12.5 Health and Coping
Promoting health begins with implementing strategies that prevent illness and enhance wellness. Traditionally, people have thought about their health only when something goes wrong—
Coping With Stress
coping alleviating stress using emotional, cognitive, or behavioral methods.
problem-
12-
emotion-
Stressors are unavoidable. This fact, coupled with the fact that persistent stress correlates with heart disease, depression, and lowered immunity, gives us a clear message. We need to learn to cope with the stress in our lives, alleviating it with emotional, cognitive, or behavioral methods. We address some stressors directly, with problem-
501
When challenged, some of us tend to respond with cool problem-
Personal Control
12-
Picture the scene: Two rats receive simultaneous shocks. One can turn a wheel to stop the shocks (as illustrated in FIGURE 12.28). The helpless rat, but not the wheel turner, becomes more susceptible to ulcers and lowered immunity to disease (Laudenslager & Reite, 1984). In humans, too, uncontrollable threats trigger the strongest stress responses (Dickerson & Kemeny, 2004).
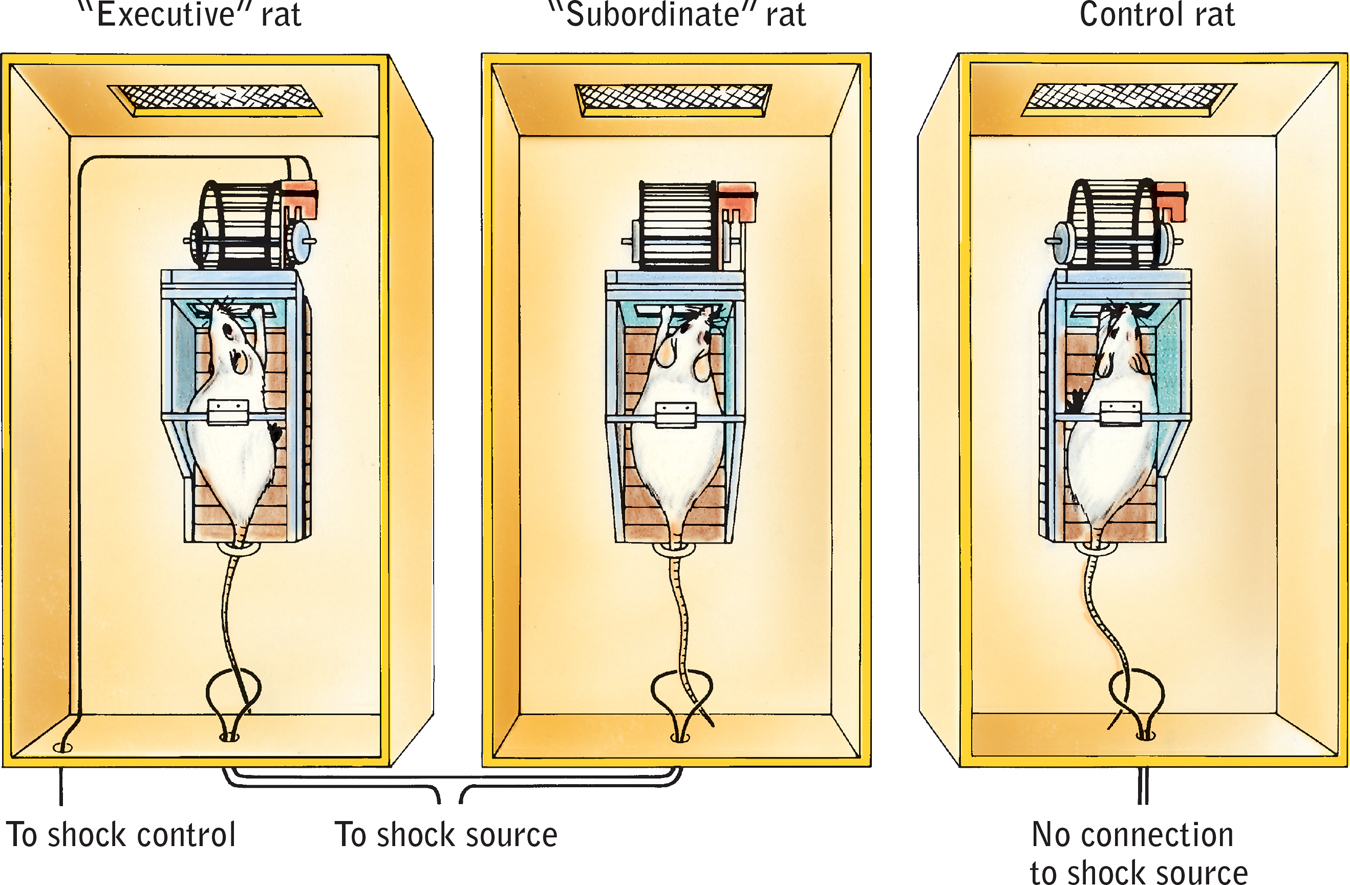
Health consequences of a loss of control The “executive” rat at the left can switch off the tail shock by turning the wheel. Because it has control over the shock, it is no more likely to develop ulcers than is the unshocked control rat on the right. The “subordinate” rat in the center receives the same shocks as the executive rat, but with no control over the shocks. It is, therefore, more likely to develop ulcers. (Adapted from Weiss, 1977.)
learned helplessness the hopelessness and passive resignation an animal or human learns when unable to avoid repeated aversive events.
