Aging and Memory
17-2 How does memory change with age?
Among the most intriguing developmental psychology questions is whether adult cognitive abilities, such as memory, intelligence, and creativity, parallel the gradually accelerating decline of physical abilities.
As we age, we remember some things well. Looking back in later life, adults asked to recall the one or two most important events over the last half-century tend to name events from their teens or twenties (Conway et al., 2005; Rubin et al., 1998). They also display this “reminiscence bump” when asked to name their all-time favorite music, movies, and athletes (Janssen et al., 2011). Whatever people experience around this time—World War II, the 9/11 terrorist attacks, the election of the first U.S. Black president—becomes pivotal (Pillemer, 1998; Schuman & Scott, 1989). In our teens and twenties are so many memorable “firsts”—first kiss, first job, first day at college or university, first meeting in-laws.
Early adulthood is indeed a peak time for some types of learning and remembering. In one test of recall, people watched video clips as 14 strangers said their names, using a common format: “Hi, I’m Larry” (Crook & West, 1990). Then those strangers reappeared and gave additional details. For example, they said, “I’m from Philadelphia,” providing more visual and voice cues for remembering the person’s name. As FIGURE 17.2 shows, after a second and third replay of the introductions, everyone remembered more names, but younger adults consistently surpassed older adults.
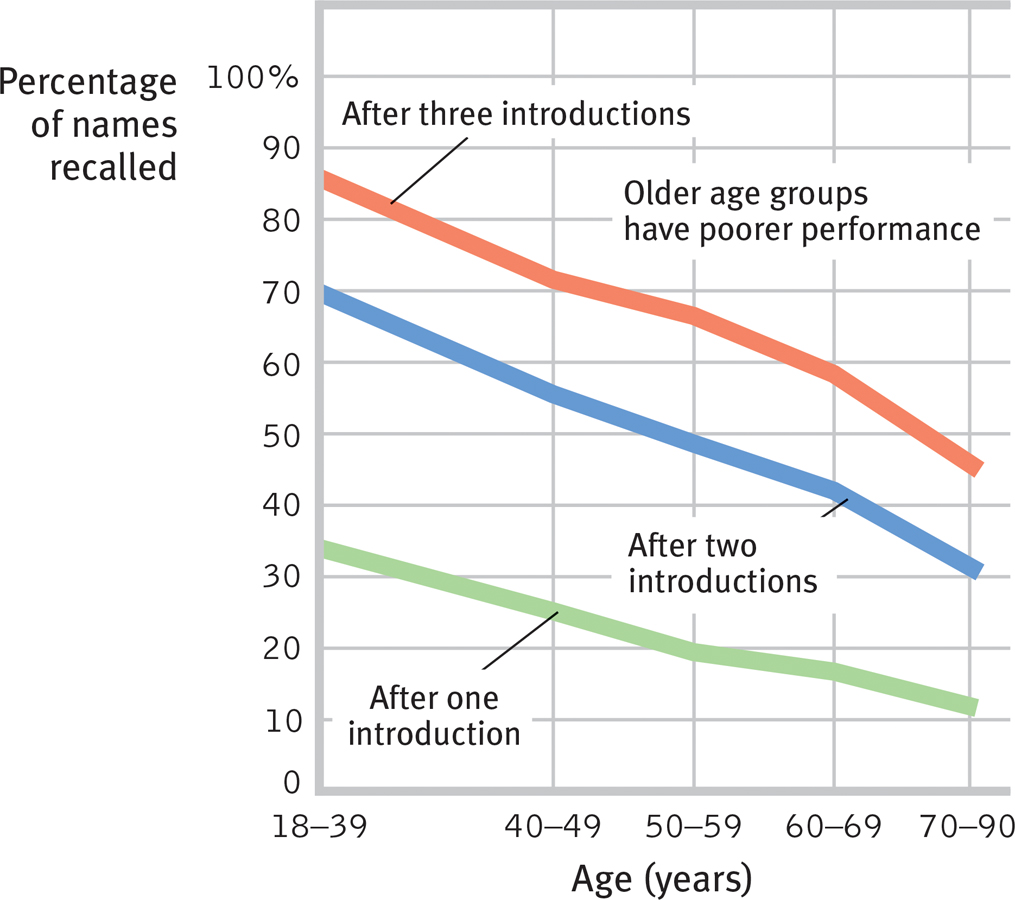
Tests of recall Recalling new names introduced once, twice, or three times is easier for younger adults than for older ones. (Data from Crook & West, 1990.)
