16.1 Introduction to Therapy and the Psychological Therapies
The long history of efforts to treat psychological disorders has included a bewildering mix of harsh and gentle methods. Well-

Treating Psychological Disorders
16-
Reformers Philippe Pinel (1745–
Modern Western therapies can be classified into two main categories:
- In psychotherapy, a trained therapist uses psychological techniques to assist someone seeking to overcome difficulties or achieve personal growth. The therapist may seek to uncover hidden meaning from a client’s early relationships, to encourage the client to adopt new ways of thinking, or to replace old behaviors with new ones.
- Biomedical therapy offers medications and other biological treatments. For example, a person with severe depression, as we will see, may receive antidepressants, electroconvulsive shock therapy (ECT), or deep-
brain stimulation.  The history of treatment Visitors to eighteenth-
The history of treatment Visitors to eighteenth-century mental hospitals paid to gawk at patients, as though they were viewing zoo animals. William Hogarth’s (1697– 1764) painting captured one of these visits to London’s St. Mary of Bethlehem hospital (commonly called Bedlam).
psychotherapy treatment involving psychological techniques; consists of interactions between a trained therapist and someone seeking to overcome psychological difficulties or achieve personal growth.
biomedical therapy prescribed medications or procedures that act directly on the person’s physiology.
Some psychologists consider psychotherapy to be a biological treatment, because changing the way we think and behave can prompt physical changes in the brain (Kandel, 2013). Effective psychotherapy is a brain-
eclectic approach an approach to psychotherapy that uses techniques from various forms of therapy.
The care provider’s training and expertise, as well as the disorder itself, influence the choice of treatment. Psychotherapy and medication are often combined. Kay Redfield Jamison received psychotherapy in her meetings with her psychiatrist, and she took medications to control her wild mood swings.
Let’s look first at the psychotherapy options for those treated with “talk therapies.” Each is built on one or more of psychology’s major theories: psychodynamic, humanistic, behavioral, and cognitive. Most of these techniques can be used one-
Psychoanalysis and Psychodynamic Therapies
psychoanalysis Sigmund Freud’s therapeutic technique. Freud believed the patient’s free associations, resistances, dreams, and transferences—and the therapist’s interpretations of them—released previously repressed feelings, allowing the patient to gain self-insight.
16-
The first major psychological therapy was Sigmund Freud’s psychoanalysis. Although few clinicians today practice therapy as Freud did, his work deserves discussion. It helped form the foundation for treating psychological disorders, partly by influencing modern therapists working from the psychodynamic perspective.
659
Goals
Freud believed that in therapy, people could achieve healthier, less anxious living by releasing the energy they had previously devoted to id-
Freud’s therapy aimed to bring patients’ repressed or disowned feelings into conscious awareness. By helping them reclaim their unconscious thoughts and feelings, and by giving them insight into the origins of their disorders, he aimed to help them reduce growth-
Techniques
Psychoanalysis is historical reconstruction. Psychoanalytic theory emphasizes the power of childhood experiences to mold the adult. Thus, it aims to unearth one’s past in the hope of unmasking the present. After discarding hypnosis as an unreliable excavator, Freud turned to free association.
resistance in psychoanalysis, the blocking from consciousness of anxiety-laden material.
Imagine yourself as a patient using free association. You begin by relaxing, perhaps by lying on a couch. As the psychoanalyst sits out of your line of vision, you say aloud whatever comes to mind. At one moment, you’re relating a childhood memory. At another, you’re describing a dream or recent experience. It sounds easy, but soon you notice how often you edit your thoughts as you speak. You pause for a second before uttering an embarrassing thought. You omit what seems trivial, irrelevant, or shameful. Sometimes your mind goes blank or you find yourself unable to remember important details. You may joke or change the subject to something less threatening.
interpretation in psychoanalysis, the analyst’s noting supposed dream meanings, resistances, and other significant behaviors and events in order to promote insight.
To the analyst, these mental blocks indicate resistance. They hint that anxiety lurks and you are defending against sensitive material. The analyst will note your resistances and then provide insight into their meaning. If offered at the right moment, this interpretation—of, say, your not wanting to talk about your mother—
transference in psychoanalysis, the patient’s transfer to the analyst of emotions linked with other relationships (such as love or hatred for a parent).
Over many such sessions, your relationship patterns surface in your interaction with your therapist. You may find yourself experiencing strong positive or negative feelings for your analyst. The analyst may suggest you are transferring feelings, such as feelings of dependency or mingled love and anger, that you experienced in earlier relationships with family members or other important people. By exposing such feelings, you may gain insight into your current relationships.
Relatively few North American therapists now offer traditional psychoanalysis. Much of its underlying theory is not supported by scientific research (Chapter 14). Analysts’ interpretations cannot be proven or disproven. And psychoanalysis takes considerable time and money, often years of several sessions per week. Some of these problems have been addressed in the modern psychodynamic perspective that has evolved from psychoanalysis.
“I haven’t seen my analyst in 200 years. He was a strict Freudian. If I’d been going all this time, I’d probably almost be cured by now.”
Woody Allen, after awakening from suspended animation in the movie Sleeper
RETRIEVAL PRACTICE
- In psychoanalysis, when patients experience strong feelings for their therapist, this is called ______________. Patients are said to demonstrate anxiety when they put up mental blocks around sensitive memories, indicating ______________. The therapist will attempt to provide insight into the underlying anxiety by offering a(n) ______________ of the mental blocks.
transference; resistance; interpretation
660
psychodynamic therapy therapy deriving from the psychoanalytic tradition; views individuals as responding to unconscious forces and childhood experiences, and seeks to enhance self-insight.