At times, we all feel helpless, hopeless, and depressed after experiencing a series of bad events beyond our control. Martin Seligman and his colleagues have shown that for some animals and people, a series of uncontrollable events creates a state of learned helplessness, with feelings of passive resignation (FIGURE 12.29). In one series of experiments, dogs were strapped in a harness and given repeated shocks, with no opportunity to avoid them (Seligman & Maier, 1967). Later, when placed in another situation where they could escape the punishment by simply leaping a hurdle, the dogs cowered as if without hope. Other dogs that had been able to escape the first shocks reacted differently. They had learned they were in control and easily escaped the shocks in the new situation (Seligman & Maier, 1967). In other experiments, people have shown similar patterns of learned helplessness (Abramson et al., 1978, 1989; Seligman, 1975).

Learned helplessness When animals and people experience no control over repeated bad events, they often learn helplessness.
Perceiving a loss of control, we become more vulnerable to ill health. A famous study of elderly nursing home residents with little perceived control over their activities found that they declined faster and died sooner than those given more control (Rodin, 1986). Workers able to adjust office furnishings and control interruptions and distractions in their work environment have also experienced less stress (O’Neill, 1993). Such findings help explain why British civil service workers at the executive grades have tended to outlive those at clerical or laboring grades, and why Finnish workers with low job stress have been less than half as likely to die of strokes or heart disease as were those with a demanding job and little control. The more control workers have, the longer they live (Bosma et al., 1997, 1998; Kivimaki et al., 2002; Marmot et al., 1997).
Control also helps explain a link between economic status and longevity (Jokela et al., 2009). In one study of 843 grave markers in an old graveyard in Glasgow, Scotland, those with the costliest, highest pillars (indicating the most affluence) tended to have lived the longest (Carroll et al., 1994). Likewise, those living in Scottish regions with the least overcrowding and unemployment have the greatest longevity. There and elsewhere, high economic status predicts a lower risk of heart and respiratory diseases (Sapolsky, 2005). Wealth predicts better health among children, too (Chen, 2004). With higher economic status come reduced risks of low birth weight, infant mortality, smoking, and violence. Even among other primates, those at the bottom of the social pecking order have been more likely than their higher-
502
Why does perceived loss of control predict health problems? Because losing control provokes an outpouring of stress hormones. When rats cannot control shock or when primates or humans feel unable to control their environment, stress hormone levels rise, blood pressure increases, and immune responses drop (Rodin, 1986; Sapolsky, 2005). One study found these effects among nurses, who reported their workload and their level of personal control on the job. The greater their workload, the higher their cortisol level and blood pressure—
Increasing control—
In the case of nursing home patients, 93 percent of those who were encouraged to exert more control became more alert, active, and happy (Rodin, 1986). As researcher Ellen Langer concluded, “Perceived control is basic to human functioning” (1983, p. 291). “For the young and old alike,” she suggested, environments should enhance people’s sense of control over their world. No wonder mobile devices and DVRs, which enhance our control of the content and timing of our entertainment, are so popular.

Google incorporates these principles effectively. Each week, Google employees can spend 20 percent of their working time on projects they find personally interesting. This Innovation Time Off program increases employees’ personal control over their work environment, and it has paid off. Gmail was developed this way.
People thrive when they live in conditions of personal freedom and empowerment. At the national level, citizens of stable democracies report higher levels of happiness (Inglehart et al., 2008).
So, some freedom and control are better than none. But does ever-
external locus of control the perception that chance or outside forces beyond our personal control determine our fate.
Internal Versus External Locus of Control If experiencing a loss of control can be stressful and unhealthy, do people who generally feel in control of their lives enjoy better health? Consider your own feelings of control. Do you believe that your life is beyond your control? That the world is run by a few powerful people? That getting a good job depends mainly on being in the right place at the right time? Or do you more strongly believe that you control your own fate? That each of us can influence our government’s decisions? That being a success is a matter of hard work?
internal locus of control the perception that we control our own fate.
503
Hundreds of studies have compared people who differ in their perceptions of control. On the one side are those who have what Julian Rotter called an external locus of control, the perception that chance or outside forces control their fate. On the other side are those who perceive an internal locus of control, who believe they control their own destiny. In study after study, the “internals” have achieved more in school and work, acted more independently, enjoyed better health, and felt less depressed than did the “externals” (Lefcourt, 1982; Ng et al., 2006). In one long-
Another way to say that we believe we are in control of our own life is to say we have free will, or that we can control our own willpower. Studies show that people who believe in their freedom learn better, perform better at work, behave more helpfully, and have a stronger desire to punish rule breakers (Clark et al., 2014; Job et al., 2010; Stillman et al., 2010).
