3.3 Drugs and Consciousness
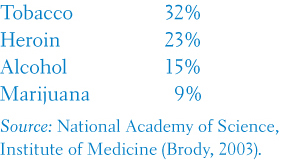
The odds of getting hooked after using various drugs:
Let’s imagine a day in the life of a legal drug user. It begins with a wake-
Tolerance and Addiction
3-
substance use disorder continued substance craving and use despite significant life disruption and/or physical risk.
Most of us manage to use some nonprescription drugs in moderation and without disrupting our lives. But some of us develop a self-
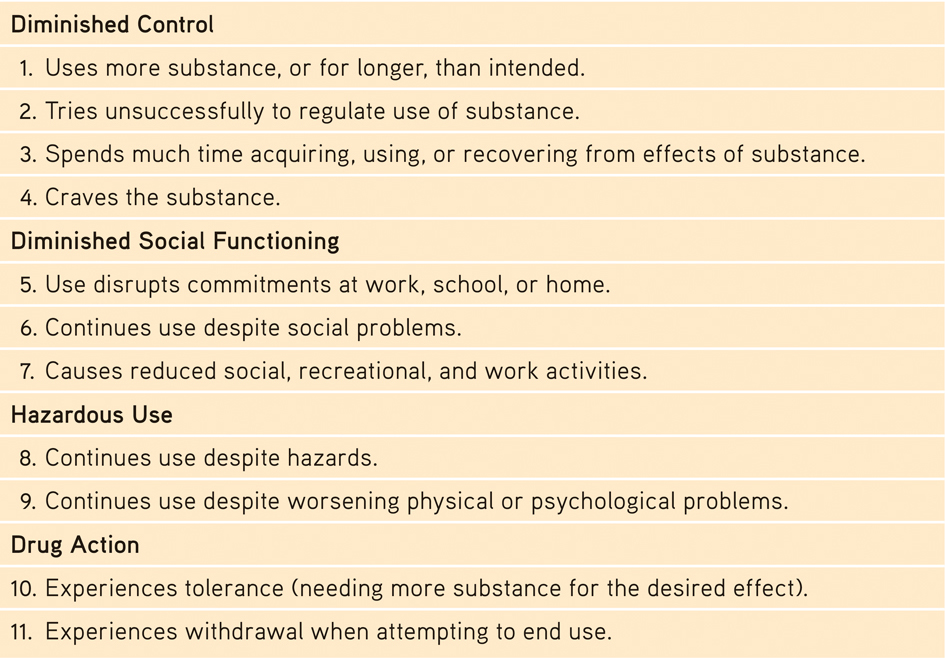
When Is Drug Use a Disorder?
According to the American Psychiatric Association, a person may be diagnosed with substance use disorder when drug use continues despite significant life disruption. Resulting brain changes may persist after quitting use of the substance (thus leading to strong cravings when exposed to people and situations that trigger memories of drug use). The severity of substance use disorder varies from mild (two to three of these indicators) to moderate (four to five indicators) to severe (six or more indicators). (Source: American Psychiatric Association, 2013.)
psychoactive drug a chemical substance that alters perceptions and moods.
118
tolerance the diminishing effect with regular use of the same dose of a drug, requiring the user to take larger and larger doses before experiencing the drug’s effect.
Why might a person who rarely drinks alcohol get buzzed on one can of beer while a long-
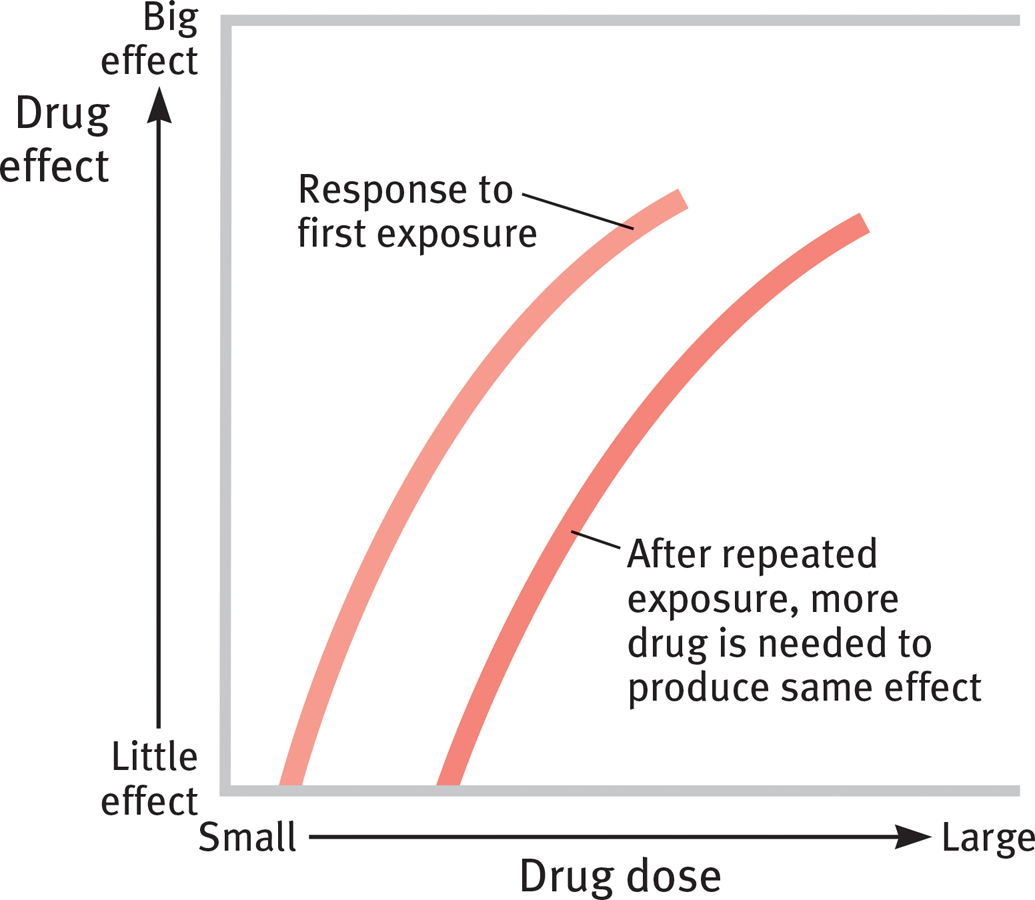
Drug tolerance
addiction compulsive craving of drugs or certain behaviors (such as gambling) despite known adverse consequences.
withdrawal the discomfort and distress that follow discontinuing an addictive drug or behavior.
THINKING CRITICALLY ABOUT
Addiction
3-13 How has the concept of addiction changed?
In recent years, the concept of addiction has been extended to cover many behaviors formerly considered bad habits or even sins. Psychologists debate whether the concept has been stretched too far, and whether addictions are really as irresistible as commonly believed. For example, “even for a very addictive drug like cocaine, only 15 to 16 percent of people become addicted within 10 years of first use,” observed Terry Robinson and Kent Berridge (2003).
Addictions can be powerful, and many addicts do benefit from therapy or group support. Alcoholics Anonymous has supported millions in overcoming alcohol addiction. But viewing addiction as an uncontrollable disease can undermine people’s self-confidence and their belief that they can change. And that, critics say, would be unfortunate, for many people do voluntarily stop using addictive drugs, without any treatment. Most ex-smokers, for example, have kicked the habit on their own (Newport, 2013).
The addiction-as-disease-needing-treatment idea has been offered for a host of driven, excessive behaviors—eating, gambling, work, sex, and accumulating wealth. However, critics suggest that “addiction” can become an all-purpose excuse when used not as a metaphor (“I’m a science fiction addict”) but as reality. Moreover, they note that labeling a behavior doesn’t explain it. Attributing serial adultery to a “sex addiction” does not explain the sexual impulsiveness (Radford, 2010).