Psychodynamic Therapy
Although influenced by Freud’s ideas, psychodynamic therapists don’t talk much about id, ego, and superego. Instead they try to help people understand their current symptoms. They focus on themes across important relationships, including childhood experiences and the therapist relationship. Rather than lying on a couch, out of the therapist’s line of vision, patients meet with their therapist face-
In these sessions, patients gain perspective by exploring defended-
| Therapist: | Do you mean, then, that if you could, you would like to? |
| Patient: | Well, I don’t know. … Maybe I can’t say it because I’m not sure it’s true. Maybe I don’t love her. |
Further interactions reveal that he can’t express real love because it would feel “mushy” and “soft” and therefore unmanly. He is “in conflict with himself, and he is cut off from the nature of that conflict.” Shapiro noted that with such patients, who are estranged from themselves, therapists using psychodynamic techniques “are in a position to introduce them to themselves. We can restore their awareness of their own wishes and feelings, and their awareness, as well, of their reactions against those wishes and feelings.”
Psychodynamic therapists may also help reveal past relationship troubles as the origin of current difficulties. Jonathan Shedler (2010a) recalls his patient Jeffrey’s complaints of difficulty getting along with his colleagues and wife, who saw him as hypercritical. Jeffrey then “began responding to me as if I were an unpredictable, angry adversary.” Shedler seized this opportunity to help Jeffrey recognize the relationship pattern, and its roots in the attacks and humiliation he experienced from his alcohol-

Interpersonal psychotherapy, a brief (12-
The case of Anna, a 34-
661
Humanistic Therapies
16-
The humanistic perspective (Chapter 14) emphasizes people’s inherent potential for self-
- Humanistic therapists aim to boost people’s self-fulfillment by helping them grow in self-awareness and self-acceptance.
- Promoting this growth, not curing illness, is the therapy focus. Thus, those in therapy became “clients” or just “persons” rather than “patients” (a change many other therapists have adopted).
- The path to growth is taking immediate responsibility for one’s feelings and actions, rather than uncovering hidden determinants.
- Conscious thoughts are more important than the unconscious.
- The present and future are more important than the past. The goal is to explore feelings as they occur, rather than achieve insights into the childhood origins of the feelings.
insight therapies a variety of therapies that aim to improve psychological functioning by increasing a person’s awareness of underlying motives and defenses.
client-centered therapy a humanistic therapy, developed by Carl Rogers, in which the therapist uses techniques such as active listening within a genuine, accepting, empathic environment to facilitate clients’ growth. (Also called person-centered therapy.)
Carl Rogers (1902–
Believing that most people possess the resources for growth, Rogers (1961, 1980) encouraged therapists to exhibit genuineness, acceptance, and empathy. When therapists drop their facades and genuinely express their true feelings, when they enable their clients to feel unconditionally accepted, and when they empathically sense and reflect their clients’ feelings, the clients may deepen their self-
Hearing has consequences. When I truly hear a person and the meanings that are important to him at that moment, hearing not simply his words, but him, and when I let him know that I have heard his own private personal meanings, many things happen. There is first of all a grateful look. He feels released. He wants to tell me more about his world. He surges forth in a new sense of freedom. He becomes more open to the process of change.
active listening empathic listening in which the listener echoes, restates, and clarifies. A feature of Rogers’ client-centered therapy.
I have often noticed that the more deeply I hear the meanings of the person, the more there is that happens. Almost always, when a person realizes he has been deeply heard, his eyes moisten. I think in some real sense he is weeping for joy. It is as though he were saying, “Thank God, somebody heard me. Someone knows what it’s like to be me.”
“Hearing” refers to Rogers’ technique of active listening—echoing, restating, and seeking clarification of what the person expresses (verbally or nonverbally) and acknowledging the expressed feelings. Active listening is now an accepted part of therapeutic counseling practices in many schools, colleges, and clinics. The counselor listens attentively and interrupts only to restate and confirm feelings, to accept what is being expressed, or to seek clarification. The following brief excerpt between Rogers and a male client illustrates how he sought to provide a psychological mirror that would help clients see themselves more clearly.
“We have two ears and one mouth that we may listen the more and talk the less.”
Zeno, 335–263 b.c.e., Diogenes Laertius
662
| Rogers: | Feeling that now, hm? That you’re just no good to yourself, no good to anybody. Never will be any good to anybody. Just that you’re completely worthless, huh?—Those really are lousy feelings. Just feel that you’re no good at all, hm? |
| Client: | Yeah. (Muttering in low, discouraged voice) That’s what this guy I went to town with just the other day told me. |
| Rogers: | This guy that you went to town with really told you that you were no good? Is that what you’re saying? Did I get that right? |
| Client: |
M- |
| Rogers: | I guess the meaning of that if I get it right is that here’s somebody that— |
| Client: | (Rather defiantly) I don’t care though. |
| Rogers: | You tell yourself you don’t care at all, but somehow I guess some part of you cares because some part of you weeps over it. |
|
(Meador & Rogers, 1984, p. 167) |
unconditional positive regard a caring, accepting, nonjudgmental attitude, which Carl Rogers believed would help clients develop self-awareness and self-acceptance.
Can a therapist be a perfect mirror, without selecting and interpreting what is reflected? Rogers conceded that one cannot be totally nondirective. Nevertheless, he believed that the therapist’s most important contribution is to accept and understand the client. Given a nonjudgmental, grace-
If you want to listen more actively in your own relationships, three Rogers-
- Paraphrase. Rather than saying “I know how you feel,” check your understandings by summarizing the person’s words in your own words.
- Invite clarification. “What might be an example of that?” may encourage the person to say more.
- Reflect feelings.“It sounds frustrating” might mirror what you’re sensing from the person’s body language and intensity.
Behavior Therapies
behavior therapy therapy that applies learning principles to the elimination of unwanted behaviors.
16-
The insight therapies assume that many psychological problems diminish as self-
663
Classical Conditioning Techniques
counterconditioning behavior therapy procedures that use classical conditioning to evoke new responses to stimuli that are triggering unwanted behaviors; include exposure therapies and aversive conditioning.
