boys and girls occurring at different times.
- Average age of menarche decreased from the mid-1800s to about 1960 and has remained stable since. Breast growth and other aspects of pubertal development have accelerated in recent decades, with obesity being a major cause.
420