Sometimes, though, behaviors such as gambling, video gaming, or online surfing do become compulsive and dysfunctional, much like abusive drug taking (Gentile, 2009; Griffiths, 2001; Hoeft et al., 2008). Thus, psychiatry’s manual of disorders now includes behavior addictions such as “gambling disorder” and proposes “Internet gaming disorder” for further study (American Psychiatric Association, 2013). Studies in Asia, Europe, and North America estimate gaming addiction rates of from 3 to 12 percent of players (Anderson et al., 2012; Ferguson et al., 2011). Some Internet users display an apparent inability to resist logging on, and staying on, even when this excessive use impairs their work and relationships (Ko et al., 2005). But there is hope. One research review found both psychological and drug therapies for Internet addiction “highly effective” (Winkler et al., 2013).
119
RETRIEVAL PRACTICE
- What is the process that leads to drug tolerance?
With repeated exposure to a psychoactive drug, the drug’s effect lessens. Thus, it takes bigger doses to get the desired effect.
Types of Psychoactive Drugs
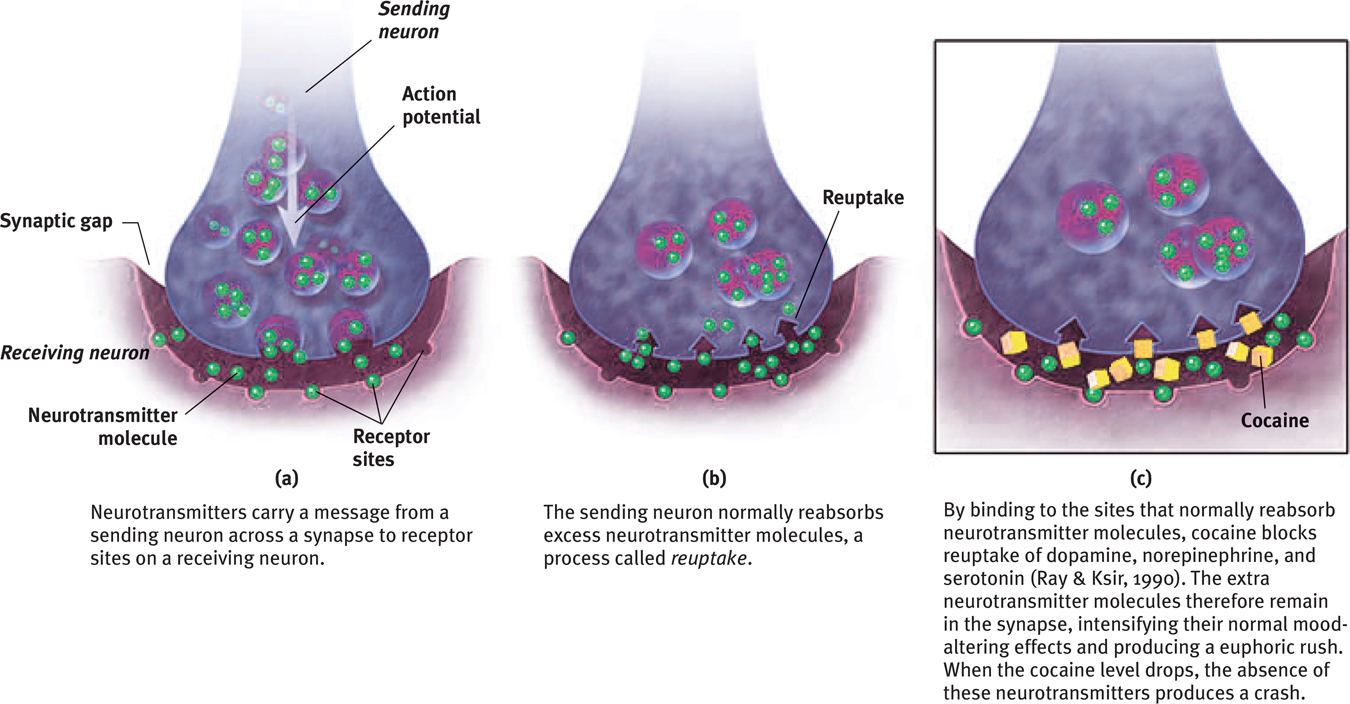
The three major categories of psychoactive drugs are depressants, stimulants, and hallucinogens. All do their work at the brain’s synapses, stimulating, inhibiting, or mimicking the activity of the brain’s own chemical messengers, the neurotransmitters.
Depressants
3-
depressants drugs (such as alcohol, barbiturates, and opiates) that reduce neural activity and slow body functions.
Depressants are drugs such as alcohol, barbiturates (tranquilizers), and opiates that calm neural activity and slow body functions.
Alcohol True or false? In small amounts, alcohol is a stimulant. False. Low doses of alcohol may, indeed, enliven a drinker, but they do so by acting as a disinhibitor—they slow brain activity that controls judgment and inhibitions. Alcohol is an equal-

SLOWED NEURAL PROCESSING Low doses of alcohol relax the drinker by slowing sympathetic nervous system activity. Larger doses cause reactions to slow, speech to slur, and skilled performance to deteriorate. Paired with sleep deprivation, alcohol is a potent sedative. Add these physical effects to lowered inhibitions, and the result can be deadly. Worldwide, several hundred thousand lives are lost each year in alcohol-
MEMORY DISRUPTION Alcohol can disrupt memory formation, and heavy drinking can also have long-
120
The prolonged and excessive drinking that characterizes alcohol use disorder can shrink the brain (FIGURE 3.21). Women, who have less of a stomach enzyme that digests alcohol, are especially vulnerable (Wuethrich, 2001). Girls and young women can become addicted to alcohol more quickly than boys and young men do, and they are at risk for lung, brain, and liver damage at lower consumption levels (CASA, 2003).
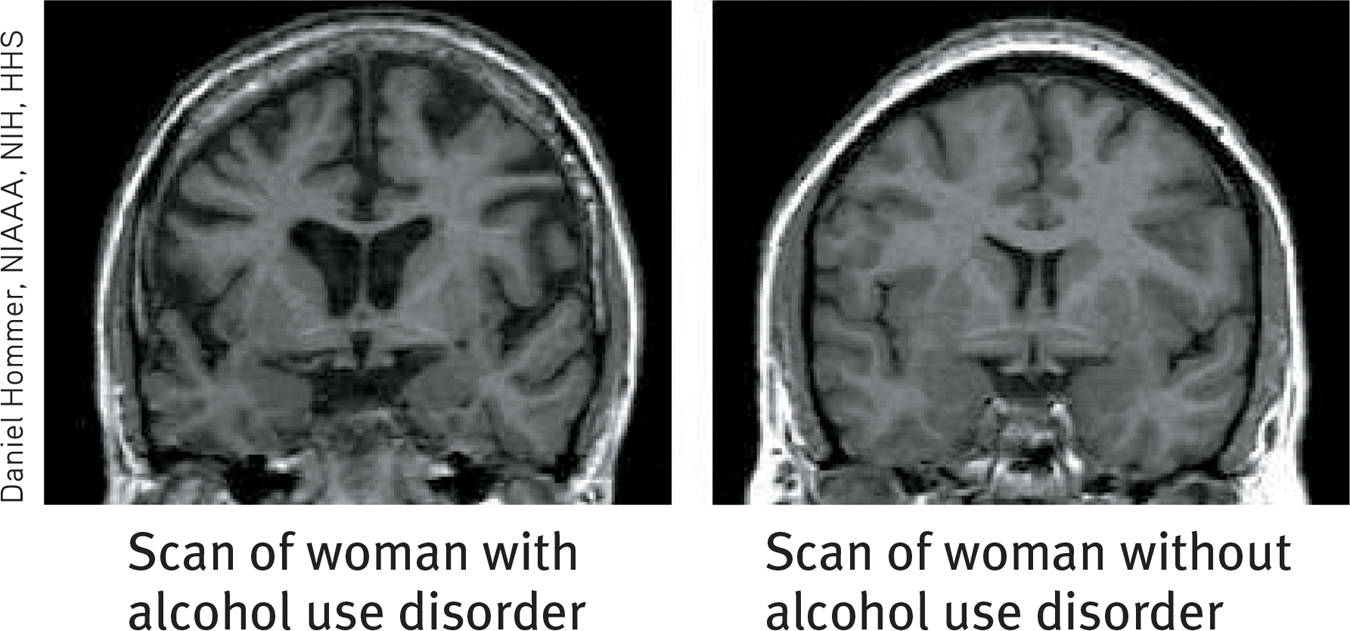
Disordered drinking shrinks the brain MRI scans show brain shrinkage in women with alcohol use disorder (left) compared with women in a control group (right).
alcohol use disorder (popularly known as alcoholism) alcohol use marked by tolerance, withdrawal, and a drive to continue problematic use.