Compared with their parents’ generation, more young Americans now endorse an external locus of control (Twenge et al., 2004). This shift may help explain an associated increase in rates of depression and other psychological disorders in young people (Twenge et al., 2010).
RETRIEVAL PRACTICE
- To cope with stress, we tend to use ______________ -focused (emotion/problem) strategies when we feel in control of our world, and ______________ -focused (emotion/problem) strategies when we believe we cannot change a situation.
problem; emotion
self-
Depleting and Strengthening Self-
12-
Self-
Self-
Exercising willpower decreases neural activation in regions associated with mental control (Wagner et al., 2013). Might sugar provide a sweet solution to self-
504
Researchers do not encourage candy bar diets to improve self-
Decreased mental energy after exercising self-
The point to remember: Develop self-
Explanatory Style: Optimism Versus Pessimism
12-
In The How of Happiness, psychologist Sonja Lyubomirsky (2008) tells the true story of Randy. By any measure, Randy lived a hard life. His dad and best friend died by suicide. Growing up, his mother’s boyfriend treated him poorly. Randy’s own first marriage was troubled. His wife was unfaithful, and they divorced. Despite these setbacks, Randy is a happy person whose presence can light up a room. He remarried and enjoys his role as stepfather to three boys. He also finds his work life to be rewarding. Randy says he survived his life challenges by seeing the “silver lining in the cloud.”
Randy’s story illustrates how our outlook—
Optimistic students have also tended to get better grades because they often respond to setbacks with the hopeful attitude that effort, good study habits, and self-
Consider the consistency and startling magnitude of the optimism and positive emotions factor in several other studies:
- One research team followed 941 Dutch people, ages 65 to 85, for nearly a decade (Giltay et al., 2004, 2007). Among those in the lowest optimism quartile, 57 percent died, as did only 30 percent of the top optimism quartile.
 Positive expectations often motivate eventual success.
Positive expectations often motivate eventual success. - When Finnish researchers followed 2428 men for up to a decade, the number of deaths among those with a bleak, hopeless outlook was more than double that found among their optimistic counterparts (Everson et al., 1996). American researchers found the same when following 4256 Vietnam-
era veterans (Phillips et al., 2009). - A now-
famous study followed up on 180 Catholic nuns who had written brief autobiographies at about 22 years of age and had thereafter lived similar lifestyles. Those who had expressed happiness, love, and other positive feelings in their autobiographies lived an average 7 years longer than their more dour counterparts (Danner et al., 2001). By age 80, some 54 percent of those expressing few positive emotions had died, as had only 24 percent of the most positive spirited.
505
Optimism runs in families, so some people truly are born with a sunny, hopeful outlook. With identical twins, if one is optimistic, the other often will be as well (Mosing et al., 2009). One genetic marker of optimism is a gene that enhances the social-
The good news is that all of us, even the most pessimistic, can learn to become more optimistic. Compared with pessimists who simply kept diaries of their daily activities, those who became skilled at seeing the bright side of difficult situations and viewing their goals as achievable reported lower levels of depression (Sergeant & Mongrain, 2014). Optimism is the light bulb that can brighten anyone’s mood.
“The optimist proclaims we live in the best of all possible worlds, and the pessimist fears this is true.”
James Branch Cabell, The Silver Stallion, 1926
Social Support
12-
Social support—
People need people. Some fill this need by connecting with friends, family, co-
506

What explains the link between social support and health? Are middle-
Social support calms us and reduces blood pressure and stress hormones. Numerous studies support this finding (Hostinar et al., 2014; Uchino et al., 1996, 1999). To see if social support might calm people’s response to threats, one research team subjected happily married women, while lying in an fMRI machine, to the threat of electric shock to an ankle (Coan et al., 2006). During the experiment, some women held their husband’s hand. Others held the hand of an unknown person or no hand at all. While awaiting the occasional shocks, women holding their husband’s hand showed less activity in threat-
Social support fosters stronger immune functioning. Volunteers in studies of resistance to cold viruses showed this effect (Cohen et al., 1997, 2004). Healthy volunteers inhaled nasal drops laden with a cold virus and were quarantined and observed for five days. (In these experiments, more than 600 volunteers received $800 each to endure this experience.) Age, race, sex, smoking, and other health habits being equal, those with the most social ties were least likely to catch a cold. If they did catch one, they produced less mucus. More sociability meant less susceptibility. The cold fact is that the effect of social ties is nothing to sneeze at!
Close relationships give us an opportunity for “open heart therapy,” a chance to confide painful feelings (Frattaroli, 2006). Talking about a stressful event can temporarily arouse us, but in the long run it calms us, by calming limbic system activity (Lieberman et al., 2007; Mendolia & Kleck, 1993). In one study, 33 Holocaust survivors spent two hours recalling their experiences, many in intimate detail never before disclosed (Pennebaker et al., 1989). In the weeks following, most watched a tape of their recollections and showed it to family and friends. Those who were most self-
“Woe to one who is alone and falls and does not have another to help.”