One cluster of behavior therapies derives from principles developed in Ivan Pavlov’s early twentieth-
Another example: If a claustrophobic fear of elevators is a learned aversion to being in a confined space, then might one unlearn that association by reconditioning to replace the fear response? Counterconditioning pairs the trigger stimulus (in this case, the enclosed space of the elevator) with a new response (relaxation) that is incompatible with fear. Two specific counterconditioning techniques—
RETRIEVAL PRACTICE
- What might a psychodynamic therapist say about Mowrer’s therapy for bed-wetting? How might a behavior therapist reply?
A psychodynamic therapist might be more interested in helping the child develop insight about the underlying problems that have caused the bed-
Exposure Therapies Picture this scene reported in 1924 by behaviorist psychologist Mary Cover Jones: Three-
As Peter begins his midafternoon snack, Jones introduces a caged rabbit on the other side of the huge room. Peter, eagerly munching away on his crackers and drinking his milk, hardly notices. On succeeding days, she gradually moves the rabbit closer and closer. Within two months, Peter is tolerating the rabbit in his lap, even stroking it while he eats. Moreover, his fear of other furry objects subsides as well, having been countered, or replaced, by a relaxed state that cannot coexist with fear (Fisher, 1984; Jones, 1924).

exposure therapies behavioral techniques, such as systematic desensitization and virtual reality exposure therapy, that treat anxieties by exposing people (in imagination or actual situations) to the things they fear and avoid.
Unfortunately for those who might have been helped by her counterconditioning procedures, Jones’ story of Peter and the rabbit did not immediately become part of psychology’s lore. It was more than 30 years later that psychiatrist Joseph Wolpe (1958; Wolpe & Plaud, 1997) refined Jones’ technique into what are now the most widely used types of behavior therapies: exposure therapies, which expose people to what they normally avoid or escape (behaviors that get reinforced by reduced anxiety). Exposure therapies have them face their fear, and thus overcome their fear of the fear response itself. As people can habituate to the sound of a train passing their new apartment, so, with repeated exposure, can they become less anxiously responsive to things that once petrified them (Barrera et al., 2013; Foa et al., 2013).
systematic desensitization a type of exposure therapy that associates a pleasant relaxed state with gradually increasing anxiety-triggering stimuli. Commonly used to treat phobias.
664
One widely used exposure therapy is systematic desensitization. Wolpe assumed, as did Jones, that you cannot be simultaneously anxious and relaxed. Therefore, if you can repeatedly relax when facing anxiety-
Next, using progressive relaxation, the therapist would train you to relax one muscle group after another, until you achieve a blissful state of complete relaxation and comfort. Then the therapist would ask you to imagine, with your eyes closed, a mildly anxiety-
The therapist would progress up the constructed anxiety hierarchy, using the relaxed state to desensitize you to each imagined situation. After several sessions, you move to actual situations and practice what you had only imagined before, beginning with relatively easy tasks and gradually moving to more anxiety-
“The only thing we have to fear is fear itself.”
U.S. President Franklin D. Roosevelt First Inaugural Address, 1933
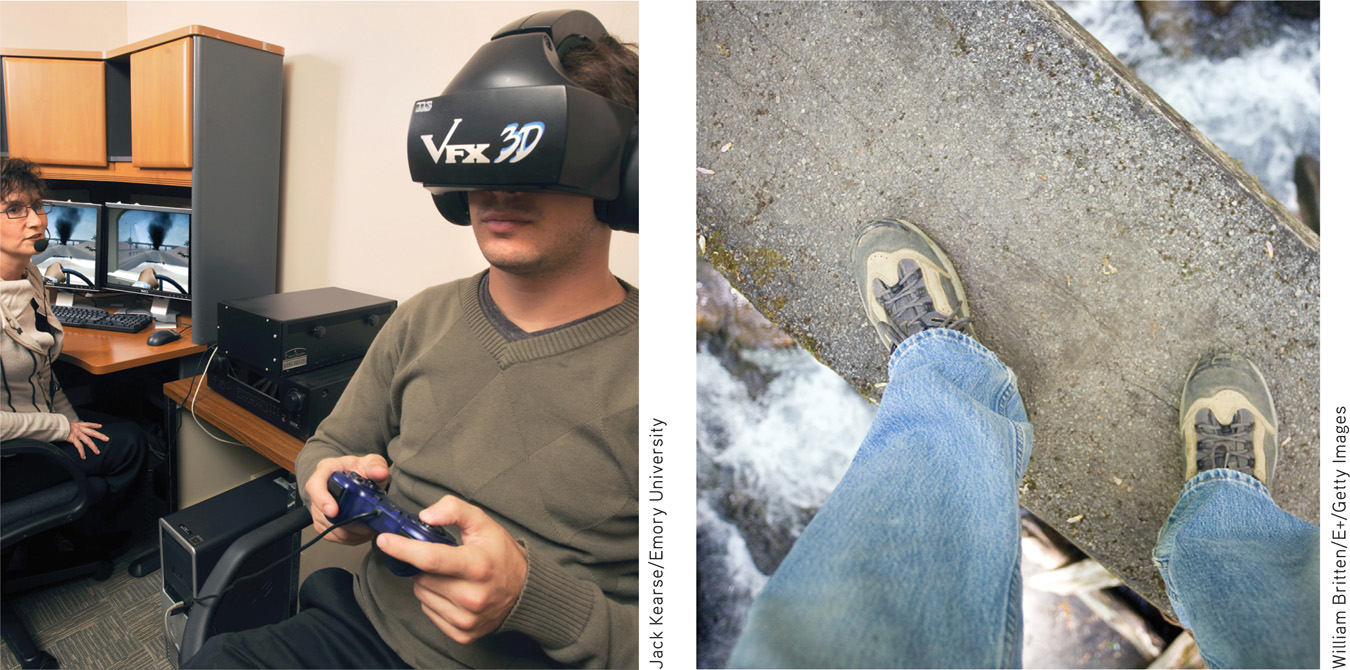
virtual reality exposure therapy an anxiety treatment that progressively exposes people to electronic simulations of their greatest fears, such as airplane flying, spiders, or public speaking.