REDUCED SELF-
Reduced self-
EXPECTANCY EFFECTS As with other psychoactive drugs, expectations influence behavior. When people believe that alcohol affects social behavior in certain ways, and believe they have been drinking alcohol, they will behave accordingly (Moss & Albery, 2009). In a now-
So, alcohol’s effect lies partly in that powerful sex organ, the mind. Fourteen “intervention studies” have educated college drinkers about that very point (Scott-
barbiturates drugs that depress central nervous system activity, reducing anxiety but impairing memory and judgment.
Barbiturates Like alcohol, the barbiturate drugs, or tranquilizers, depress nervous system activity. Barbiturates such as Nembutal, Seconal, and Amytal are sometimes prescribed to induce sleep or reduce anxiety. In larger doses, they can impair memory and judgment. If combined with alcohol—
opiates opium and its derivatives, such as morphine and heroin; depress neural activity, temporarily lessening pain and anxiety.
Opiates The opiates—opium and its derivatives—
121
RETRIEVAL PRACTICE
- How is a “shopping addiction” different from the psychological definition of addiction?
Being strongly interested in something in a way that is not compulsive and dysfunctional is not an addiction. It does not involve obsessive craving in spite of known negative consequences.
- Alcohol, barbiturates, and opiates are all in a class of drugs called ______________.
depressants
Stimulants
3-

stimulants drugs (such as caffeine, nicotine, and the more powerful amphetamines, cocaine, Ecstasy, and methamphetamine) that excite neural activity and speed up body functions.
A stimulant excites neural activity and speeds up body functions. Pupils dilate, heart and breathing rates increase, and blood sugar levels rise, causing a drop in appetite. Energy and self-
amphetamines drugs that stimulate neural activity, causing speeded-up body functions and associated energy and mood changes.
Stimulants include caffeine, nicotine, the amphetamines, cocaine, methamphetamine (“speed”), and Ecstasy. People use stimulants to feel alert, lose weight, or boost mood or athletic performance. Unfortunately, stimulants can be addictive, as you may know if you are one of the many who use caffeine daily in your coffee, tea, soda, or energy drinks. Cut off from your usual dose, you may crash into fatigue, headaches, irritability, and depression (Silverman et al., 1992). A mild dose of caffeine typically lasts three or four hours, which—
“There is an overwhelming medical and scientific consensus that cigarette smoking causes lung cancer, heart disease, emphysema, and other serious diseases in smokers. Smokers are far more likely to develop serious diseases, like lung cancer, than nonsmokers.”
Philip Morris Companies Inc., 1999
nicotine a stimulating and highly addictive psychoactive drug in tobacco.
Nicotine Cigarettes and other tobacco products deliver highly addictive nicotine. Imagine that cigarettes were harmless—
The lost lives from these dynamite-
For HIV patients who smoke, the virus is now much less lethal than the smoking (Helleberg et al., 2013).
Smoke a cigarette and nature will charge you 12 minutes—
“Smoking cures weight problems … eventually.”
Comedian-writer Steven Wright
Those drawn to nicotine find it very hard to quit, because tobacco products are powerfully and quickly addictive. Attempts to quit even within the first weeks of smoking often fail (DiFranza, 2008). As with other addictions, smokers develop tolerance, and quitting causes withdrawal symptoms, including craving, insomnia, anxiety, irritability, and distractibility. Nicotine-
“To cease smoking is the easiest thing I ever did; I ought to know because I’ve done it a thousand times.”
Mark Twain (1835–1910)
122
All it takes to relieve this aversive state is a single puff on a cigarette. Within 7 seconds, a rush of nicotine signals the central nervous system to release a flood of neurotransmitters (FIGURE 3.22). Epinephrine and norepinephrine diminish appetite and boost alertness and mental efficiency. Dopamine and opioids temporarily calm anxiety and reduce sensitivity to pain (Ditre et al., 2011; Scott et al., 2004). Thus, ex-
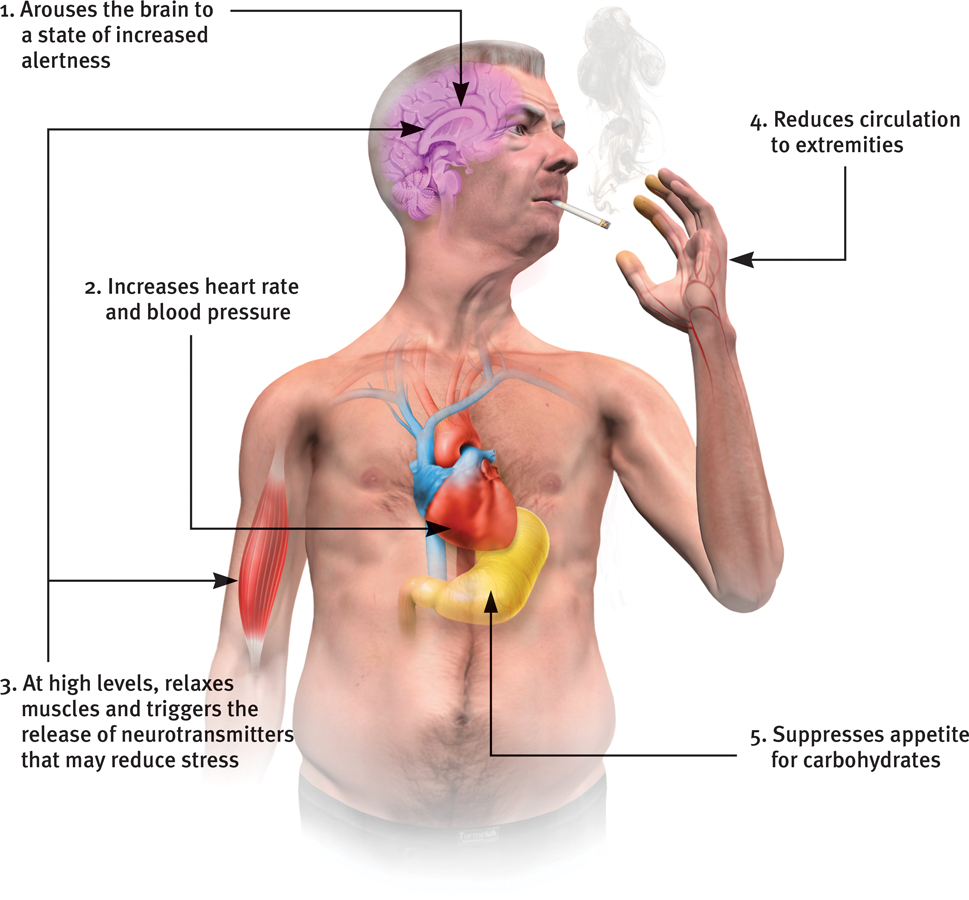
Where there’s smoke …: The physiological effects of nicotine Nicotine reaches the brain within 7 seconds, twice as fast as intravenous heroin. Within minutes, the amount in the blood soars.
Humorist Dave Barry (1995) recalling why he smoked his first cigarette the summer he turned 15: “Arguments against smoking: ‘It’s a repulsive addiction that slowly but surely turns you into a gasping, gray-skinned, tumor-ridden invalid, hacking up brownish gobs of toxic waste from your one remaining lung.’ Arguments for smoking: ‘Other teenagers are doing it.’ Case closed! Let’s light up!”