Ecclesiastes 4:10
Suppressing emotions can be detrimental to physical health. When health psychologist James Pennebaker (1985) surveyed more than 700 undergraduate women, about 1 in 12 of them reported a traumatic sexual experience in childhood. The sexually abused women—
507
Even writing about personal traumas in a diary can help (Burton & King, 2008; Hemenover, 2003; Lyubomirsky et al., 2006). In an analysis of 633 trauma victims, writing therapy was as effective as psychotherapy in reducing psychological trauma (van Emmerik et al., 2013). In another experiment, volunteers who wrote trauma diaries had fewer health problems during the ensuing four to six months (Pennebaker, 1990). As one participant explained, “Although I have not talked with anyone about what I wrote, I was finally able to deal with it, work through the pain instead of trying to block it out. Now it doesn’t hurt to think about it.”
If we are aiming to exercise more, drink less, quit smoking, or be a healthy weight, our social ties can tug us away from or toward our goal. If you are trying to achieve some goal, think about whether your social network can help or hinder you. That social net covers not only the people you know but friends of your friends, and friends of their friends. That’s three degrees of separation between you and the most remote people. Within that network, others can influence your thoughts, feelings, and actions without your awareness (Christakis & Fowler, 2009). Obesity, for example, spreads within networks in ways that seem not merely to reflect people’s seeking out similar others.
Question
KKmgj2Q2WDPp9JM/5A9J4kb0sH3IbPDn/NsSbM5uUyTy3Gy2DMjhdHB7qiXggQxHSASI+1a7bc20wRelmDYVSPgjDO7YLR0g7mG9dLsca8E5WZJ05yCFMCm4TGPKyfkkUv9SwXd+5Wwg2qOzYgy3fJozRzZlEtyvUknkdMbnpWNMtGf0OEgtfMa8IAcaPhMH8UOSfe0pBspE3f16MBgYCqXE/9uSw6wv1SV6YU5U8HCMXkrjjKuFb682vDS9avXi4qhoAV2HbU0ksAmbReducing Stress
Having a sense of control, developing more optimistic thinking, and building social support can help us experience less stress and thus improve our health. Moreover, these factors interrelate: People who have been upbeat about themselves and their future have tended also to enjoy health-
aerobic exercise sustained exercise that increases heart and lung fitness; may also alleviate depression and anxiety.
Aerobic Exercise
12-
Aerobic exercise is sustained, oxygen-
Exercise helps fight heart disease by strengthening the heart, increasing bloodflow, keeping blood vessels open, and lowering both blood pressure and the blood pressure reaction to stress (Ford, 2002; Manson, 2002). Compared with inactive adults, people who exercise suffer half as many heart attacks (Powell et al., 1987; Visich & Fletcher, 2009). Exercise makes the muscles hungry for the fats that, if not used by the muscles, contribute to clogged arteries (Barinaga, 1997). In one study of over 650,000 American adults, walking 150 minutes per week predicted living seven more years (Moore et al., 2012). People who avoid sedentary activities, such as watching television, also tend to live longer lives (Veerman et al., 2012; Wilmot et al., 2012).
The genes passed down to us from our distant ancestors were those that enabled the physical activity essential to hunting, foraging, and farming (Raichlen & Polk, 2013). In muscle cells, those genes, when activated by exercise, respond by producing proteins. In the modern inactive person, these genes produce lower quantities of proteins and leave us susceptible to more than 20 chronic diseases, such as type 2 diabetes, coronary heart disease, stroke, Alzheimer’s disease, and cancer (Booth & Neufer, 2005). Inactivity is thus potentially toxic. But physical activity can weaken the influence of some genetic risk factors. In one analysis of 45 studies, the risk of obesity fell by 27 percent (Kilpeläinen et al., 2012).
