Chapter 1. MUSCULAR SYSTEM
Objectives
After completing this unit, you should be able to:
- Define origin, insertion, agonist, synergist, and antagonist and explain how muscles move the skeleton. Explain how muscles are named. Group the major muscles of the body and identify the actions of these muscles.
- Identify the microscopic structures of muscle fiber and describe the structure of myofibrils. Describe the sliding filament theory of muscular contraction and explain the length-tension relationship of skeletal muscle.
- Explain the process of excitation-contraction coupling and identify the role of calcium in development of the muscle contraction. Describe a motor unit and explain tetanic contraction and recruitment.
- Describe the ATP energy sources for muscular contraction (creatine phosphate, anaerobic and aerobic metabolism). Describe the cause of muscle fatigue.
Muscular System Organization
There are three types of muscle tissue found throughout the body: skeletal, cardiac, and smooth. The primary function of muscle tissue is to contract, and allow for movement. This chapter focuses on skeletal muscle which is found attached to the skeleton, and is primarily under voluntary control. This means that we get to choose when skeletal muscle contracts. The main function of skeletal muscle is to pull on bones or skin to allow for body movement. However, skeletal muscle also aids in increasing the stability of joints. Tension in our skeletal muscle is important in maintaining body posture. Without having some muscles contracted, you could not sit upright in a chair. The muscular system also plays an important role in maintaining homeostasis with regard to body temperature. Contraction of skeletal muscle releases heat that is used to maintain our body temperature.
Muscular System Organization
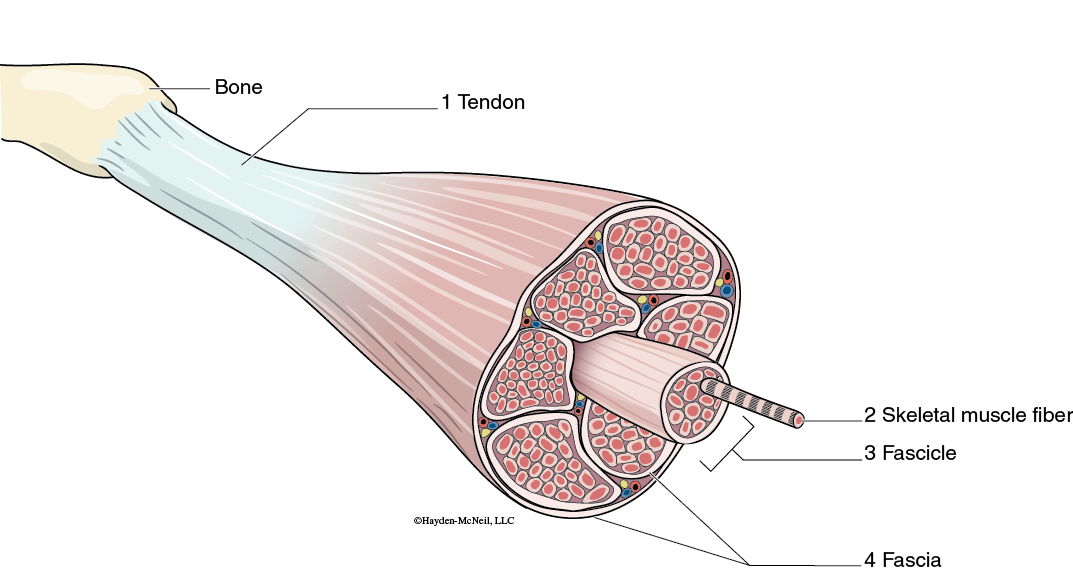
A single muscle is actually made up of many long, tube-shaped cells known as skeletal muscle fibers. Surrounding each muscle is a layer of connective tissue known as fascia. The fascia can extend beyond the bulk of the muscle to form tendons. Tendons attach muscle to the periosteum of bone.
Muscular System Organization
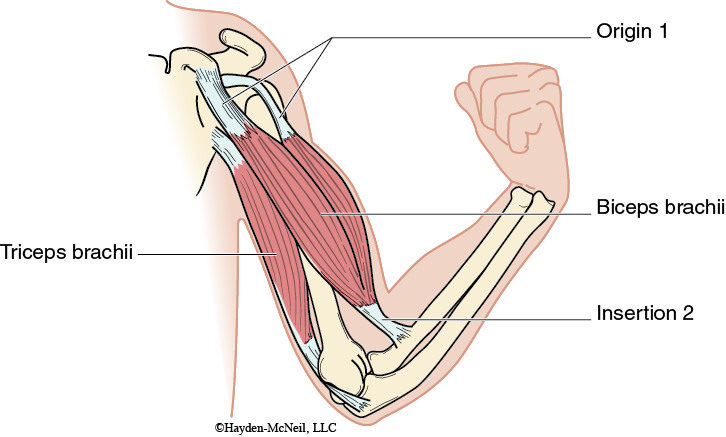
Each muscle has an origin and an insertion. These terms refer to what structures the muscle is attached to. The origin is the attachment of the muscle that remains stationary, whereas the insertion is the attachment where movement occurs. When a skeletal muscle contracts, the insertion is pulled toward the origin. The action of a muscle refers to what movement the muscle causes. With any action, there are muscles that promote that movement known as agonistic muscles, and muscles that oppose or resist that movement known as antagonistic muscles. When any movement occurs, the agonistic muscles for that movement contract and antagonistic muscles relax.