When an anxiety-
aversive conditioning a type of counterconditioning that associates an unpleasant state (such as nausea) with an unwanted behavior (such as drinking alcohol).
665
Aversive Conditioning In systematic desensitization, the goal is substituting a positive (relaxed) response for a negative (fearful) response to a harmless stimulus. In aversive conditioning, the goal is substituting a negative (aversive) response for a positive response to a harmful stimulus (such as alcohol). Thus, aversive conditioning is the reverse of systematic desensitization—
The procedure is simple: It associates the unwanted behavior with unpleasant feelings. To treat nail biting, one can paint the fingernails with a nasty-
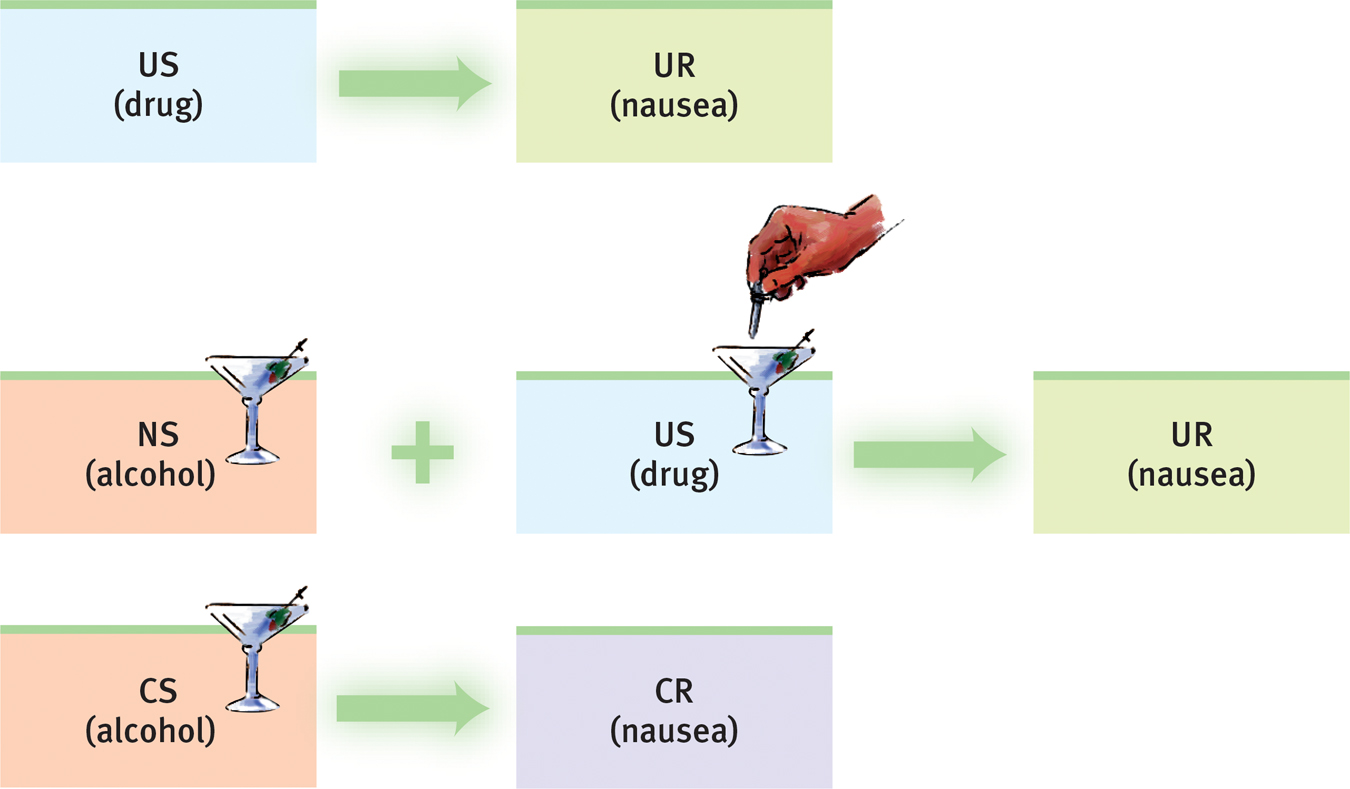
Aversion therapy for alcohol use disorder After repeatedly imbibing an alcoholic drink mixed with a drug that produces severe nausea, some people with a history of alcohol use disorder develop at least a temporary conditioned aversion to alcohol. (Remember: US is unconditioned stimulus, UR is unconditioned response, NS is neutral stimulus, CS is conditioned stimulus, and CR is conditioned response.)
Does aversive conditioning work? In the short run it may. Arthur Wiens and Carol Menustik (1983) studied 685 hospital patients with alcohol use disorder who completed an aversion therapy program. One year later, after returning for several booster treatments of alcohol-
The problem is that in therapy (as in research), cognition influences conditioning. People know that outside the therapist’s office they can drink without fear of nausea. Their ability to discriminate between the aversive conditioning situation and all other situations can limit the treatment’s effectiveness. Thus, therapists often use aversive conditioning in combination with other treatments.