508
Does exercise also boost the spirit? Many studies reveal that aerobic exercise can reduce stress, depression, and anxiety. Americans, Canadians, and Britons who do aerobic exercise at least three times a week manage stress better, exhibit more self-
But we could state this observation another way: Stressed and depressed people exercise less. These findings are correlations, and cause and effect are unclear. To sort out cause and effect, researchers experiment. They randomly assign stressed, depressed, or anxious people either to an aerobic exercise group or to a control group. Next, they measure whether aerobic exercise (compared with a control activity) produces a change in stress, depression, anxiety, or some other health-
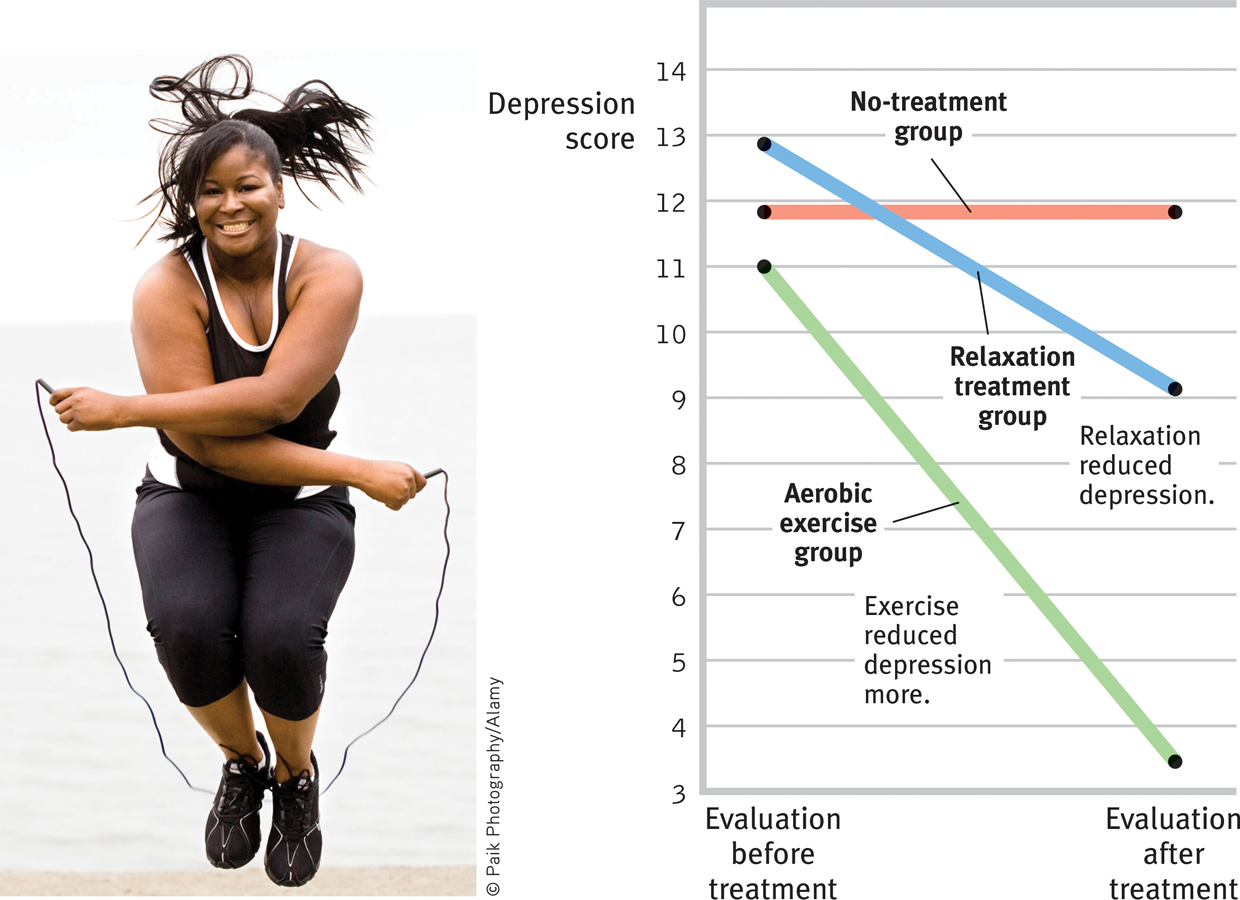
Aerobic exercise and depression Mildly depressed college women who participated in an aerobic exercise program showed markedly reduced depression, compared with those who did relaxation exercises or received no treatment. (Data from McCann & Holmes, 1984.)
Dozens of other experiments confirm that exercise prevents or reduces depression and anxiety (Conn, 2010; Rethorst et al., 2009; Windle et al., 2010). Moreover, exercise is not only as effective as drugs, it may better prevent symptom recurrence (Babyak et al., 2000; Salmon, 2001). When experimenters randomly assigned depressed people to an exercise group, an antidepressant group, or a placebo pill group, exercise diminished depression levels as effectively as antidepressants—
509

Vigorous exercise provides a substantial and immediate mood boost (Watson, 2000). Even a 10-
On a simpler level, the sense of accomplishment and improved physique and body image that often accompany a successful exercise routine may enhance one’s self-
Relaxation and Meditation
12-
Knowing the damaging effects of stress, could we learn to counteract our stress responses by altering our thinking and lifestyle? In the late 1960s, some respected psychologists began experimenting with biofeedback, a system of recording, amplifying, and feeding back information about subtle physiological responses, many controlled by the autonomic nervous system. Biofeedback instruments mirror the results of a person’s own efforts, enabling the person to learn which techniques do (or do not) control a particular physiological response. After a decade of study, however, the initial claims for biofeedback seemed overblown and oversold (Miller, 1985). In 1995, a National Institutes of Health panel declared that biofeedback works best on tension headaches.

Simple methods of relaxation, which require no expensive equipment, produce many of the results biofeedback once promised. Figure 12.30 pointed out that aerobic exercise reduces depression. But did you notice in that figure that depression also decreased among women in the relaxation treatment group? More than 60 studies have found that relaxation procedures can also help alleviate headaches, hypertension, anxiety, and insomnia (Nestoriuc et al., 2008; Stetter & Kupper, 2002).