Perhaps it is not surprising, then, that nearly two-thirds of people over age 40 have said their memory is worse than it was 10 years ago (KRC, 2001). In fact, how well older people remember depends on the task. In another experiment, when asked to recognize 24 words they had earlier tried to memorize, people showed only a minimal decline in memory. When asked to recall that information without clues, the decline was greater (FIGURE 17.3).
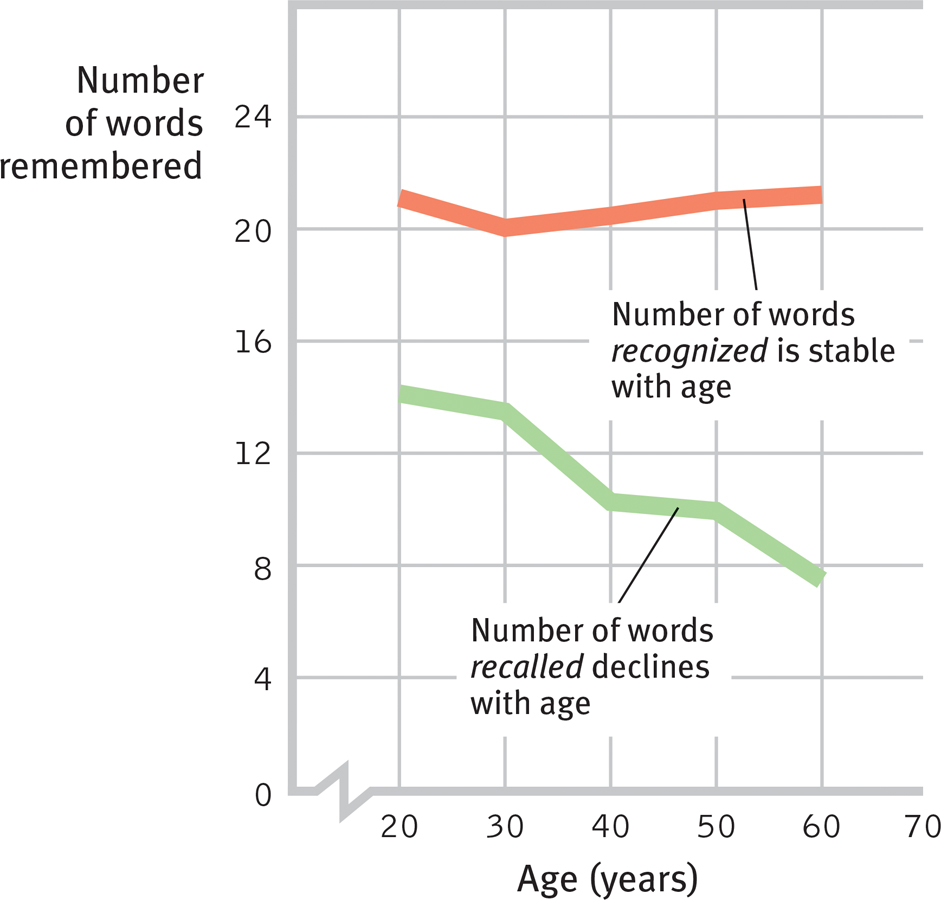
Recall and recognition in adulthood In this experiment, the ability to recall new information declined during early and middle adulthood, but the ability to recognize new information did not. (Data from Schonfield & Robertson, 1966.)