Skeletal Muscle Identification
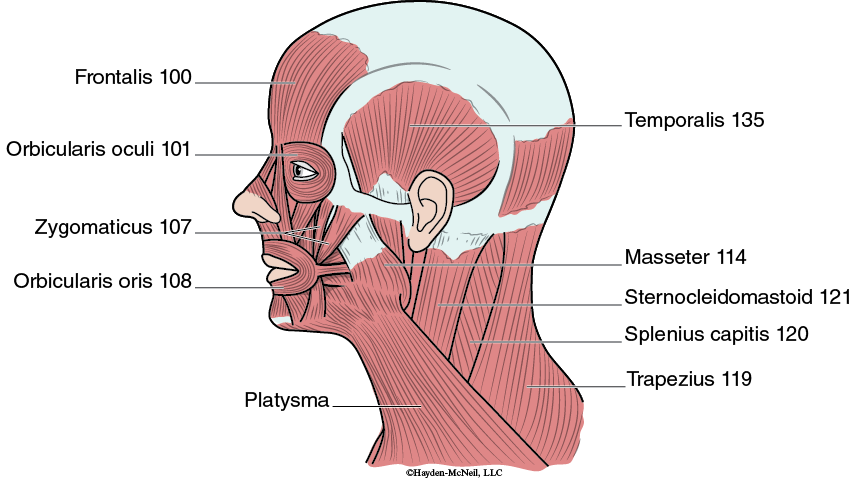
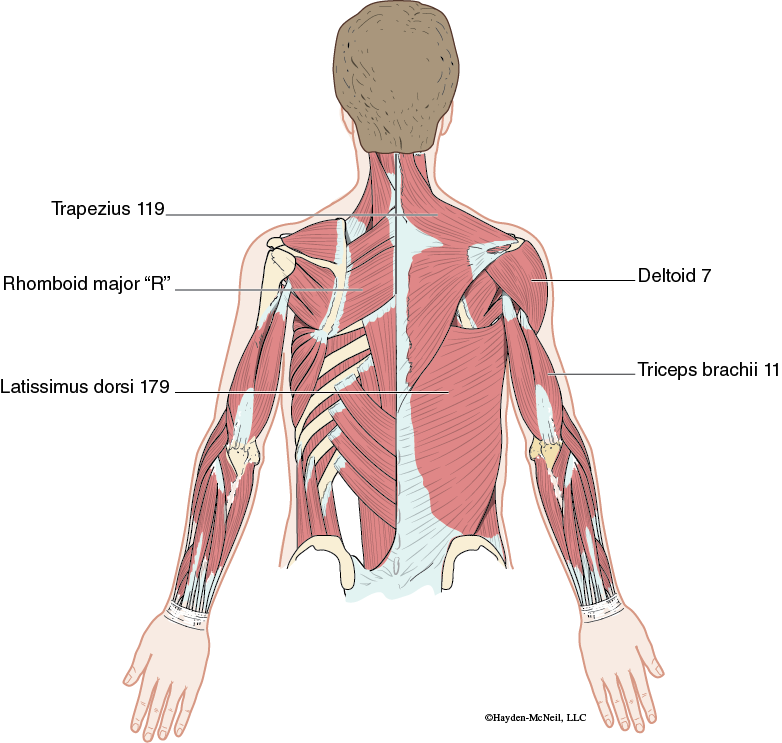
A variety of criteria have been used in naming muscles. Understanding these criteria will make it easier to remember the names of muscles and correctly identify them. The name of many muscles reflects their location in the body. An example of this is the frontalis muscle which gets its name for its location on the forehead and can be found overlying the frontal bone of the skull. Other muscles are named for their general shape. The left and right trapezius muscles of the upper back together form the shape of a diamond or trapezoid. Muscles can also be named for the action or movement that they cause. An example of this is the supinator, which gets its name for its action of supinating the forearm. Many of the muscles you will be learning in this chapter are named for their origin or insertion. The sternocleidomastoid muscle gets its name for its two origins on the sternum and clavicle, and its insertion on the mastoid process of the skull. The biceps brachii and triceps brachii get their names for the number of origins each has. The biceps brachii has two origins in the shoulder, and the triceps brachii has three. Parts of muscle names often reflect their relative size compared to other muscles in that region. For example, the gluteus maximus muscle gets the name maximus because it is the largest of the muscles in the gluteal region. Finally, in this chapter you will learn several muscles that get their name in part because of the direction that the muscle fibers or fascicles travel. Muscle fibers in the rectus abdominis muscle run straight up and down (rectus=straight), whereas fibers in the external oblique muscles run diagonally (oblique=at an angle).