These rewards keep people smoking, even among the 3 in 4 smokers who wish they could stop (Newport, 2013). Each year, fewer than 1 in 7 smokers who want to quit will be able to resist. Even those who know they are committing slow-
Nevertheless, repeated attempts seem to pay off. Half of all Americans who have ever smoked have quit, sometimes aided by a nicotine replacement drug and with encouragement from a counselor or support group. Success is equally likely whether smokers quit abruptly or gradually (Fiore et al., 2008; Lichtenstein et al., 2010; Lindson et al., 2010). For those who endure, the acute craving and withdrawal symptoms gradually dissipate over the ensuing six months (Ward et al., 1997). After a year’s abstinence, only 10 percent will relapse in the next year (Hughes, 2010). These nonsmokers may live not only healthier but also happier lives. Smoking correlates with higher rates of depression, chronic disabilities, and divorce (Doherty & Doherty, 1998; Edwards & Kendler, 2012; Vita et al., 1998). Healthy living seems to add both years to life and life to years.
RETRIEVAL PRACTICE
- What withdrawal symptoms should your friend expect when she finally decides to quit smoking?
Your friend will likely experience strong craving, insomnia, anxiety, irritability, and distractibility. She’ll probably find it harder to concentrate. However, if she sticks with it, the craving and withdrawal symptoms will gradually dissipate over about six months.
123
cocaine a powerful and addictive stimulant derived from the coca plant; produces temporarily increased alertness and euphoria.
CocaineCocaine use offers a fast track from euphoria to crash. The recipe for Coca-
Cocaine euphoria and crash
“Cocaine makes you a new man. And the first thing that new man wants is more cocaine.”
Comedian George Carlin (1937–2008)
In situations that trigger aggression, ingesting cocaine may heighten reactions. Caged rats fight when given foot shocks, and they fight even more when given cocaine and foot shocks. Likewise, humans who voluntarily ingest high doses of cocaine in laboratory experiments impose higher shock levels on a presumed opponent than do those receiving a placebo (Licata et al., 1993). Cocaine use may also lead to emotional disturbances, suspiciousness, convulsions, cardiac arrest, or respiratory failure.
In national surveys, 3 percent of U.S. high school seniors and 6 percent of British 18-

Cocaine’s psychological effects depend in part on the dosage and form consumed, but the situation and the user’s expectations and personality also play a role. Given a placebo, cocaine users who thought they were taking cocaine often had a cocaine-
methamphetamine a powerfully addictive drug that stimulates the central nervous system, with speeded-up body functions and associated energy and mood changes; over time, appears to reduce baseline dopamine levels.
Methamphetamine Methamphetamine is chemically related to its parent drug, amphetamine (NIDA, 2002, 2005) but has greater effects. Methamphetamine triggers the release of the neurotransmitter dopamine, which stimulates brain cells that enhance energy and mood, leading to eight hours or so of heightened energy and euphoria. Its aftereffects may include irritability, insomnia, hypertension, seizures, social isolation, depression, and occasional violent outbursts (Homer et al., 2008). Over time, methamphetamine may reduce baseline dopamine levels, leaving the user with continuing depressed functioning.
124

Ecstasy (MDMA) a synthetic stimulant and mild hallucinogen. Produces euphoria and social intimacy, but with short-term health risks and longer-term harm to serotonin-producing neurons and to mood and cognition.
Ecstasy Ecstasy, a street name for MDMA (methylenedioxymetham-
During the 1990s, Ecstasy’s popularity soared as a “club drug” taken at nightclubs and all-
Hallucinogens
3-
hallucinogens psychedelic (“mind-manifesting”) drugs, such as LSD, that distort perceptions and evoke sensory images in the absence of sensory input.
Hallucinogens distort perceptions and evoke sensory images in the absence of sensory input (which is why these drugs are also called psychedelics, meaning “mind-
Whether provoked to hallucinate by drugs, loss of oxygen, or extreme sensory deprivation, the brain hallucinates in basically the same way (Siegel, 1982). The experience typically begins with simple geometric forms, such as a lattice, cobweb, or spiral. The next phase consists of more meaningful images; some may be superimposed on a tunnel or funnel, others may be replays of past emotional experiences. As the hallucination peaks, people frequently feel separated from their body and experience dreamlike scenes so real that they may become panic-
near-death experience an altered state of consciousness reported after a close brush with death (such as through cardiac arrest); often similar to drug-induced hallucinations.
These sensations are strikingly similar to the near-death experience, an altered state of consciousness reported by about 10 to 15 percent of patients revived from cardiac arrest (Agrillo, 2011; Greyson, 2010; Parnia et al., 2013). Many describe visions of tunnels (FIGURE 3.24), bright lights or beings of light, a replay of old memories, and out-
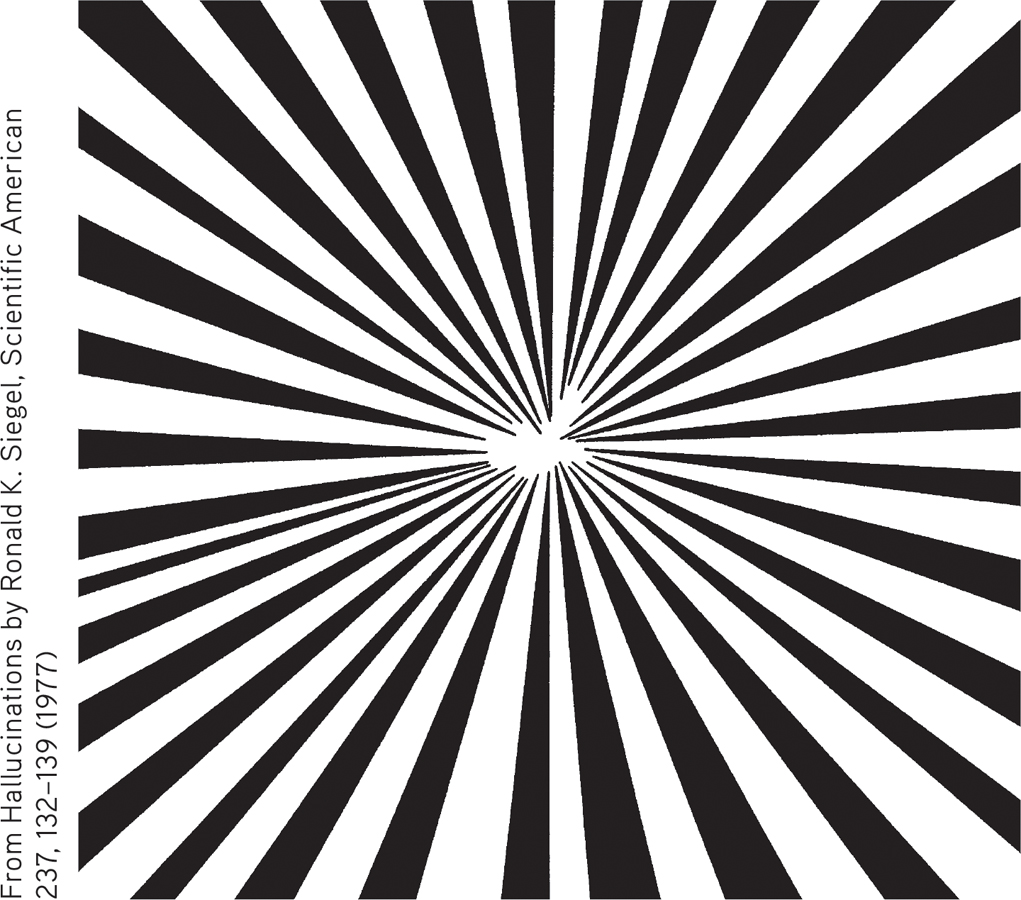
Near-
LSD a powerful hallucinogenic drug; also known as acid (lysergic acid diethylamide).
LSD Albert Hofmann, a chemist, created—
125
THC the major active ingredient in marijuana; triggers a variety of effects, including mild hallucinations.