Teens and young adults surpass both young children and 70-year-olds at prospective memory (“Remember to …”) (Zimmerman & Meier, 2006). But older people’s prospective memory remains strong when events help trigger a memory (as when walking by a convenience store triggers “Pick up milk!”). Time-based tasks (“Client meeting at 3:00 P.M.”) and especially habitual tasks (“Take medications at 9:00 A.M., 2:00 P.M., and 6:00 P.M.”) can be challenging (Einstein et al., 1990, 1995, 1998). To minimize such problems, older adults rely more on time management and reminder cues, such as notes to themselves (Henry et al., 2004). This might have helped John Basinger, who, at age 76, was to be interviewed by a local paper regarding a psychology journal article on his late-life memorization of all 12 volumes of John Milton’s epic poem Paradise Lost (Seamon et al., 2010; Weir, 2010). He forgot a scheduled meeting with the reporter. When calling to apologize, he noted the irony of forgetting his interview about memory.
In our capacity to learn and remember, as in other areas of development, we differ. Younger adults vary in their abilities to learn and remember, but 70-year-olds vary much more. “Differences between the most and least able 70-year-olds become much greater than between the most and least able 50-year-olds,” reported Oxford researcher Patrick Rabbitt (2006). Some 70-year-olds perform below nearly all 20-year-olds; other 70-year-olds match or outdo the average 20-year-old.
No matter how quick or slow we are, remembering seems also to depend on the type of information we are trying to retrieve. If the information is meaningless—nonsense syllables or unimportant events—then the older we are, the more errors we are likely to make. If the information is meaningful, as was Paradise Lost for John Basinger, older people’s rich web of existing knowledge will help them to hold it. But they may take longer than younger adults to produce the words and things they know. Older adults also more often experience memories on the tip-of-the-tongue (Ossher et al., 2012). Quick-thinking game show winners have usually been young or middle-aged adults (Burke & Shafto, 2004).
Psychologists who study the aging mind have been debating whether “brain fitness” computer training programs can build mental muscles and stave off cognitive decline. Given what we know about the brain’s plasticity, can exercising our brains on a “cognitive treadmill”—with memory, visual tracking, and problem-solving exercises—avert losing our minds? “At every point in life, the brain’s natural plasticity gives us the ability to improve … function,” said one neuroscientist-entrepreneur (Merzenich, 2007). One five-year study of nearly 3000 people found that 10 one-hour cognitive training sessions, with follow-up booster sessions a year (and more later), led to improved cognitive scores on tests related to their training (Boron et al., 2007; Willis et al., 2006). Other studies with children and adults also found that brain training that exercises working memory can sharpen the mind (Anguera et al., 2013; Jonides et al., 2012).
Based on such findings, some computer game makers are marketing daily brain-exercise programs for older adults. But other researchers, after reviewing all the available studies, advise caution (Melby-Lervåg & Hulme, 2013; Redick et al., 2013; Salthouse, 2010; Shipstead et al., 2012a,b). The available evidence, they argue, suggests that brain training can produce short-term gains, but only on the trained tasks (Berkman et al., 2014; Harrison et al., 2013). A British study of 11,430 people, who either completed brain training activities over six weeks or a control task, confirmed the limited benefits. Although the training improved the practiced skills, it did not boost overall cognitive fitness (Owen et al., 2010).
If you are within five years of 20, what experiences from the past year will you likely never forget? (This is the time of your life you may best remember when you are 50.)
Other modules explore another dimension of cognitive development: intelligence. There we discuss how cross-sectional studies (comparing people of different ages) and longitudinal studies (restudying people over time) have identified mental abilities that do and do not change as people age. Age is less a predictor of memory and intelligence than is proximity to death. Tell me whether someone is 8 months or 8 years from a natural death and, regardless of age, you’ve given me a clue to that person’s mental ability. In the last three or four years of life and especially as death approaches, cognitive decline typically accelerates and negative feelings increase (Vogel et al., 2013; Wilson et al., 2007). Researchers call this near-death drop terminal decline (Backman & MacDonald, 2006).
Neurocognitive Disorders and Alzheimer’s Disease
17-3 How do neurocognitive disorders and Alzheimer’s disease affect cognitive ability?
Most people who live into their nineties do so with clear minds. Some, unfortunately, suffer a substantial loss of brain cells in a process that is not normal aging. A series of small strokes, a brain tumor, or alcohol use disorder can progressively damage the brain, causing that mental erosion we call a neurocognitive disorder (NCD, formerly called dementia). Heavy midlife smoking more than doubles later risk of the disorder (Rusanen et al., 2011). The feared brain ailment Alzheimer’s disease strikes 3 percent of the world’s population by age 75. Up to age 95, the incidence of mental disintegration doubles roughly every 5 years (FIGURE 17.4).