Muscles of the Head
Facial Muscles
The facial muscles are unique in that they have origins on bone, but insertions on the skin of the face or other muscles. The facial muscles contract to cause a variety of facial expressions from surprise (frontalis), winking (orbicularis oculi), smiling (zygomaticus), puckering (orbicularis oris), or pouting (platysma).
Muscles of Mastication
The muscles of mastication move the lower jaw at the temporomandibular joint (TMJ) for chewing and speech. The masseter and temporalis muscles both work to close the jaw. The masseter pulls on the angle of the lower jaw, and is the stronger of the two. The temporalis works to both close the jaw and retract the mandible.
Muscles of Head Movement
Balance and movement of the head are primarily controlled by two pairs of muscles named the sternocleidomastoid and splenius capitis. The sternocleidomastoid muscle bends the head forward, and can assist in rotating the head toward the shoulder. The splenius capitis muscles extend or bend the head backwards, and also assist in rotating the head.
Muscles of Ventilation
The diaphragm is the major muscle of respiration. When it contracts, it moves downwards into the abdominal cavity. This increases the volume of the thoracic cavity, and allows air to enter the lungs.
Abdominal Muscles
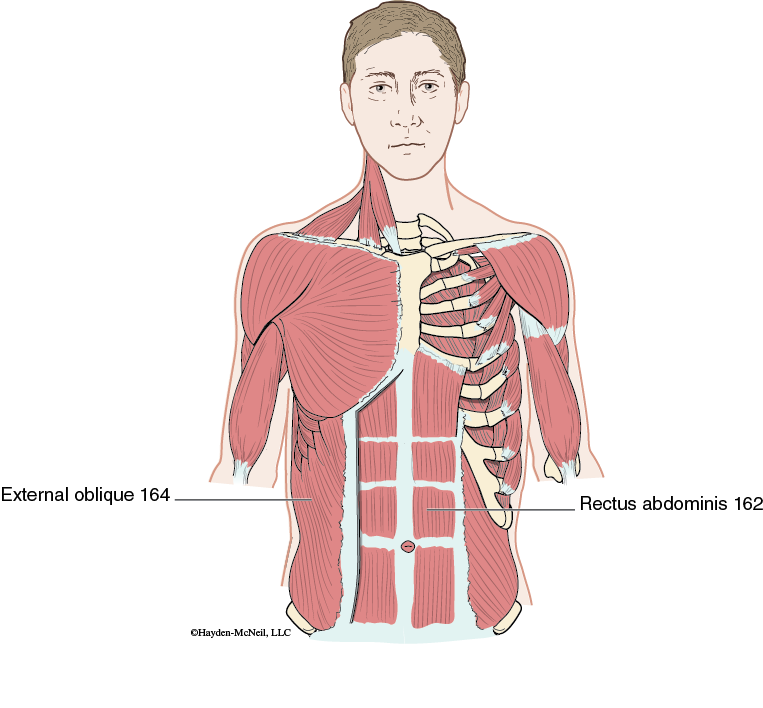
Muscles of the abdominal wall act to protect and compress the contents of the abdominal cavity, and rotate and flex the trunk. Abdominal muscles can also aid in defecation, childbirth, forced exhalation, vomiting, coughing, and screaming. The external oblique is the outermost muscle, and is located on the sides of the abdomen, while the rectus abdominis muscle is located in the center forming the “six-pack” muscle.
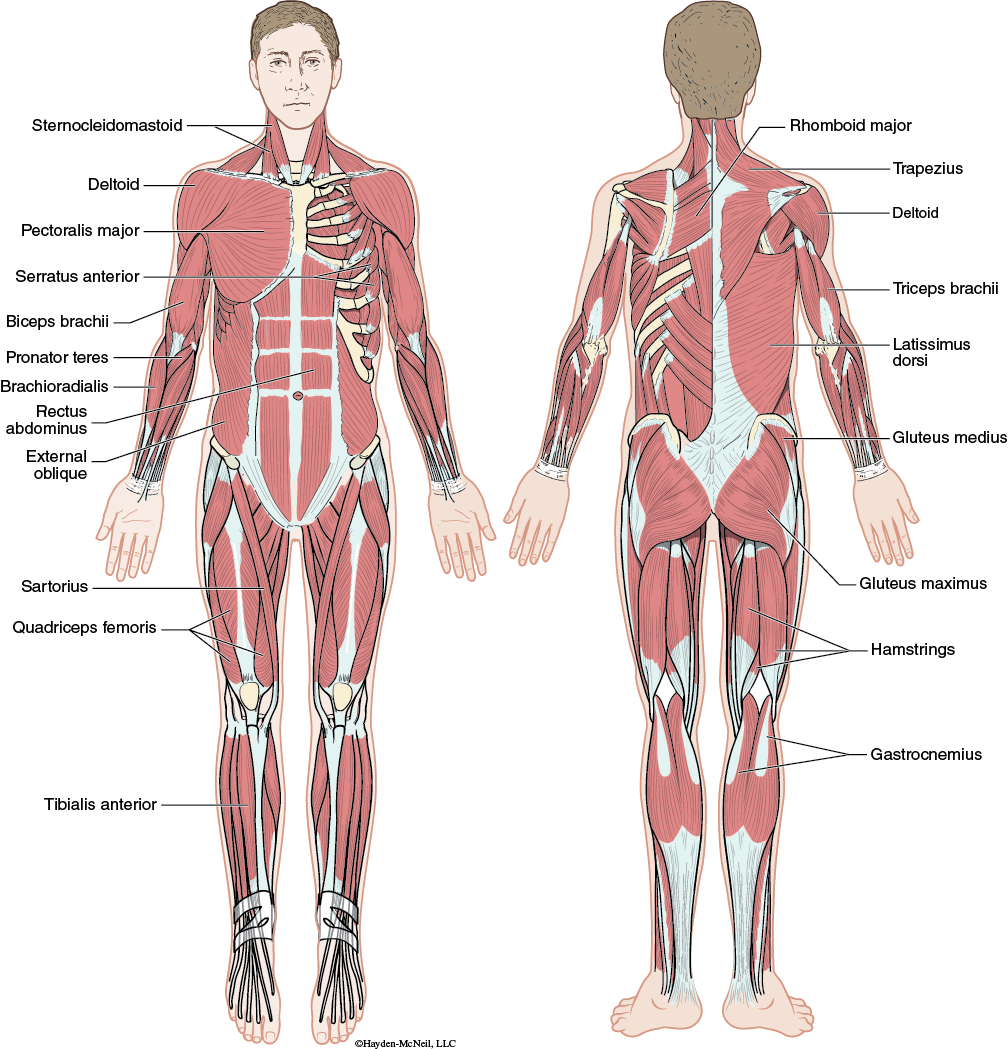
Muscles of Upper Limb Movement
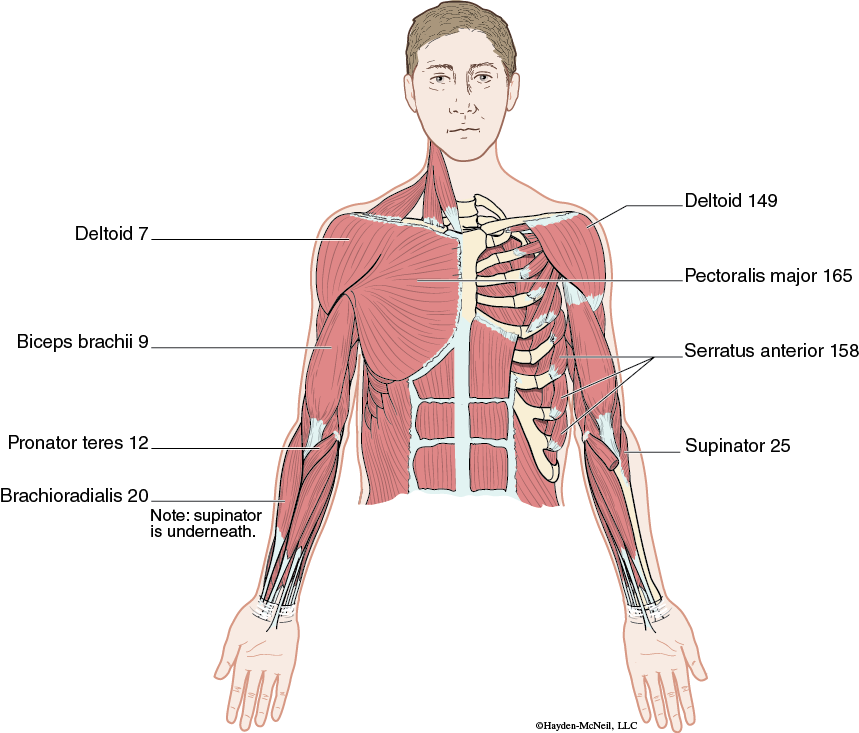
The following muscles are associated with the pectoral girdle and the upper limbs. These muscles work to stabilize or move the scapula (trapezius, rhomboid major, serratus anterior), move the arm (pectoralis major, latissimus dorsi, and deltoid), stabilize the shoulder joint (rotator cuff muscles), move the elbow joint (biceps brachii, brachioradialis, and triceps brachii), or rotate the lower arm (pronator teres and supinator).