Operant Conditioning
16-
The work of B. F. Skinner and others teaches us a basic principle of operant conditioning: Voluntary behaviors are strongly influenced by their consequences. Knowing this, some behavior therapists practice behavior modification. They reinforce desired behaviors, and they withhold reinforcement for undesired behaviors. Using operant conditioning to solve specific behavior problems has raised hopes for some otherwise hopeless cases. Children with intellectual disabilities have been taught to care for themselves. Socially withdrawn children with autism spectrum disorder (ASD) have learned to interact. People with schizophrenia have been helped to behave more rationally in their hospital ward. In such cases, therapists use positive reinforcers to shape behavior in a step-
In extreme cases, treatment must be intensive. One study worked with 19 withdrawn, uncommunicative 3-
token economy an operant conditioning procedure in which people earn a token of some sort for exhibiting a desired behavior and can later exchange their tokens for various privileges or treats.
666
Rewards used to modify behavior vary. For some people, the reinforcing power of attention or praise is sufficient. Others require concrete rewards, such as food. In institutional settings, therapists may create a token economy. When people display appropriate behavior, such as getting out of bed, washing, dressing, eating, talking coherently, cleaning up their rooms, or playing cooperatively, they receive a token or plastic coin as a positive reinforcer. Later, they can exchange their accumulated tokens for various rewards, such as candy, TV time, trips to town, or better living quarters. Token economies have been successfully applied in various settings (homes, classrooms, hospitals, institutions for juvenile offenders) and among members of various populations (including disturbed children and people with schizophrenia and other mental disabilities).
Critics of behavior modification express two concerns. The first is practical: How durable are the behaviors? Will people become so dependent on extrinsic rewards that the appropriate behaviors will stop when the reinforcers stop? Proponents of behavior modification believe the behaviors will endure if therapists wean patients from the tokens by shifting them toward other, real-
The second concern is ethical: Is it right for one human to control another’s behavior? Those who set up token economies deprive people of something they desire and decide which behaviors to reinforce. To critics, this whole process has an authoritarian taint. Advocates reply that some patients request the therapy. Moreover, control already exists; rewards and punishers are already maintaining destructive behavior patterns. So why not reinforce adaptive behavior instead? Treatment with positive rewards is more humane than being institutionalized or punished, advocates argue, and the right to effective treatment and an improved life justifies temporary deprivation.
RETRIEVAL PRACTICE
- What are the insight therapies, and how do they differ from behavior therapies?
The insight therapies—psychodynamic and humanistic therapies—
- Some maladaptive behaviors are learned. What hope does this fact provide?
If a behavior can be learned, it can be unlearned, and replaced by other more adaptive responses.
- Exposure therapies and aversive conditioning are applications of ______________ conditioning. Token economies are an application of ______________ conditioning.
classical; operant
Cognitive Therapies
16-
We have seen how behavior therapists treat specific fears and problem behaviors. But how do they deal with depressive disorders? Or with generalized anxiety, in which anxiety has no focus? Behavior therapists treating these less clearly defined psychological problems have had help from the same cognitive revolution that has profoundly changed other areas of psychology during the last half-
667
cognitive therapy therapy that teaches people new, more adaptive ways of thinking; based on the assumption that thoughts intervene between events and our emotional reactions.
The cognitive therapies assume that our thinking colors our feelings (FIGURE 16.2). Between an event and our response lies the mind. Self-
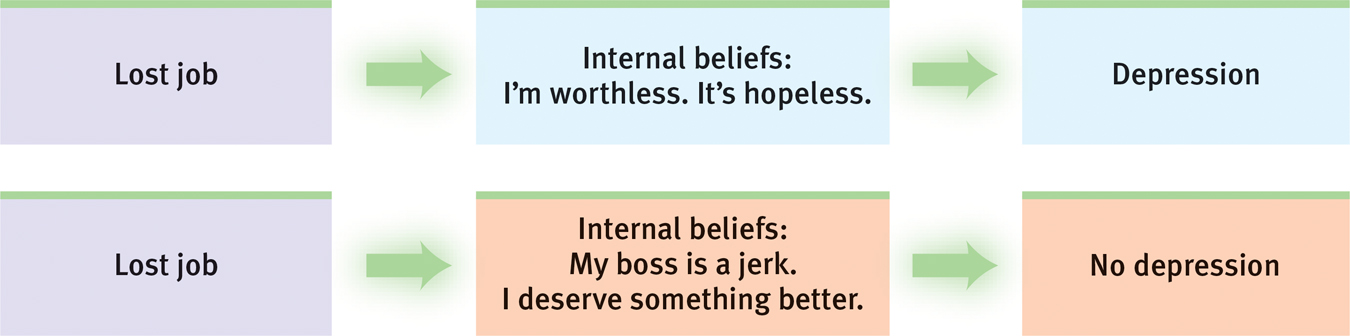
A cognitive perspective on psychological disorders The person’s emotional reactions are produced not directly by the event but by the person’s thoughts in response to the event.
“Life does not consist mainly, or even largely, of facts and happenings. It consists mainly of the storm of thoughts that are forever blowing through one’s mind.”