Marijuana Marijuana leaves and flowers contain THC (delta-
Marijuana is a mild hallucinogen, amplifying sensitivity to colors, sounds, tastes, and smells. But like alcohol, marijuana relaxes, disinhibits, and may produce a euphoric high. Both alcohol and marijuana impair the motor coordination, perceptual skills, and reaction time necessary for safely operating an automobile or other machine. “THC causes animals to misjudge events,” reported Ronald Siegel (1990, p. 163). “Pigeons wait too long to respond to buzzers or lights that tell them food is available for brief periods; and rats turn the wrong way in mazes.”
Marijuana and alcohol also differ. The body eliminates alcohol within hours. THC and its by-
A marijuana user’s experience can vary with the situation. If the person feels anxious or depressed, marijuana may intensify the feelings. The more often the person uses marijuana, especially during adolescence, the greater the risk of anxiety, depression, or addiction (Bambico et al., 2010; Hurd et al., 2013; Murray et al., 2007).
Marijuana also disrupts memory formation and interferes with immediate recall of information learned only a few minutes before (Bossong et al., 2012). Such cognitive effects outlast the period of smoking (Messinis et al., 2006). Heavy adult use for over 20 years is associated with a shrinkage of brain areas that process memories and emotions (Yücel et al., 2008). One study, which has tracked more than 1000 New Zealanders from birth, found that the IQ scores of persistent teen marijuana users dropped eight points from age 13 to 38 (Meier et al., 2012). (This mental decline was seen only in those who started regular use before age 18, while their brains were still rapidly developing.) Prenatal exposure through maternal marijuana use impairs brain development (Berghuis et al., 2007; Huizink & Mulder, 2006).
 To review the basic psychoactive drugs and their actions, and to play the role of experimenter as you administer drugs and observe their effects, visit LaunchPad’s PsychSim 6: Your Mind on Drugs.
To review the basic psychoactive drugs and their actions, and to play the role of experimenter as you administer drugs and observe their effects, visit LaunchPad’s PsychSim 6: Your Mind on Drugs.
To free up resources to fight crime, some states and countries have passed laws legalizing the possession of small quantities of marijuana. In some cases, legal medical marijuana use has been granted to relieve the pain and nausea associated with diseases such as AIDS and cancer (Munsey, 2010; Watson et al., 2000). In such cases, the Institute of Medicine recommends delivering the THC with medical inhalers. Marijuana smoke, like cigarette smoke, is toxic and can cause cancer, lung damage, and pregnancy complications (BLF, 2012).
***
Despite their differences, the psychoactive drugs summarized in TABLE 3.4 below share a common feature: They trigger negative aftereffects that offset their immediate positive effects and grow stronger with repetition. And that helps explain both tolerance and withdrawal. As the opposing, negative aftereffects grow stronger, it takes larger and larger doses to produce the desired high (tolerance), causing the after-
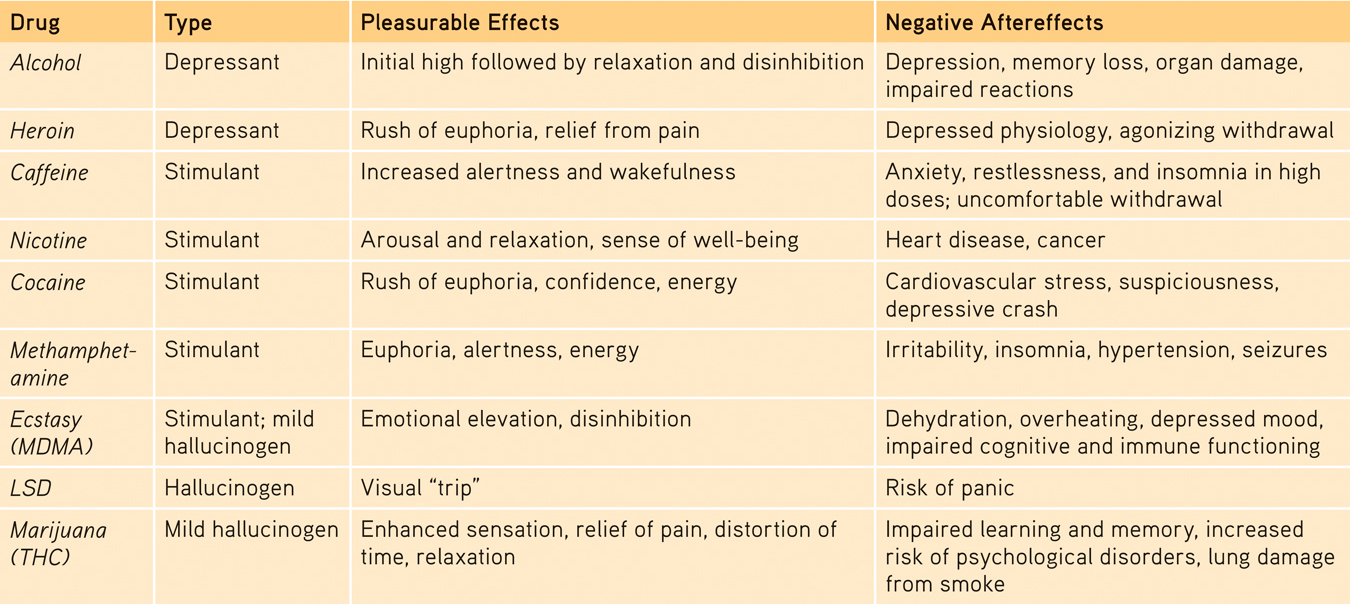
A Guide to Selected Psychoactive Drugs
126
RETRIEVAL PRACTICE
“How strange would appear to be this thing that men call pleasure! And how curiously it is related to what is thought to be its opposite, pain! … Wherever the one is found, the other follows up behind.”
Plato, Phaedo, fourth century b.c.e.
- How does this pleasure-pain description apply to the repeated use of psychoactive drugs?
Psychoactive drugs create pleasure by altering brain chemistry. With repeated use of the drug, the brain develops tolerance and needs more of the drug to achieve the desired effect. (Marijuana is an exception.) Discontinuing use of the substance then produces painful or psychologically unpleasant withdrawal symptoms.
Influences on Drug Use
3-
Drug use by North American youth increased during the 1970s. Then, with increased drug education and a more realistic and deglamorized media depiction of taking drugs, drug use declined sharply (except for a small rise in the mid-
- In the University of Michigan’s annual survey of 15,000 U.S. high school seniors, the proportion who said there is “great risk” in regular marijuana use rose from 35 percent in 1978 to 79 percent in 1991, then retreated to 40 percent in 2013 (Johnston et al., 2014).