Muscles of Lower Limb Movement
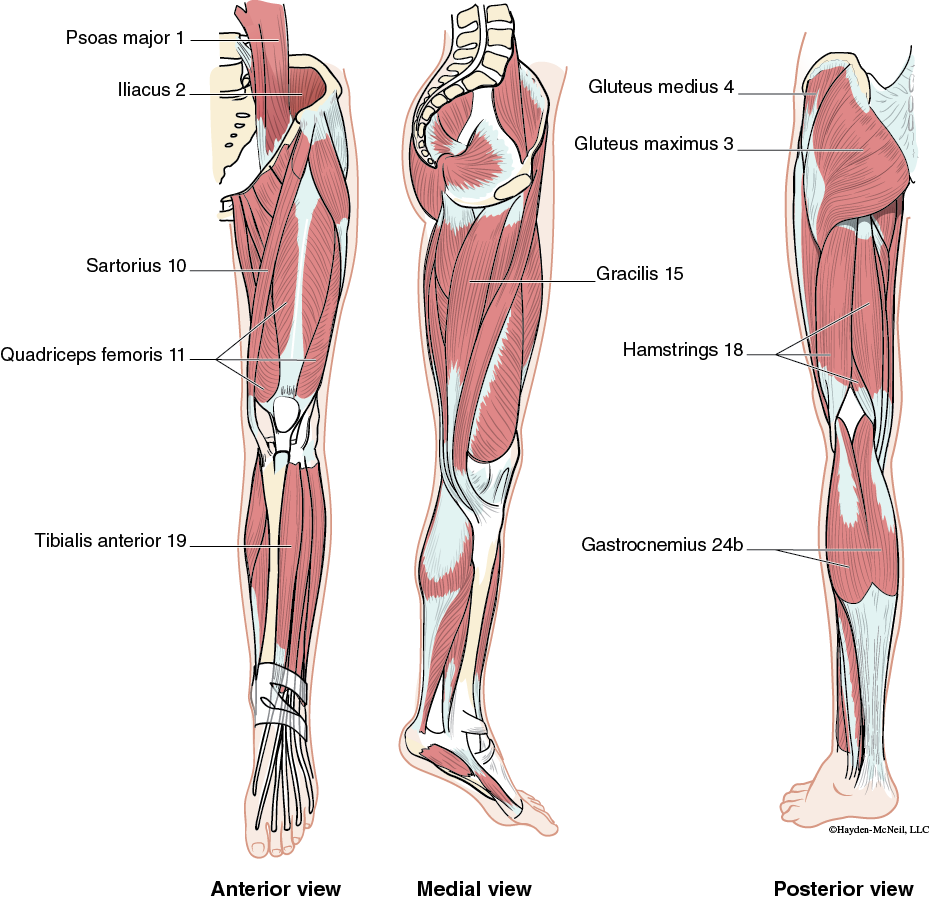
The muscles that move the lower limb are associated with the pelvic girdle and bones of the lower limb. Several of these muscles work to flex, extend, abduct, adduct, and rotate the thigh (psoas major, iliacus, gracilis, gluteus maximus, and gluteus medius). Others aid in rotating the leg, and flexing and extending the knee (quadriceps femoris, sartorius, and hamstrings). Finally muscles of the lower limb can be used to move the ankle and foot (tibialis anterior, and gastrocnemius).
Muscle Characteristics
Skeletal muscle cells are known as muscle fibers. The fibers are very long and cylindrical in shape. Muscle fibers are multinucleated because they form from indivial cells that fuse together during development. The plasma membrane of the newly formed muscle fiber is called the sarcolemma. The filaments found within skeletal muscle fibers are arranged in a specific pattern that leads to a striped or striated appearance when examined under the microscope.
Skeletal muscle is the only muscle type in the human body that is under voluntary control. When we choose to contract a muscle, a signal from our brain travels down a motor neuron to the muscle fiber. The signal triggers an electrical impulse that travels along the entire muscle fiber, a characteristic of skeletal muscle known as excitability. Once stimulated, the tension in the muscle will increase resulting in muscle contraction. The skeletal muscle characteristic contractility refers to the fact that the muscle cell physically shortens once stimulated by a neuron.
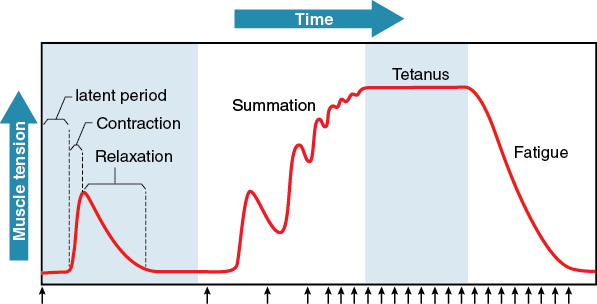
The response of a motor unit to the signal of a motor neuron is known as a muscle twitch. A muscle twitch only lasts a fraction of a second but involves the muscle both contracting and relaxing. A muscle will not always contract when stimulated by a motor neuron. The signal from the neuron must be strong enough to trigger a muscle impulse. Muscle contraction is considered an all or none response because as long as the signal from the neuron reaches a certain minimal level, the muscle fiber will always contract the same way with the same force, but if the signal is not strong enough, the muscle will remain relaxed.
Because the muscle twitch is such a short response, in order to contract an entire muscle the motor unit must be stimulated several times very quickly before it is able to relax completely. This can lead to tetanic contraction or continuous contraction of greater strength than a muscle twitch.