Mark Twain, 1835–1910
Aaron Beck’s Therapy for Depression
Cognitive therapist Aaron Beck believes that changing people’s thinking can change their functioning. When Beck analyzed depressed people’s dreams, he found recurring negative themes of loss, rejection, and abandonment that extended into their waking thoughts. Such negativity even extends into therapy, as clients recall and rehearse their failings and worst impulses (Kelly, 2000). With cognitive therapy, Beck and his colleagues (1979) sought to reverse clients’ catastrophizing beliefs about themselves, their situations, and their futures. Gentle questioning seeks to reveal irrational thinking, and then to persuade people to remove the dark glasses through which they view life (Beck et al., 1979, pp. 145–
| Client: | I agree with the descriptions of me but I guess I don’t agree that the way I think makes me depressed. |
| Beck: | How do you understand it? |
| Client: | I get depressed when things go wrong. Like when I fail a test. |
| Beck: | How can failing a test make you depressed? |
| Client: | Well, if I fail I’ll never get into law school. |
| Beck: | So failing the test means a lot to you. But if failing a test could drive people into clinical depression, wouldn’t you expect everyone who failed the test to have a depression? … Did everyone who failed get depressed enough to require treatment? |
| Client: | No, but it depends on how important the test was to the person. |
| Beck: | Right, and who decides the importance? |
| Client: | I do. |
| Beck: | And so, what we have to examine is your way of viewing the test (or the way that you think about the test) and how it affects your chances of getting into law school. Do you agree? |
| Client: | Right. |
| Beck: | Do you agree that the way you interpret the results of the test will affect you? You might feel depressed, you might have trouble sleeping, not feel like eating, and you might even wonder if you should drop out of the course. |
| Client: | I have been thinking that I wasn’t going to make it. Yes, I agree. |
| Beck: | Now what did failing mean? |
| Client: | (tearful) That I couldn’t get into law school. |
| Beck: | And what does that mean to you? |
| Client: | That I’m just not smart enough. |
| Beck: | Anything else? |
| Client: | That I can never be happy. |
| Beck: | And how do these thoughts make you feel? |
| Client: | Very unhappy. |
| Beck: | So it is the meaning of failing a test that makes you very unhappy. In fact, believing that you can never be happy is a powerful factor in producing unhappiness. So, you get yourself into a trap— |
We often think in words. Therefore, getting people to change what they say to themselves is an effective way to change their thinking. Perhaps you can identify with the anxious students who, before an exam, make matters worse with self-
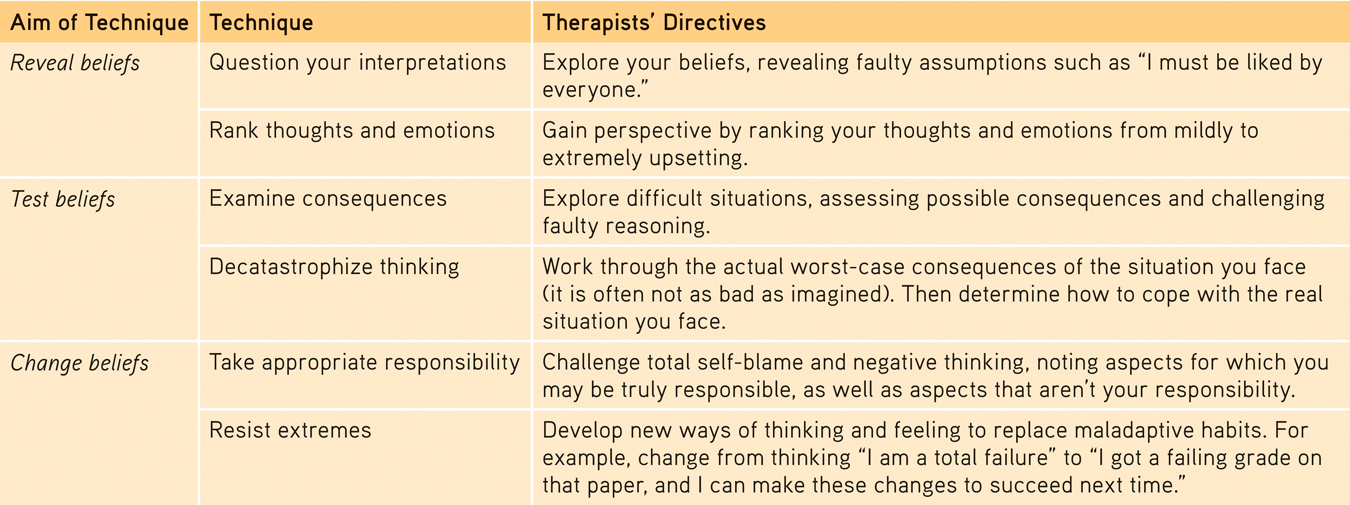
Selected Cognitive Therapy Techniques
669
It’s not just depressed people who can benefit from positive self-
cognitive-behavioral therapy (CBT) a popular integrative therapy that combines cognitive therapy (changing self-defeating thinking) with behavior therapy (changing behavior).
Cognitive-
Cognitive-behavioral therapy (CBT) today’s most widely practiced psychotherapy, aims not only to alter the way people think (cognitive therapy), but also to alter the way they act (behavior therapy). It seeks to make people aware of their irrational negative thinking, to replace it with new ways of thinking, and to practice the more positive approach in everyday settings. Behavioral change is typically addressed first, followed by sessions on cognitive change; the therapy concludes with a focus on maintaining both and preventing relapses.
“The trouble with most therapy is that it helps you to feel better. But you don’t get better. You have to back it up with action, action, action.”
Therapist Albert Ellis (1913–2007)
Anxiety, depressive disorders, and bipolar disorder share a common problem: emotion regulation (Aldao & Nolen-
CBT may also be useful with obsessive-
670
Studies have also found that cognitive-
RETRIEVAL PRACTICE
- How do the humanistic and cognitive therapies differ?
By reflecting clients’ feelings in a nondirective setting, the humanistic therapies attempt to foster personal growth by helping clients become more self-
- An influential cognitive therapy for depression was developed by ______________ ______________.
Aaron Beck
- What is cognitive-behavioral therapy, and what sorts of problems does this therapy best address?
This integrative therapy helps people change self-
Group and Family Therapies
16-
Group Therapy
Except for traditional psychoanalysis, most therapies may also occur in small groups. Group therapy does not provide the same degree of therapist involvement with each client. However, it offers many benefits:
- It saves therapists’ time and clients’ money, often with no less effectiveness than individual therapy (Fuhriman & Burlingame, 1994).
- It offers a social laboratory for exploring social behaviors and developing social skills. Therapists frequently suggest group therapy for people experiencing frequent conflicts or whose behavior distresses others. For up to 90 minutes weekly, the therapist guides people’s interactions as they discuss issues and try out new behaviors.