Such findings would not surprise Meyer Friedman and his colleagues. They tested relaxation in a program designed to help Type A heart attack survivors (who are more prone to heart attacks than their Type B peers) reduce their risk of future attacks. They randomly assigned hundreds of middle-
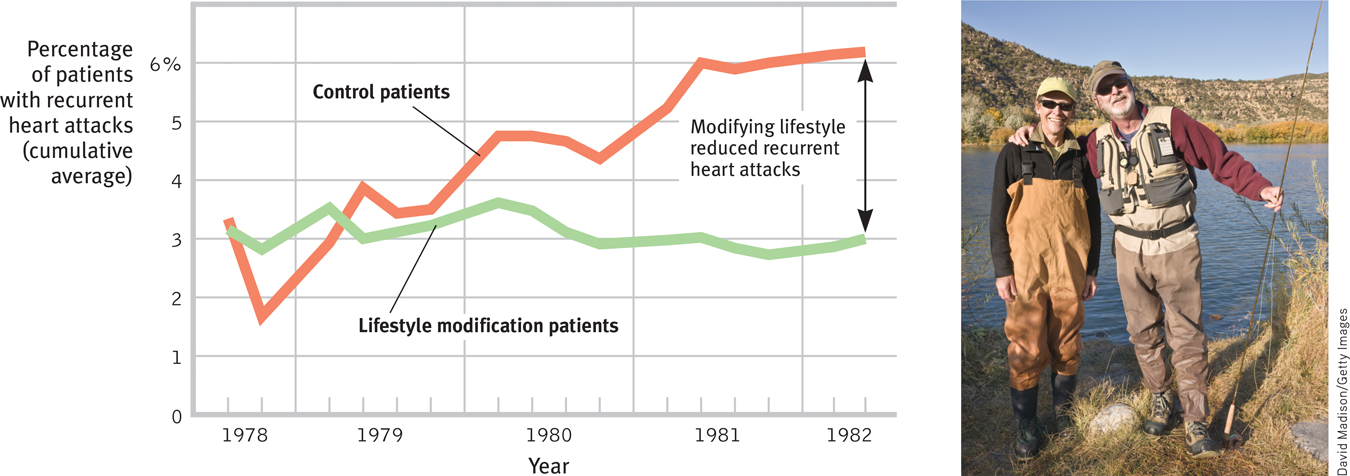
Recurrent heart attacks and lifestyle modification The San Francisco Recurrent Coronary Prevention Project offered counseling from a cardiologist to survivors of heart attacks. Those who were also guided in modifying their Type A lifestyle suffered fewer repeat heart attacks. (Data from Friedman & Ulmer, 1984.)
510
Time may heal all wounds, but relaxation can help speed that process. In one study, surgery patients were randomly assigned to two groups. Both groups received standard treatment, but the second group also experienced a 45-
Meditation is a modern practice with a long history. In many of the world’s great religions, meditation has been used to reduce suffering and improve awareness, insight, and compassion. Numerous studies have confirmed the psychological benefits of meditation (Goyal et al., 2014; Sedlmeier et al., 2012). Today, it has found a new home in stress management programs, such as mindfulness meditation. If you were taught this practice, you would relax and silently attend to your inner state, without judging it (Kabat-
“Sit down alone and in silence. Lower your head, shut your eyes, breathe out gently, and imagine yourself looking into your own heart.… As you breathe out, say ‘Lord Jesus Christ, have mercy on me.’ … Try to put all other thoughts aside. Be calm, be patient, and repeat the process very frequently.”
Gregory of Sinai, died 1346
Practicing mindfulness may improve many health measures. In one study of 1140 people, some received mindfulness-
511

So, what’s going on in the brain as we practice mindfulness? Correlational and experimental studies offer three explanations. Mindfulness
- strengthens connections among regions in our brain. The affected regions are those associated with focusing our attention, processing what we see and hear, and being reflective and aware (Ives-
Deliperi et al., 2011; Kilpatrick et al., 2011). - activates brain regions associated with more reflective awareness (Davidson et al., 2003; Way et al., 2010). When labeling emotions, “mindful people” show less activation in the amygdala, a brain region associated with fear, and more activation in the prefrontal cortex, which aids emotion regulation (Creswell et al., 2007).
- calms brain activation in emotional situations. This lower activation was clear in one study in which participants watched two movies—
one sad, one neutral. Those in the control group, who were not trained in mindfulness, showed strong differences in brain activation when watching the two movies. Those who had received mindfulness training showed little change in brain response to the two movies (Farb et al., 2010). Emotionally unpleasant images also trigger weaker electrical brain responses in mindful people than in their less mindful counterparts (Brown et al., 2013). A mindful brain is strong, reflective, and calm.
And then there are the mystics who seek to use the mind’s power to enable novocaine-
Exercise and meditation are not the only routes to healthy relaxation. Massage helps relax both premature infants and those suffering pain. An analysis of 17 experiments revealed another benefit: Massage therapy relaxes muscles and helps reduce depression (Hou et al., 2010).