Muscle Physiology
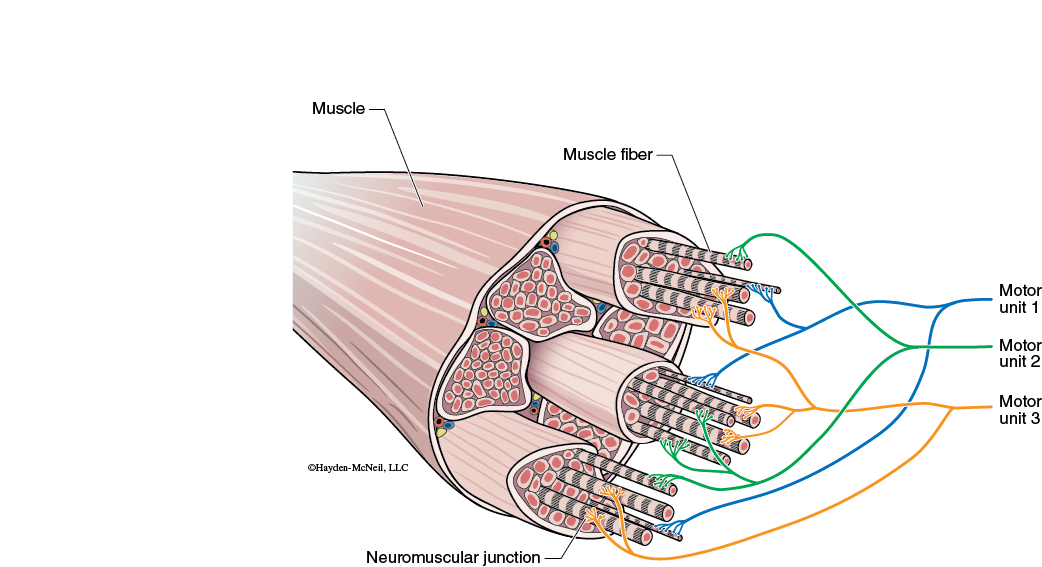
Contraction of skeletal muscle is controlled by impulses sent from motor neurons. Many muscle fibers within a muscle often contract at the same time because they are controlled by the same neuron, forming a motor unit. Motor units vary in size based on how many muscle fibers each neuron controls. Small motor units where one neuron controls few cells can be used for fine movements, whereas large motor units are found in large muscles used for less precise movements.
A neuromuscular junction refers to where the signal from a motor neuron is passed to the muscle fiber. The motor neuron releases the neurotransmitter acetylcholine, which excites the muscle fiber, creating a muscle impulse.
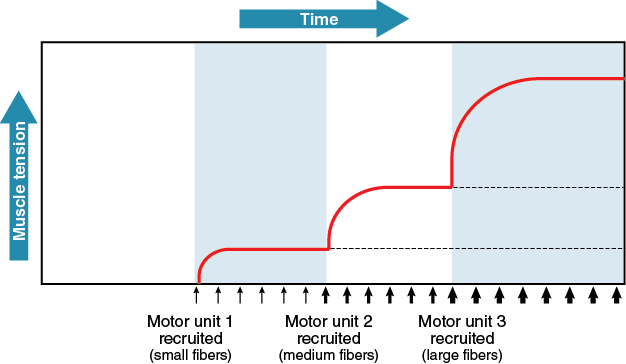
Any skeletal muscle shows a graded muscle response. This means that the strength of the contraction can vary from weak to very strong. This variation in contraction strength is caused by varying the number motor units used. Some motor units are continuously stimulated to maintain muscle tone. To increase contraction force, you need to have more muscle fibers contracting by using more motor units. Recruitment is the process of activating more motor units to create a stronger contraction.
Microscopic Structure of Skeletal Muscle
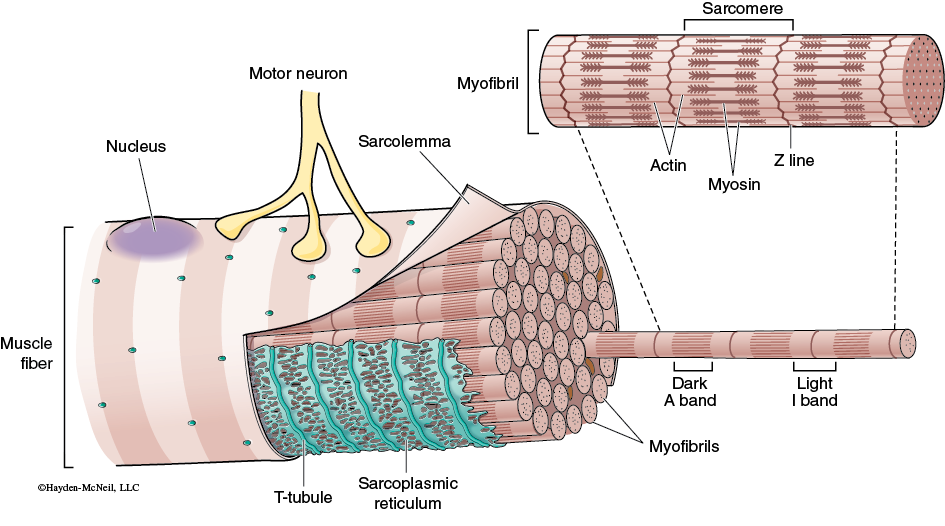
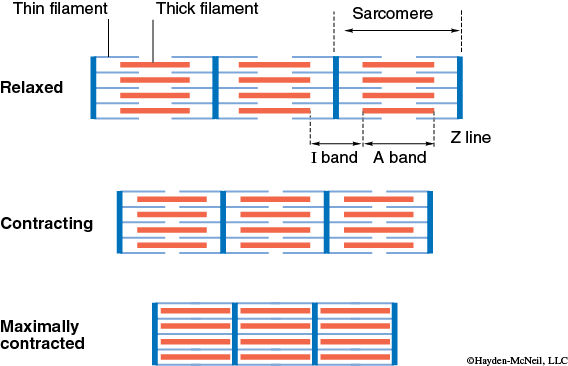
Each skeletal muscle fiber contains many myofibrils, surrounded by a plasma membrane called the sarcolemma. The myofibrils contain two different sized filaments. The thick filaments are formed of the molecule myosin, and thin filaments are formed of the molecule actin. The actin filaments are held in place by the z-line, which appears as a dark line that zigzags back and forth between actin filaments. Actin and myosin filaments alternate positions along the myofibrils to form light and dark banded regions known as striations. Dark bands appear where myosin is present, and light bands are located where we find actin and no myosin. A sarcomere is the smallest contracting unit of a muscle fiber, and extends from one z-line to the next z-line. As such, it is made of light regions at either end, with a dark region where myosin is present in the center.