- After peaking in 1978, marijuana use by U.S. high school seniors declined through 1992, then rose, but has recently been holding steady (see FIGURE 3.25). Among Canadian 15-
to 24- year- olds, 23 percent report using marijuana monthly, weekly, or daily (Health Canada, 2012). 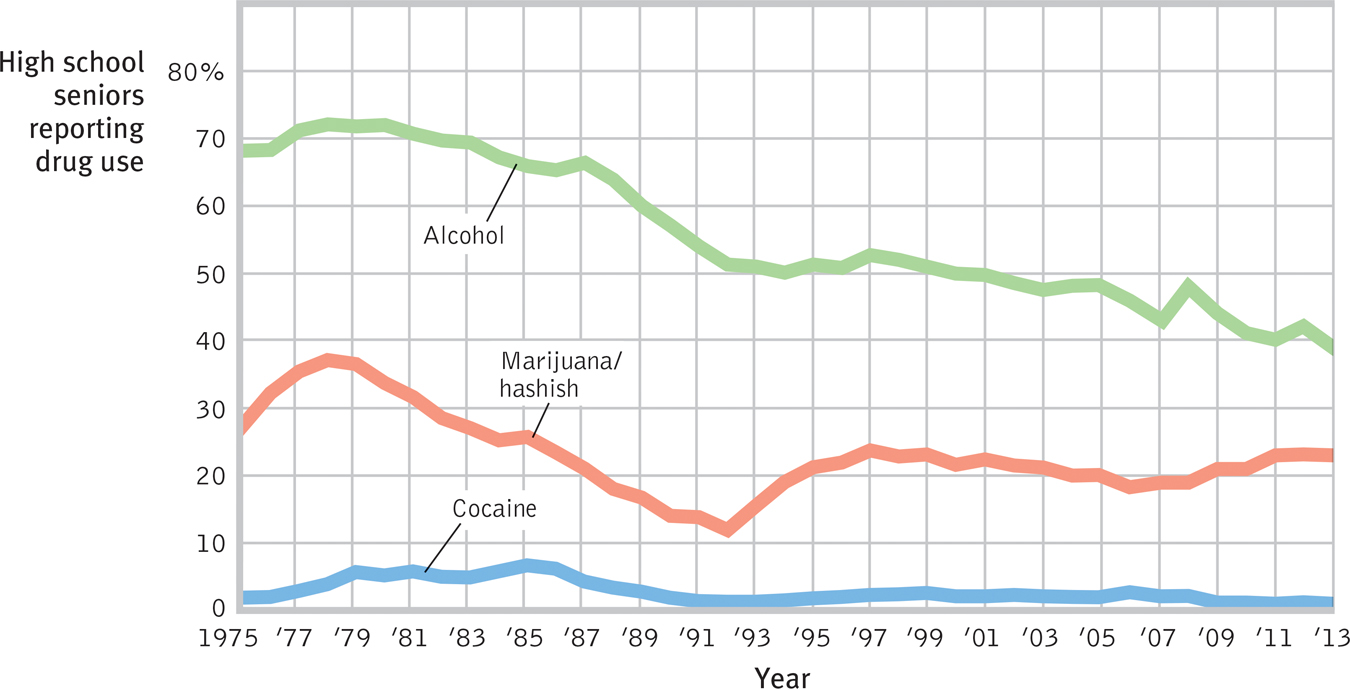
 FIGURE 3.25
FIGURE 3.25
Trends in drug use The percentage of U.S. high school seniors who report having used alcohol, marijuana, or cocaine during the past 30 days largely declined from the late 1970s to 1992, when it partially rebounded for a few years. (Data from Johnston et al., 2014.)
For some adolescents, occasional drug use represents thrill seeking. Why, though, do others become regular drug users? In search of answers, researchers have engaged biological, psychological, and social-
127
Biological Influences
Some people may be biologically vulnerable to particular drugs. For example, evidence accumulates that heredity influences some aspects of substance use problems, especially those appearing by early adulthood (Crabbe, 2002):
- Adopted individuals are more susceptible to alcohol use disorder if there is a history of it in one or both biological parents.
- Having an identical rather than fraternal twin with alcohol use disorder puts one at increased risk for alcohol problems (Kendler et al., 2002). In marijuana use also, identical twins more closely resemble each other than do fraternal twins.
- Boys who at age 6 are excitable, impulsive, and fearless (genetically influenced traits) are more likely as teens to smoke, drink, and use other drugs (Masse & Tremblay, 1997).
- Researchers have bred rats and mice that prefer alcoholic drinks to water. One such strain has reduced levels of the brain chemical NPY. Mice engineered to overproduce NPY are very sensitive to alcohol’s sedating effect and drink little (Thiele et al., 1998).
- Researchers have identified genes that are more common among people and animals predisposed to alcohol use disorder, and they are seeking genes that contribute to tobacco addiction (Stacey et al., 2012). These culprit genes seemingly produce deficiencies in the brain’s natural dopamine reward system: While triggering temporary dopamine-produced pleasure, the addictive drugs disrupt normal dopamine balance. Studies of how drugs reprogram the brain’s reward systems raise hopes for anti-addiction drugs that might block or blunt the effects of alcohol and other drugs (Miller, 2008; Wilson & Kuhn, 2005).
Warning signs of alcohol use disorder
- Drinking binges
- Craving alcohol
- Use results in unfulfilled work, school, or home tasks
- Failing to honor a resolve to drink less
- Continued use despite health risk
- Avoiding family or friends when drinking
Biological influences on drug use extend to other drugs as well. One study tracked 18,115 Swedish adoptees. Those with drug-
Psychological and Social-
Throughout this text, you will see that biological, psychological, and social-
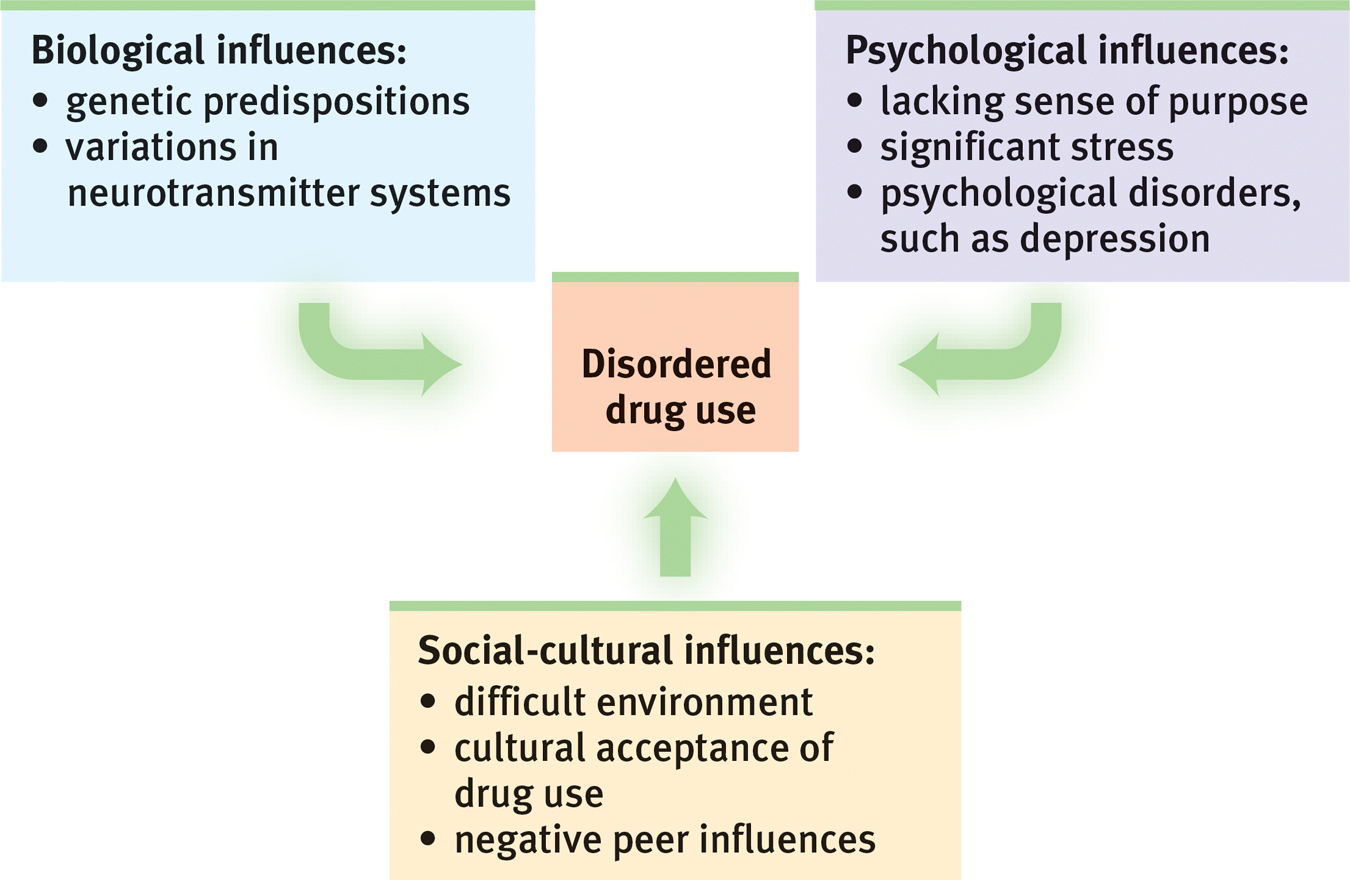
Levels of analysis for disordered drug use The biopsychosocial approach enables researchers to investigate disordered drug use from complementary perspectives.