Question
jaHXwS3fX6N2zRPRg4fG061jbwprawUoYQNhI21UCmRygFZ1bzyx5c/GzPilERY2F4KlBs+RkkDzNHro1KEMWOnnGVz+y9z9zo33MJFd1Em/J2gJW/M01UORmrUf0fXeaDh1v0H20uKJuAA7hfX44uteXxlCO2FwaHQwoyjMFx3ll93AQNcO0Om2zSn6385RBDQ6Fak4OWeYjobTtb9IGXZ4Dr65yR8UGlnzAQAAQ2LN/122ucO3AZa6YvaatS6K0qNE5HC6Ny06aMGed2DJxSzzGL7zVBAuG568s/PMUpOdaS4eMi7GziKD9nkviTmPElnRMEwl73BSTEgGDVcpzw==Faith Communities and Health
12-
A wealth of studies—
512
How should we interpret such findings? Correlations are not cause-
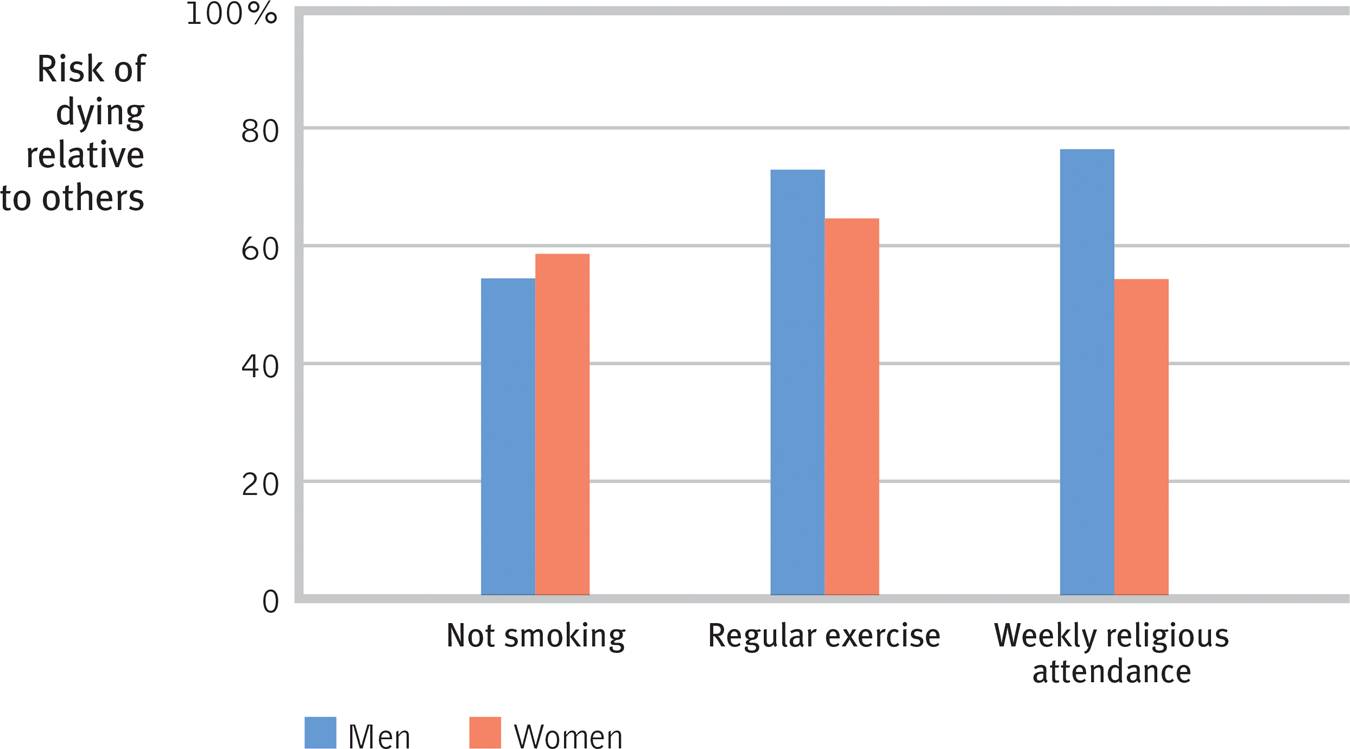
Predictors of longer life: Not smoking, frequent exercise, and regular religious attendance Epidemiologist William Strawbridge and his co-
These correlational findings do not indicate that nonattenders can suddenly add 8 years to their life if they start attending services and change nothing. Nevertheless, the findings do indicate that religious involvement, like nonsmoking and exercise, is a predictor of health and longevity. Can you imagine what intervening variables might account for the correlation? Research points to three possible sets of influences (FIGURE 12.33):
- Healthy behaviors: Religion promotes self-
control (McCullough & Willoughby, 2009), and religiously active people tend to smoke and drink much less and to have healthier lifestyles (Islam & Johnson, 2003; Koenig & Vaillant, 2009; Masters & Hooker, 2013; Park, 2007). In one Gallup survey of 550,000 Americans, 15 percent of the very religious were smokers, as were 28 percent of those nonreligious (Newport et al., 2010). But such lifestyle differences are not great enough to explain the dramatically reduced mortality in the Israeli religious settlements. In American studies, too, about 75 percent of the longevity difference remained when researchers controlled for unhealthy behaviors, such as inactivity and smoking (Musick et al., 1999). - Social support: Could social support explain the faith factor (Ai et al., 2007; Kim-
Yeary et al., 2012)? In Judaic, Christian, and Islamic religions, faith is a communal experience. To belong to one of these faith communities is to have access to a support network. Religiously active people are there for one another when misfortune strikes. Moreover, religion encourages marriage, another predictor of health and longevity. In the Israeli religious settlements, for example, divorce has been almost nonexistent. - Positive emotions: Even after controlling for social support, gender, unhealthy behaviors, preexisting health problems, and social support, the mortality studies have found that religiously engaged people tend to live longer (Chida et al., 2009). Researchers therefore speculate that religiously active people may benefit from a stable, coherent worldview, a sense of hope for the long-
term future, feelings of ultimate acceptance, and the relaxed meditation of prayer or Sabbath observance. These intervening variables may also help to explain why the religiously active have had healthier immune functioning, fewer hospital admissions, and, for AIDS patients, fewer stress hormones and longer survival (Ironson et al., 2002; Koenig & Larson, 1998; Lutgendorf et al., 2004).
