55-2Are some psychotherapies more effective than others for specific disorders?
So what can we tell people considering psychotherapy, and those paying for it, about which psychotherapy will be most effective for their problem? The statistical summaries and surveys fail to pinpoint any one type of therapy as generally superior (Smith et al., 1977, 1980). Clients seemed equally satisfied, Consumer Reports concluded, whether treated by a psychiatrist, psychologist, or social worker; whether seen in a group or individual context; whether the therapist had extensive or relatively limited training and experience (Seligman, 1995). Other studies concur (Barth et al., 2013). There is little if any connection between clinicians’ experience, training, supervision, and licensing and their clients’ outcomes (Luborsky et al., 2002; Wampold, 2007).
“Whatever differences in treatment efficacy exist, they appear to be extremely small, at best.”
Bruce Wampold et al. (1997)
Page 676
So, was the dodo bird in Alice in Wonderland right: “Everyone has won and all must have prizes”? Not quite. Some forms of therapy get prizes for particular problems, though there is often an overlapping—or comorbidity—of disorders. Behavioral conditioning therapies, for example, have achieved especially favorable results with specific behavior problems, such as bed-wetting, phobias, compulsions, marital problems, and sexual dysfunctions (Baker et al., 2008; Hunsley & DiGiulio, 2002; Shadish & Baldwin, 2005). Psychodynamic therapy has helped treat depression and anxiety (Driessen et al., 2010; Leichsenring & Rabung, 2008; Shedler, 2010b). With mild to moderate depression, non-directive (client-centered) counseling often helps (Cuijpers et al., 2013). And new studies confirm cognitive and cognitive-behavioral therapy’s effectiveness (some say superiority) in coping with anxiety, posttraumatic stress disorder, and depression (Baker et al., 2008; De Los Reyes & Kazdin, 2009; Stewart & Chambless, 2009; Tolin, 2010).
“Different sores have different salves.”
English proverb
Moreover, we can say that therapy is most effective when the problem is clear-cut (Singer, 1981; Westen & Morrison, 2001). Those who experience phobias or panic, who are unassertive, or who are frustrated by sexual performance problems can hope for improvement. Those with less-focused problems, such as depression and anxiety, usually benefit in the short term but often relapse later. The more specific the problem, the greater the hope.
But no prizes—and little or no scientific support—go to certain other therapies (Arkowitz & Lilienfeld, 2006). We would all therefore be wise to avoid energy therapies that propose to manipulate people’s invisible energy fields, recovered-memory therapies that aim to unearth “repressed memories” of early child abuse, and rebirthing therapies that engage people in reenacting the supposed trauma of their birth.
As with some medical treatments, it’s possible for psychological treatments to be not only ineffective but also harmful—by making people worse or preventing their getting better (Barlow, 2010; Castonguay et al., 2010; Dimidjian & Hollon, 2010). The National Science and Technology Council cites the Scared Straight program (seeking to deter children and youth from crime) as an example of well-intentioned programs that have proved ineffective or even harmful.
The evaluation question—which therapies get prizes and which do not?—lies at the heart of what some call psychology’s civil war. To what extent should science guide both clinical practice and the willingness of health care providers and insurers to pay for psychotherapy?
On the one side are research psychologists using scientific methods to extend the list of well-defined and validated therapies for various disorders. They decry clinicians who “give more weight to their personal experiences” (Baker et al., 2008). On the other side are non-scientist therapists who view their practice as more art than science, saying that people are too complex and therapy too intuitive to describe in a manual or test in an experiment. Between these two factions stand the science-oriented clinicians, who aim to base practice on evidence and make mental health professionals accountable for effectiveness.
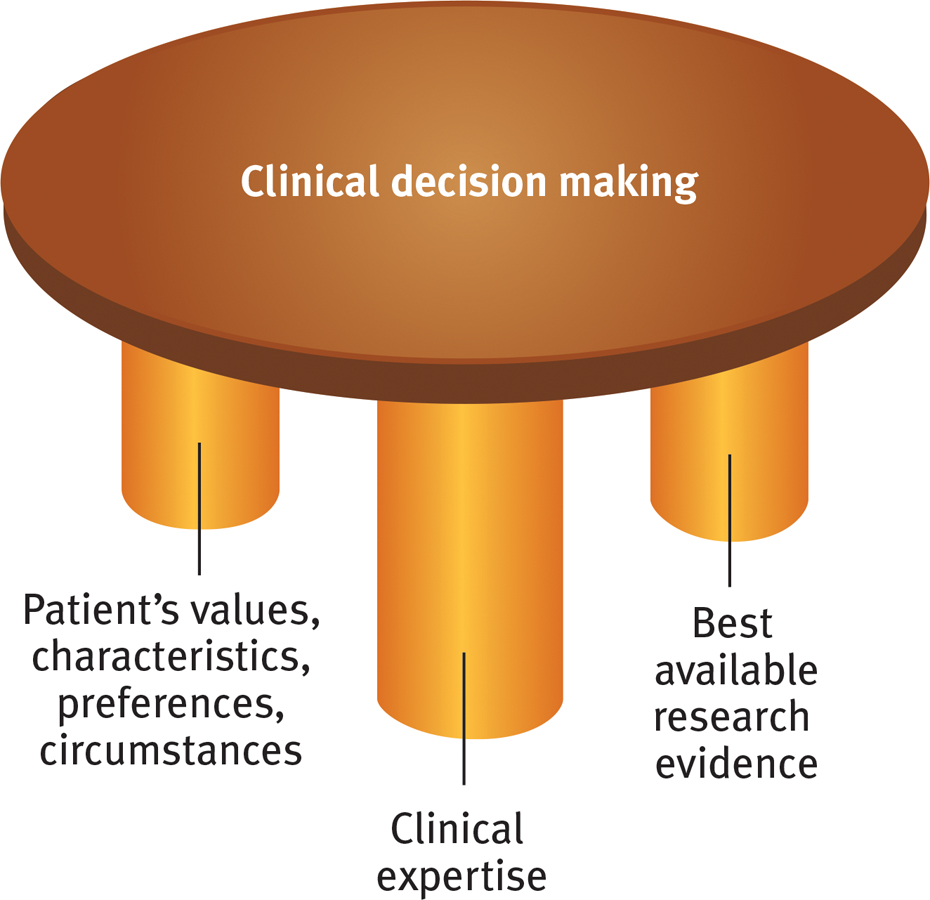
To encourage evidence-based practice in psychology, the American Psychological Association and others (2006; Lilienfeld et al., 2013) urge clinicians to integrate the best available research with clinical expertise and with patient preferences and characteristics. Available therapies “should be rigorously evaluated” and then applied by clinicians who are mindful of their skills and of each patient’s unique situation (FIGURE 55.2). Increasingly, insurer and government support for mental health services requires evidence-based practice.
Figure 55.2 Evidence-based clinical decision making The ideal clinical decision making is a three-legged stool, upheld by research evidence, clinical expertise, and knowledge of the patient.
RETRIEVAL PRACTICE
Therapy is most likely to be helpful for those with problems that _________ (are/are not) well-defined.