128
Sometimes the psychological influence is obvious. Many heavy users of alcohol, marijuana, and cocaine have experienced significant stress or failure and are depressed. Girls with a history of depression, eating disorders, or sexual or physical abuse are at risk for substance addiction. So are youth undergoing school or neighborhood transitions (CASA, 2003; Logan et al., 2002). Collegians who have not yet achieved a clear identity are also at greater risk (Bishop et al., 2005). By temporarily dulling the pain of self-
Smoking usually begins during early adolescence. (If you are in college or university, and the cigarette manufacturers haven’t yet made you their devoted customer, they almost surely never will.) Adolescents, self-
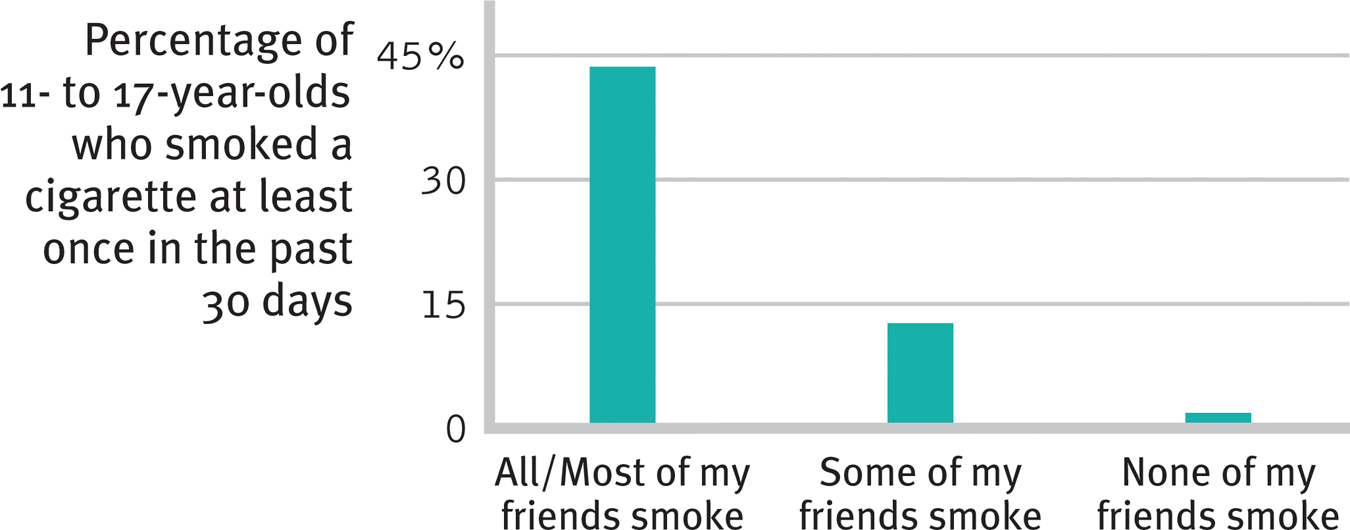
Peer influence Kids don’t smoke if their friends don’t (Philip Morris, 2003). A correlation-
Rates of drug use also vary across cultural and ethnic groups. One survey of 100,000 teens in 35 European countries found that marijuana use in the prior 30 days ranged from zero to 1 percent in Romania and Sweden to 20 to 22 percent in Britain, Switzerland, and France (ESPAD, 2003). Independent U.S. government studies of drug use in households nationwide and among high schoolers in all regions reveal that African-
129
Whether in cities or rural areas, peers influence attitudes about drugs. They also throw the parties and provide (or don’t provide) the drugs. If an adolescent’s friends use drugs, the odds are that he or she will, too. If the friends do not, the opportunity may not even arise. Teens who come from happy families, who do not begin drinking before age 15, and who do well in school tend not to use drugs, largely because they rarely associate with those who do (Bachman et al., 2007; Hingson et al., 2006; Odgers et al., 2008).
Peer influence is more than what friends do or say. Adolescents’ expectations—
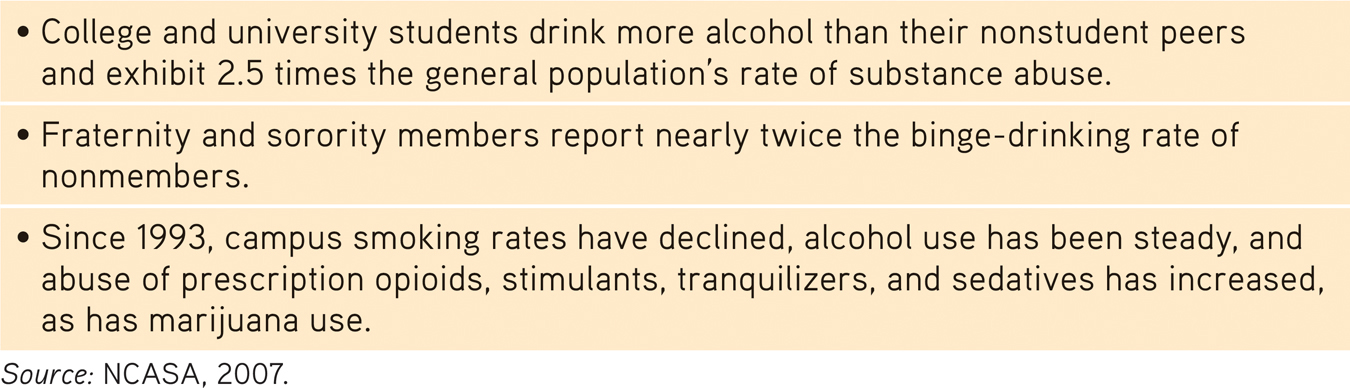
Facts About “Higher” Education
People whose beginning use of drugs was influenced by their peers are more likely to stop using when friends stop or their social network changes (Kandel & Raveis, 1989). One study that followed 12,000 adults over 32 years found that smokers tend to quit in clusters (Christakis & Fowler, 2008). Within a social network, the odds of a person quitting increased when a spouse, friend, or co-
As always with correlations, the traffic between friends’ drug use and our own may be two-
What do the findings on drug use suggest for drug prevention and treatment programs? Three channels of influence seem possible:
- Educate young people about the long-term costs of a drug’s temporary pleasures.
- Help young people find other ways to boost their self-esteem and purpose in life.
- Attempt to modify peer associations or to “inoculate” youths against peer pressures by training them in refusal skills.
130
People rarely abuse drugs if they understand the physical and psychological costs, feel good about themselves and the direction their lives are taking, and are in a peer group that disapproves of using drugs. These educational, psychological, and social-
RETRIEVAL PRACTICE
- Why do tobacco companies try so hard to get customers hooked as teens?
Nicotine is powerfully addictive, expensive, and deadly. Those who start paving the neural pathways when young may find it very hard to stop using nicotine. As a result, tobacco companies may have lifelong customers.
- Studies have found that people who begin drinking in their early teens are much more likely to develop alcohol use disorder than those who begin at age 21 or after. What possible explanations might there be for this correlation?
Possible explanations include (a) a biological predisposition to both early use and later abuse; (b) brain changes and taste preferences triggered by early use; and (c) enduring habits, attitudes, activities, or peer relationships that foster alcohol misuse.
REVIEW: Drugs and Consciousness

|
REVIEW | Drugs and Consciousness |
LEARNING OBJECTIVES
RETRIEVAL PRACTICE Take a moment to answer each of these Learning Objective Questions (repeated here from within this section). Then click the 'show answer' button to check your answers. Research suggests that trying to answer these questions on your own will improve your long-
3-
Those with a substance use disorder may exhibit impaired control, social disruption, risky behavior, and the physical effects of tolerance and withdrawal. Psychoactive drugs alter perceptions and moods. They may produce tolerance—requiring larger doses to achieve the desired effect—and withdrawal—significant discomfort accompanying attempts to quit. Continued use may lead to addiction, which is the compulsive craving of drugs or certain behaviors (such as gambling) despite known adverse consequences.