Question
lbHv1GKeIKT8naNREVxmVtdSF/JtjRbZsgmAbLtgpRau5hfjFNc3+/BfWqQqs0hzjs7OXTTv1nIIciy0690vTJpA0Zolzd67nX/TDG+ws3Y1Miq3WQK8JpWsh5p1Rq+UVMcZ4AIAbkmCaUnseP10z1jiEWxqB2LQ4P3ynzDxQt9q1+7nHT4i9EugCX60qqAqLGFuOUi0rcqQRZVK8mxVYTZqWE4ZMDmuStF4S8xETFz3O5wA6cNblJz3tNTiZQwnVGDjJYRgQS/vXdYytfybMIbGEsdM9KhgOJmPPO1v/8G55jXkhk96uBLb/6QKHKZdqEOcRU1/XtgGnOoA6af3pX68RDmNUYOUZ9uqO2ERl8CdjpYm7BcV64EB4lg=513
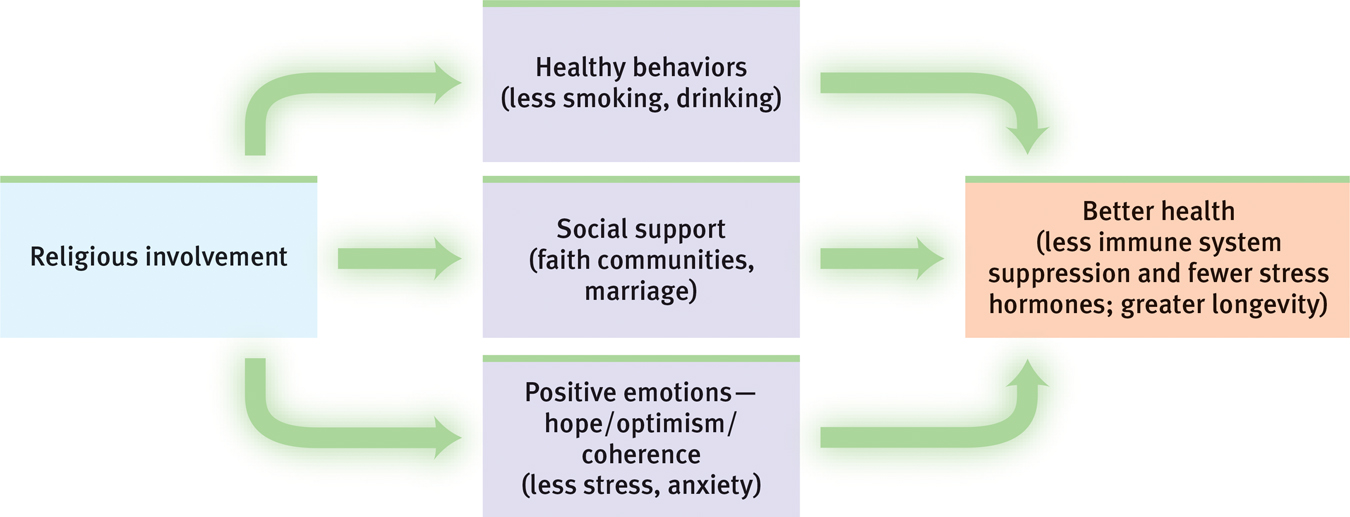
Possible explanations for the correlation between religious involvement and health/longevity
RETRIEVAL PRACTICE
- What are some of the tactics we can use to manage successfully the stress we cannot avoid?
Aerobic exercise, relaxation procedures, mindfulness meditation, and religious engagement