- It enables people to see that others share their problems. It can be a relief to discover that you are not alone—to learn that others, despite their composure, experience some of the same troublesome feelings and behaviors.
- It provides feedback as clients try out new ways of behaving. Hearing that you look poised, even though you feel anxious and self-conscious, can be very reassuring.
group therapy therapy conducted with groups rather than individuals, permitting therapeutic benefits from group interaction.
family therapy therapy that treats the family as a system. Views an individual’s unwanted behaviors as influenced by, or directed at, other family members.
Family Therapy
One special type of group interaction, family therapy, assumes that no person is an island: We live and grow in relation to others, especially our families. We struggle to differentiate ourselves from our families, but we also need to connect with them emotionally. Some of our problem behaviors arise from the tension between these two tendencies, which can create family stress.
671
Unlike most psychotherapy, which focuses on what happens inside the person’s own skin, family therapists work with multiple family members to heal relationships and to mobilize family resources. They tend to view the family as a system in which each person’s actions trigger reactions from others, and they help family members discover their role within their family’s social system. A child’s rebellion, for example, affects and is affected by other family tensions. Therapists also attempt—

Self-
Many people also participate in self-
The grandparent of support groups, Alcoholics Anonymous (AA), reports having 2.1 million members in 115,000 groups worldwide. Its famous 12-
With more than 2 million members worldwide, AA is said to be “the largest organization on Earth that nobody wanted to join” (Finlay, 2000).
In an individualistic age, with more and more people living alone or feeling isolated, the popularity of support groups—
***
For a synopsis of the modern forms of psychotherapy we’ve been discussing, see TABLE 16.2 below.
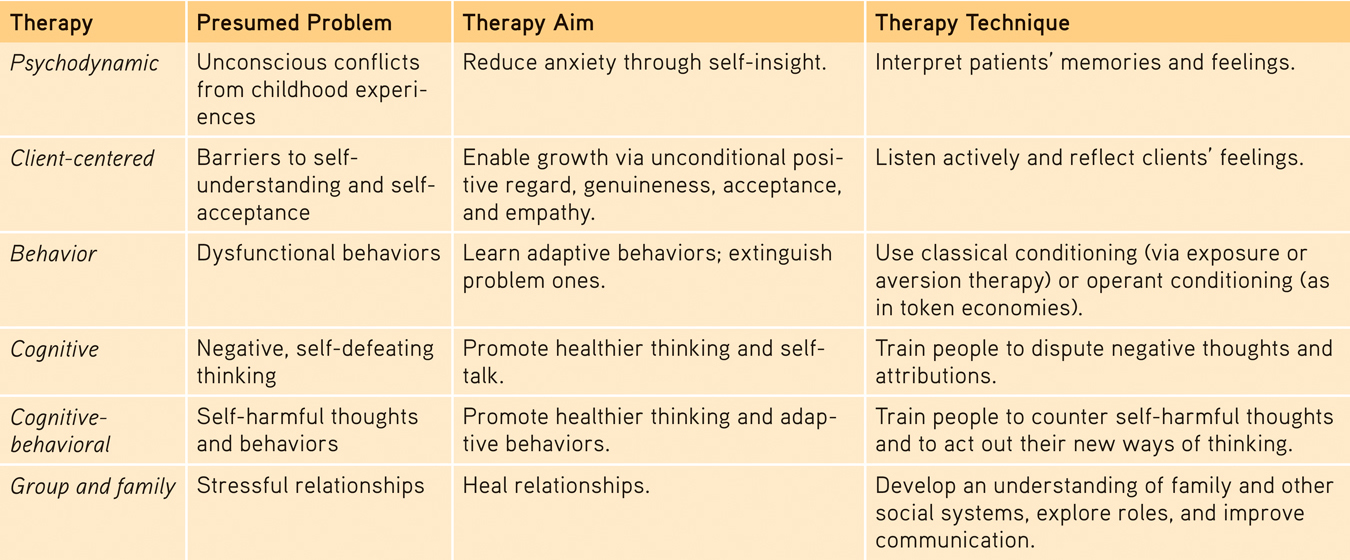
Comparing Modern Psychotherapies
672
 To review the aims and techniques of different psychotherapies, and assess your ability to recognize excerpts from each, visit LaunchPad’s PsychSim 6: Mystery Therapist.
To review the aims and techniques of different psychotherapies, and assess your ability to recognize excerpts from each, visit LaunchPad’s PsychSim 6: Mystery Therapist.
REVIEW: Introduction to Therapy and the Psychological Therapies

|
REVIEW | Introduction to Therapy and the Psychological Therapies |
LEARNING OBJECTIVES
RETRIEVAL PRACTICE Take a moment to answer each of these Learning Objective Questions (repeated here from within this section). Then click the 'show answer' button to check your answers. Research suggests that trying to answer these questions on your own will improve your long-term retention (McDaniel et al., 2009).
16-
Psychotherapy is treatment involving psychological techniques; it consists of interactions between a trained therapist and someone seeking to overcome psychological difficulties or achieve personal growth. The major psychotherapies derive from psychology’s psychodynamic, humanistic, behavioral, and cognitive perspectives. Biomedical therapy treats psychological disorders with medications or procedures that act directly on a patient’s physiology. An eclectic approach combines techniques from various forms of therapy.
16-
Through psychoanalysis, Sigmund Freud tried to give people self-insight and relief from their disorders by bringing anxiety-laden feelings and thoughts into conscious awareness. Psychoanalytic techniques included using free association and interpretation of instances of resistance and transference. Psychodynamic therapy has been influenced by traditional psychoanalysis but differs from it in many ways, including the lack of belief in id, ego, and superego. This contemporary therapy is briefer, less expensive, and more focused on helping the client find relief from current symptoms. Psychodynamic therapists help clients understand how past relationships create themes that may be acted out in present relationships. Interpersonal therapy is a brief 12- to 16-session form of psychodynamic therapy that has been effective in treating depression.