3-
Psychologists debate whether the concept of addiction has been stretched too far, and whether addictions are really as irresistible as commonly believed. Addictions can be powerful, and many with addictions do benefit from therapy or group support. But viewing addiction as an uncontrollable disease can undermine people’s self-confidence and their belief that they can change. The addiction-as-disease-needing-treatment idea has been extended to a host of excessive, driven behaviors, but labeling a behavior doesn’t explain it. The concept of addiction continues to evolve, as psychiatry’s manual of disorders now includes behavior addictions such as “gambling disorder” and proposes “Internet gaming disorder” for further study.
3-
Depressants, such as alcohol, barbiturates, and the opiates, dampen neural activity and slow body functions. Alcohol tends to disinhibit, increasing the likelihood that we will act on our impulses, whether harmful or helpful. It also impairs judgment, disrupts memory processes by suppressing REM sleep, and reduces self-awareness and self-control. User expectations strongly influence alcohol’s behavioral effects.
3-
Stimulants—including caffeine, nicotine, cocaine, the amphetamines, methamphetamine, and Ecstasy—excite neural activity and speed up body functions, triggering energy and mood changes. All are highly addictive. Nicotine’s effects make smoking a difficult habit to kick, yet the percentage of Americans who smoke has been dramatically decreasing. Cocaine gives users a fast high, followed within an hour by a crash. Its risks include cardiovascular stress and suspiciousness. Use of methamphetamines may permanently reduce dopamine production. Ecstasy (MDMA) is a combined stimulant and mild hallucinogen that produces euphoria and feelings of intimacy. Its users risk immune system suppression, permanent damage to mood and memory, and (if taken during physical activity) dehydration and escalating body temperatures.
3-
Hallucinogens—such as LSD and marijuana—distort perceptions and evoke hallucinations—sensory images in the absence of sensory input. The user’s mood and expectations influence the effects of LSD, but common experiences are hallucinations and emotions varying from euphoria to panic. Marijuana’s main ingredient, THC, may trigger feelings of disinhibition, euphoria, relaxation, relief from pain, and intense sensitivity to sensory stimuli. It may also increase feelings of depression or anxiety, impair motor coordination and reaction time, disrupt memory formation, and damage lung tissue (because of the inhaled smoke).
3-
Some people may be biologically vulnerable to particular drugs, such as alcohol. Psychological factors (such as stress, depression, and hopelessness) and social factors (such as peer pressure) combine to lead many people to experiment with—and sometimes become addicted to—drugs. Cultural and ethnic groups have differing rates of drug use. Each type of influence—biological, psychological, and social-cultural—offers a possible path for drug misuse prevention and treatment programs.
TERMS AND CONCEPTS TO REMEMBER
RETRIEVAL PRACTICE Match each of the terms on the left with its definition on the right. Click on the term first and then click on the matching definition. As you match them correctly they will move to the bottom of the activity.
Question
substance use disorder psychoactive drug tolerance addiction withdrawal depressants alcohol use disorder barbiturates opiates stimulants amphetamines nicotine cocaine methamphetamine Ecstasy (MDMA) hallucinogens near-death experience LSD THC | opium and its derivatives, such as morphine and heroin; depress neural activity, temporarily lessening pain and anxiety. psychedelic (“mind-manifesting”) drugs, such as LSD, that distort perceptions and evoke sensory images in the absence of sensory input. a chemical substance that alters perceptions and moods. the diminishing effect with regular use of the same dose of a drug, requiring the user to take larger and larger doses before experiencing the drug’s effect. compulsive craving of drugs or certain behaviors (such as gambling) despite known adverse consequences. a powerfully addictive drug that stimulates the central nervous system, with speeded-up body functions and associated energy and mood changes; over time, appears to reduce baseline dopamine levels. the discomfort and distress that follow discontinuing an addictive drug or behavior. a synthetic stimulant and mild hallucinogen. Produces euphoria and social intimacy, but with short-term health risks and longer-term harm to serotonin-producing neurons and to mood and cognition. drugs that stimulate neural activity, causing speeded-up body functions and associated energy and mood changes. (popularly known as alcoholism) alcohol use marked by tolerance, withdrawal, and a drive to continue problematic use. a powerful and addictive stimulant derived from the coca plant; produces temporarily increased alertness and euphoria. continued substance craving and use despite significant life disruption and/or physical risk. a powerful hallucinogenic drug; also known as acid (lysergic acid diethylamide). drugs that depress central nervous system activity, reducing anxiety but impairing memory and judgment. drugs (such as alcohol, barbiturates, and opiates) that reduce neural activity and slow body functions. an altered state of consciousness reported after a close brush with death (such as through cardiac arrest); often similar to drug-induced hallucinations. drugs (such as caffeine, nicotine, and the more powerful amphetamines, cocaine, Ecstasy, and methamphetamine) that excite neural activity and speed up body functions. a stimulating and highly addictive psychoactive drug in tobacco. the major active ingredient in marijuana; triggers a variety of effects, including mild hallucinations. |
Use  to create your personalized study plan, which will direct you to the resources that will help you most in
.
to create your personalized study plan, which will direct you to the resources that will help you most in
.
131
TEST
YOUR-
SELF CONSCIOUSNESS AND THE TWO-TRACK MIND
Test yourself repeatedly throughout your studies. This will not only help you figure out what you know and don’t know; the testing itself will help you learn and remember the information more effectively thanks to the testing effect.
 Brain States and Consciousness
Brain States and Consciousness
Question
1. Failure to see visible objects because our attention is occupied elsewhere is called refers to our tendency to perceive events as obvious or inevitable after the fact.
Question
2. We register and react to stimuli outside of our awareness by means of processing. When we devote deliberate attention to stimuli, we use processing.
Question
3. blindness and change blindness are forms of selective attention.
Sleep and Dreams
Question
4. Our body temperature tends to rise and fall in sync with a biological clock, which is referred to as .
Question
5. During the NREM-1 sleep stage, a person is most likely to experience
| A. |
| B. |
| C. |
| D. |
Question
6. The brain emits large, slow delta waves during sleep.
Question
7. As the night progresses, what happens to the REM stage of sleep?
It increases in duration.
Question
8. Which of the following is NOT one of the reasons that have been proposed to explain why we need sleep?
| A. |
| B. |
| C. |
| D. |
Question
9. What is the difference between narcolepsy and sleep apnea?
With narcolepsy, the person periodically falls directly into REM sleep, with no warning; with sleep apnea, the person repeatedly awakens during the night.
Question
10. In interpreting dreams, Freud was most interested in their
| A. |
| B. |
| C. |
| D. |
Question
11. What is the neural activation theory of dreaming?
The neural activation theory suggests that dreams are the brain’s attempt to make sense of random neural activity.
Question
12. “For what one has dwelt on by day, these things are seen in visions of the night” (Menander of Athens, Fragments). How might the information-processing perspective on dreaming interpret this ancient Greek quote?
The information-processing explanation of dreaming proposes that brain activity during REM sleep enables us to sift through what one has dwelt on by day.
Question
13. The tendency for REM sleep to increase following REM sleep deprivation is referred to as .
Drugs and Consciousness
Question
14. After continued use of a psychoactive drug, the drug user needs to take larger doses to get the desired effect. This is referred to as .
Question
15. The depressants include alcohol, barbiturates,
| A. |
| B. |
| C. |
| D. |
Question
16. Why might alcohol make a person more helpful or more aggressive?
Alcohol is a disinhibitor—it makes us more likely to do what we would have done when sober, whether that is being helpful or being aggressive.
Question
17. The depressants include alcohol, barbiturates,
| A. |
| B. |
| C. |
| D. |
Question
18. Near-death experiences are strikingly similar to the hallucinations evoked by .
Question
19. Use of marijuana
| A. |
| B. |
| C. |
| D. |
Question
20. An important psychological contributor to drug use is
| A. |
| B. |
| C. |
| D. |