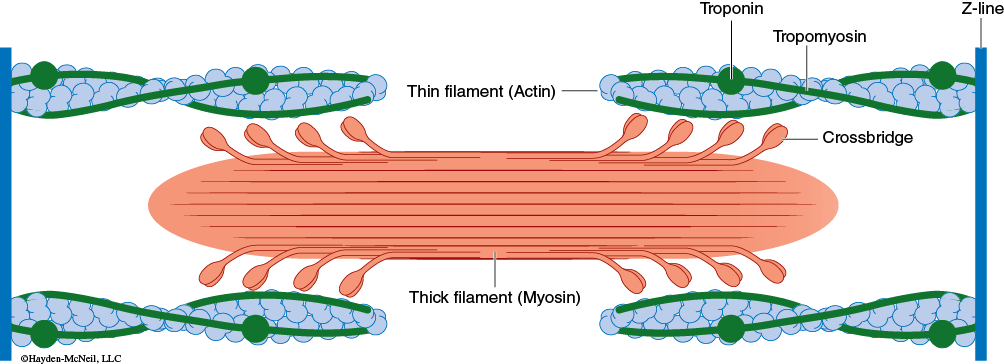
The myosin has paddle-like “heads” sticking out along its length. The heads are used to grab onto and pull the actin filaments forming cross bridges during muscle contraction. When myosin pulls on the actin, it moves the actin inwards along its length, shortening the sarcomere or distance between z-lines.
Two other proteins are associated with actin: troponin and tropomyosin. Together these proteins block the binding sites on the actin that the myosin heads grab on to. This keeps your muscles in a relaxed state unless they receive a signal from a motor neuron. When a motor neuron stimulates a muscle fiber, the impulse travels along the sarcolemma (outer plasma membrane of the muscle fiber), and along transverse tubules (t-tubules). The t-tubules extend inward from the sarcolemma, allowing the signal to travel inside the muscle fiber and around all of the myofibrils. Within the myofibril there is an extensive network of smooth endoplasmic reticulum called the sarcoplasmic reticulum. The sarcoplasmic reticulum surrounds each of the myofibrils and is in close contact with the t-tubules. The main function of the sarcoplasmic reticulum is to store calcium ions, and to release them in response to a muscle impulse.
Skeletal Muscle Contraction
Muscle contraction is stimulated by a motor neuron. The neuron releases acetylcholine at the neuromuscular junction. When acetylcholine binds to the muscle fiber, it triggers the generation of an electrical impulse along the muscle fiber known as a muscle impulse. The impulse travels along the sarcolemma and inward through the transverse tubules (t-tubules) to the entire muscle fiber. The muscle impulse on the t-tubules causes the sarcoplasmic reticulum to release calcium into the cytoplasm of the muscle fiber.
Once released, the calcium binds to the troponin which is attached to tropomyosin along the actin filaments. Binding of calcium to troponin, causes tropomyosin to move, exposing the myosin binding sites on the actin. Once the binding sites are exposed, myosin can grab onto the actin and muscle contraction can occur. Without calcium the places where myosin can attach and pull on actin remain covered, and no contraction can occur. There is a brief delay between the generation of a muscle impulse and muscle contraction known as the latent period. This is the time that it takes for calcium to be released from the sarcoplasmic reticulum and the binding sites on actin to be exposed.