16-
Both psychoanalytic and humanistic therapists are insight therapies—they attempt to improve functioning by increasing clients’ awareness of motives and defenses. Humanistic therapy’s goals have included helping clients grow in self-awareness and self-acceptance; promoting personal growth rather than curing illness; helping clients take responsibility for their own growth; focusing on conscious thoughts rather than unconscious motivations; and seeing the present and future as more important than the past.
Carl Rogers’ client-centered therapy proposed that therapists’ most important contributions are to function as a psychological mirror through active listening and to provide a growth-fostering environment of unconditional positive regard, characterized by genuineness, acceptance, and empathy.
16-
Behavior therapies are not insight therapies. Their goal is to apply learning principles to modify problem behaviors.
Classical conditioning techniques, including exposure therapies (such as systematic desensitization or virtual reality exposure therapy) and aversive conditioning, attempt to change behaviors through counterconditioning—evoking new responses to old stimuli that trigger unwanted behaviors.
16-
Operant conditioning operates under the premise that voluntary behaviors are strongly influenced by their consequences. Therapy based on operant conditioning principles uses behavior modification techniques to change unwanted behaviors through positively reinforcing desired behaviors and ignoring or punishing undesirable behaviors.
Critics maintain that (1) techniques such as those used in token economies may produce behavior changes that disappear when rewards end, and (2) deciding which behaviors should change is authoritarian and unethical. Proponents argue that treatment with positive rewards is more humane than punishing people or institutionalizing them for undesired behaviors.
16-
The cognitive therapies, such as Aaron Beck’s cognitive therapy for depression, assume that our thinking influences our feelings, and that the therapist’s role is to change clients’ self-defeating thinking by training them to view themselves in more positive ways. The widely researched and practiced cognitive-behavioral therapy (CBT) combines cognitive therapy and behavior therapy by helping clients regularly act out their new ways of thinking and talking in their everyday life.
16-
Group therapy sessions can help more people and costs less per person than individual therapy would. Clients may benefit from exploring feelings and developing social skills in a group situation, from learning that others have similar problems, and from getting feedback on new ways of behaving. Family therapy views a family as an interactive system and attempts to help members discover the roles they play and to learn to communicate more openly and directly.
TERMS AND CONCEPTS TO REMEMBER
RETRIEVAL PRACTICE Match each of the terms on the left with its definition on the right. Click on the term first and then click on the matching definition. As you match them correctly they will move to the bottom of the activity.
Question
psychotherapy biomedical therapy eclectic approach psychoanalysis resistance interpretation transference psychodynamic therapy insight therapies client-centered therapy active listening unconditional positive regard behavior therapy counterconditioning exposure therapies systematic desensitization virtual reality exposure therapy aversive conditioning token economy cognitive therapy cognitive-behavioral therapy (CBT) group therapy family therapy | therapy deriving from the psychoanalytic tradition; views individuals as responding to unconscious forces and childhood experiences, and seeks to enhance self-insight. behavior therapy procedures that use classical conditioning to evoke new responses to stimuli that are triggering unwanted behaviors; include exposure therapies and aversive conditioning. a humanistic therapy, developed by Carl Rogers, in which the therapist uses techniques such as active listening within a genuine, accepting, empathic environment to facilitate clients’ growth. (Also called person-centered therapy.) a type of exposure therapy that associates a pleasant relaxed state with gradually increasing anxiety-triggering stimuli. Commonly used to treat phobias. an operant conditioning procedure in which people earn a token of some sort for exhibiting a desired behavior and can later exchange their tokens for various privileges or treats. behavioral techniques, such as systematic desensitization and virtual reality exposure therapy, that treat anxieties by exposing people (in imagination or actual situations) to the things they fear and avoid. therapy conducted with groups rather than individuals, permitting therapeutic benefits from group interaction. a type of counterconditioning that associates an unpleasant state (such as nausea) with an unwanted behavior (such as drinking alcohol). in psychoanalysis, the blocking from consciousness of anxiety-laden material. an approach to psychotherapy that uses techniques from various forms of therapy. a variety of therapies that aim to improve psychological functioning by increasing a person’s awareness of underlying motives and defenses. in psychoanalysis, the patient’s transfer to the analyst of emotions linked with other relationships (such as love or hatred for a parent). in psychoanalysis, the analyst’s noting supposed dream meanings, resistances, and other significant behaviors and events in order to promote insight. therapy that teaches people new, more adaptive ways of thinking; based on the assumption that thoughts intervene between events and our emotional reactions. an anxiety treatment that progressively exposes people to electronic simulations of their greatest fears, such as airplane flying, spiders, or public speaking. prescribed medications or procedures that act directly on the person’s physiology. a popular integrative therapy that combines cognitive therapy (changing self-defeating thinking) with behavior therapy (changing behavior). empathic listening in which the listener echoes, restates, and clarifies. A feature of Rogers’ client-centered therapy. therapy that applies learning principles to the elimination of unwanted behaviors. a caring, accepting, nonjudgmental attitude, which Carl Rogers believed would help clients develop self-awareness and self-acceptance. Sigmund Freud’s therapeutic technique. Freud believed the patient’s free associations, resistances, dreams, and transferences—and the therapist’s interpretations of them—released previously repressed feelings, allowing the patient to gain self-insight. therapy that treats the family as a system. Views an individual’s unwanted behaviors as influenced by, or directed at, other family members. treatment involving psychological techniques; consists of interactions between a trained therapist and someone seeking to overcome psychological difficulties or achieve personal growth. |
Use  to create your personalized study plan, which will direct you to the resources that will help you most in
.
to create your personalized study plan, which will direct you to the resources that will help you most in
.
673