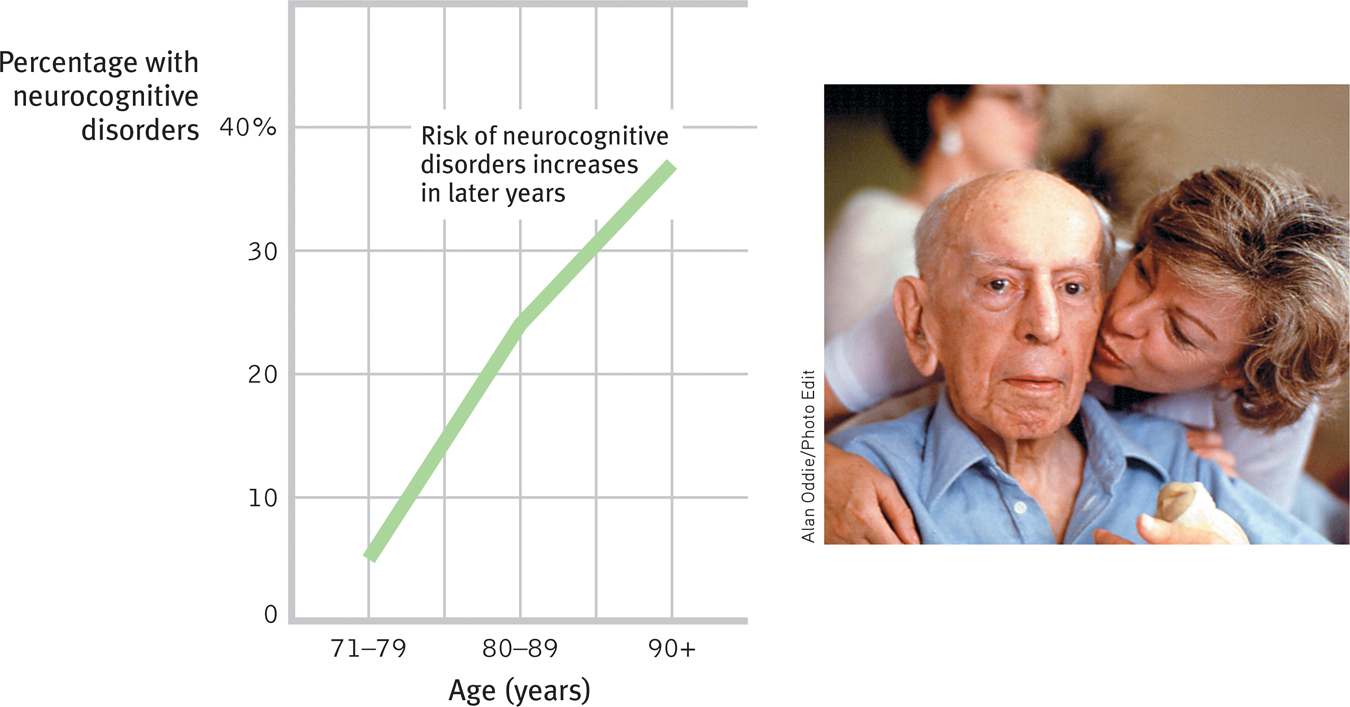
Incidence of neurocognitive disorders (NCDs) by age The risk of mental disintegration due to Alzheimer’s disease, strokes, or other brain disease increases with age (Brookmeyer et al., 2011). Still, most people who live into their nineties do so with clear minds.
Alzheimer’s destroys even the brightest of minds. First memory deteriorates, then reasoning. (Occasionally forgetting where you laid the car keys is no cause for alarm; forgetting how to get home may suggest Alzheimer’s.) Robert Sayre (1979) recalled his father shouting at his afflicted mother to “think harder,” while his mother, confused, embarrassed, on the verge of tears, randomly searched the house for lost objects. As the disease runs its course, after 5 to 20 years, the person becomes emotionally flat, then disoriented and disinhibited, then incontinent, and finally mentally vacant—a sort of living death, a mere body stripped of its humanity.