When a muscle contracts the paddle-like heads of the myosin grab onto the binding sites of the actin, forming cross bridges. Myosin pulls the actin toward the center of the sarcomere. The myosin will pull once, let go, and then pull again. Myosin will continue to pull on actin as long as the muscle impulse is present and there is energy available. The sliding of actin towards the center of the sarcomere shortens the sarcomere. The muscle filaments remain the same length, but overlap more. The increased overlap is what causes the entire muscle to become shorter or contract. Once a muscle fiber is stimulated to contract, the force that it generates does depend on how stretched or contracted the muscle fiber already is. The closer the muscle fiber is to its resting length, the stronger the contraction. Contractions will be less strong if the filaments in the muscle fiber are already greatly overlapped, or barely overlapping.
Muscle Metabolism
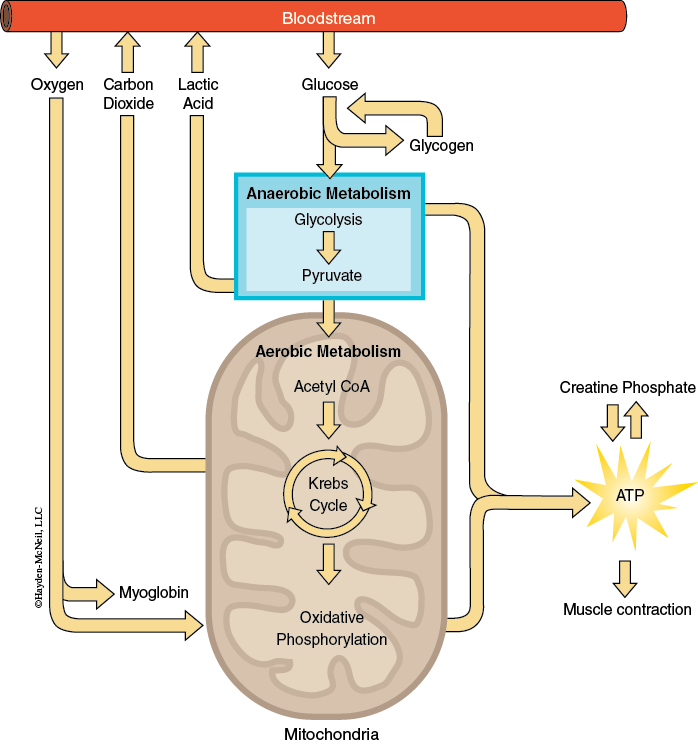
During muscle contraction, energy in the form of ATP is necessary to allow myosin to let go of the actin and be ready to pull again. A resting muscle only contains enough ATP for a few seconds of activity. After that, it must generate additional ATP from one of three sources. Creatine phosphate can be used to regenerate ATP. Resting muscles store more creatine phosphate than ATP, and it is often used to generate ATP during rapid, intense exercise. ATP and creatine phosphate stored within muscles do not provide enough energy for sustained exercise. For more sustained exercise, muscle cells will break down glucose to obtain ATP. Anaerobic metabolism involves breaking down glucose to generate ATP. However, this process can result in the accumulation of lactic acid in muscle tissue which causes muscle cramps. Aerobic metabolism is another way of producing ATP by breaking down glucose. The aerobic metabolism of glucose can produce a great deal of ATP over much longer periods of time, and will not accumulate lactic acid. However it requires an abundant oxygen supply.
The inability of a muscle to continue to contract after prolonged activity is known as muscle fatigue. Muscle fatigue can be caused by a lack of energy in the form of ATP, by a pH imbalance caused by the accumulation of lactic acid and other acids, by ion imbalances such as a lack of adequate calcium being released from the sarcoplasmic reticulum, or K+ depletion due to muscle impulses.
Muscle Fiber Type
Each muscle is made up of many individual muscle fibers. There are three types of muscle fibers, and each muscle contains various proportions of all three. Fast-twitch fibers contract rapidly and forcefully. However, they typically use anaerobic metabolism to generate energy and therefore are quick to fatigue. These fibers are good for quick, forceful movement such as lifting weights. Slow-twitch fibers use aerobic metabolism to generate energy, and contain myoglobin to store extra oxygen within the muscle fiber. These fibers are slower to contract but very resistant to fatigue. As a result they are best for the sustained contractions used in maintaining posture, or longer endurance activities such as running a marathon. Intermediate fibers also use aerobic metabolism to produce ATP, and contain myoglobin to store oxygen. They are faster to contract than the slow-twitch fibers but less resistant to fatigue. These fibers are best for activities like walking or sprinting.
Exercise
Aerobic training or endurance exercise involves activities where the body increases oxygen intake to meet the increased demand for oxygen by the muscles. It helps to build muscle endurance by increasing the number of blood capillaries surrounding the muscle fibers, and the ability of muscle fibers to store and use oxygen to generate ATP. Strength training or resistance exercise often involves using weights or other means of resistance to target and strengthen individual muscles or muscle groups. Resistance exercise can cause hypertrophy or enlargement of existing muscle fibers by enlarging existing myofibrils within muscle fibers and building new myofibrils. Hyperplasia is the growth of new cells by cell splitting. There is some evidence that suggests that human growth hormone can trigger hyperplasia in muscle tissue, increasing the number of muscle fibers. Muscle atrophy can be caused by a period of prolonged immobility as well as a variety of diseases, both of which result in a decrease in muscle mass and strength.