“We’re keeping people alive so they can live long enough to get Alzheimer’s disease.”
Steve McConnell, Alzheimer’s Association Vice President, 2007
Underlying the symptoms of Alzheimer’s are a loss of brain cells and a deterioration of neurons that produce the neurotransmitter acetylcholine, which is vital to memory and thinking. An autopsy reveals two telltale abnormalities in these acetylcholine-producing neurons: shriveled protein filaments in the cell body, and clumps of a free-floating protein fragment that accumulate as plaque at neuron tips where synaptic communication normally occurs. Long before its symptoms occur, new technologies can now test for the Alzheimer’s susceptibility gene or check spinal fluid for the culprit protein fragments (De Meyer et al., 2010; Luciano et al., 2009). Such discoveries have stimulated a race to invent and test drugs that may forestall the disease, such as by reducing the activity of a memory inhibiting neurotransmitter, called GABA (Chen et al., 2014). The recent discovery of 21 associated genes may help (Lambert et al., 2013).
A diminishing sense of smell and slowed or wobbly walking may foretell Alzheimer’s (Belluck, 2012; Wilson et al., 2007). Among older adults, hearing loss, and its associated social isolation, predicts risk of depression and accelerated mental decline (Li et al., 2014; Lin et al., 2011a,b, 2013). Compared with people with good hearing, those with hearing loss show declines in memory, attention, and learning about three years earlier. In people at risk for Alzheimer’s, brain scans (FIGURE 17.5) have also revealed—before symptoms appear—the degeneration of critical brain cells and diminished activity in Alzheimer’s-related brain areas (Apostolova et al., 2006; Johnson et al., 2006; Wu & Small, 2006). When people memorized words, scans also showed diffuse brain activity, as if more exertion was required to achieve the same performance (Bookheimer et al., 2000).
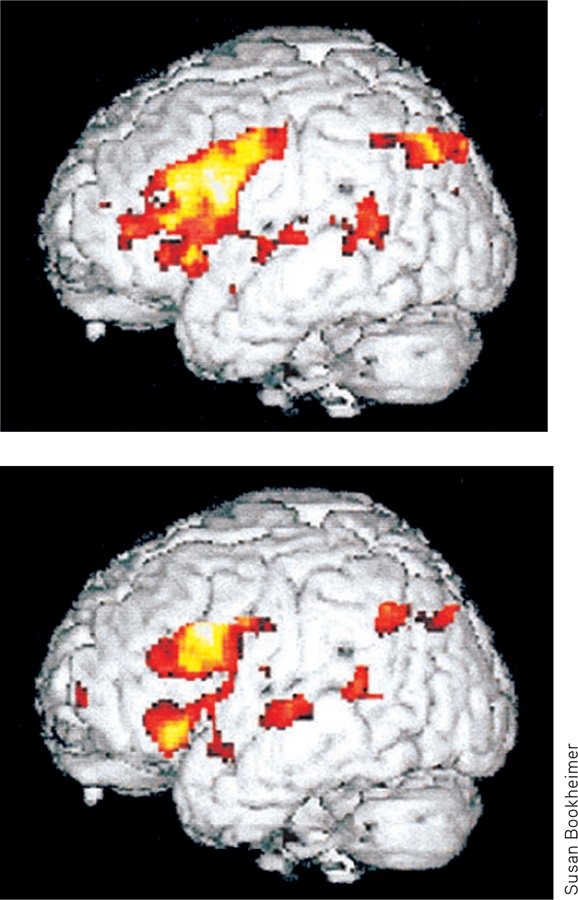
Predicting Alzheimer’s disease During a memory test, MRI scans of the brains of people at risk for Alzheimer’s (top) revealed more intense activity (yellow, followed by orange and red) when compared with normal brains (bottom). As brain scans and genetic tests make it possible to identify those likely to suffer Alzheimer’s, would you want to be tested? At what age?
Alzheimer’s is somewhat less common among those who exercise their minds as well as their bodies (Agrigoroaei & Lachman, 2011). As with muscles, so with the brain: Those who use it less often lose it.