56-2How are brain stimulation and psychosurgery used in treating specific disorders?
Please continue to the next section.
Electroconvulsive Therapy
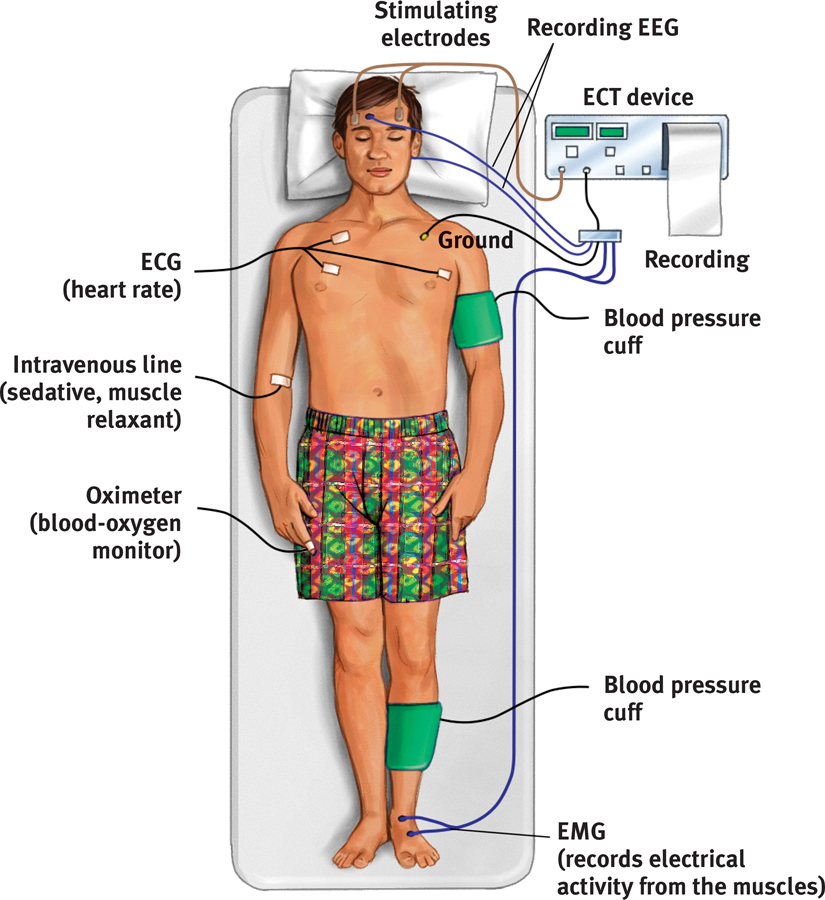
A more controversial brain manipulation occurs through shock treatment, or electroconvulsive therapy (ECT). When ECT was first introduced in 1938, the wide-awake patient was strapped to a table and jolted with roughly 100 volts of electricity to the brain, producing racking convulsions and brief unconsciousness. ECT therefore gained a barbaric image, one that lingers. Today’s ECT is much kinder and gentler. The patient receives a general anesthetic and a muscle relaxant (to prevent injury from convulsions) before a psychiatrist delivers 30 to 60 seconds of electrical current (FIGURE 56.2). Within 30 minutes, the patient awakens and remembers nothing of the treatment or of the preceding hours. After three such sessions each week for two to four weeks, 80 percent or more of people receiving ECT improve markedly, showing some memory loss for the treatment period but no discernible brain damage. Study after study confirms that ECT is an effective treatment for severe depression in “treatment-resistant” patients who have not responded to drug therapy (Bailine et al., 2010; Fink, 2009; Lima et al., 2013). An editorial in the Journal of the American Medical Association concluded that “the results of ECT in treating severe depression are among the most positive treatment effects in all of medicine” (Glass, 2001).
Figure 56.2 Electroconvulsive therapy Although controversial, ECT is often an effective treatment for depression that does not respond to drug therapy. (“Electroconvulsive” is no longer accurate, because patients are now given a drug that prevents bodily convulsions.)
Page 686
The medical use of electricity is an ancient practice. Physicians treated the Roman Emperor Claudius (10 B.C.E.–54 C.E.) for headaches by pressing electric eels to his temples.
How does ECT alleviate severe depression? After more than 70 years, no one knows for sure. One recipient likened ECT to the smallpox vaccine, which was saving lives before we knew how it worked. Others think of it as rebooting their cerebral computer. But what makes it therapeutic? Perhaps the shock-induced brain seizures calm neural centers where overactivity produces depression. Some research confirms that ECT works by weakening connections in a “hyper-connected” neural hub in the left frontal lobe (Perrin et al., 2012).
“I used to … be unable to shake the dread even when I was feeling good, because I knew the bad feelings would return. ECT has wiped away that foreboding. It has given me a sense of control, of hope.”
Kitty Dukakis (2006)
ECT is now administered with briefer pulses, sometimes only to the brain’s right side and with less memory disruption (HMHL, 2007). Yet no matter how impressive the results, the idea of electrically shocking people still strikes many as barbaric, especially given our ignorance about why ECT works. Moreover, about 4 in 10 ECT-treated patients relapse into depression within six months (Kellner et al., 2006). Nevertheless, in the minds of many psychiatrists and patients, ECT is a lesser evil than severe depression’s misery, anguish, and risk of suicide. As research psychologist Norman Endler (1982) reported after ECT alleviated his deep depression, “A miracle had happened in two weeks.”
Alternative Neurostimulation Therapies
Two other neural stimulation techniques—magnetic stimulation and deep-brain stimulation—also treat the depressed brain.
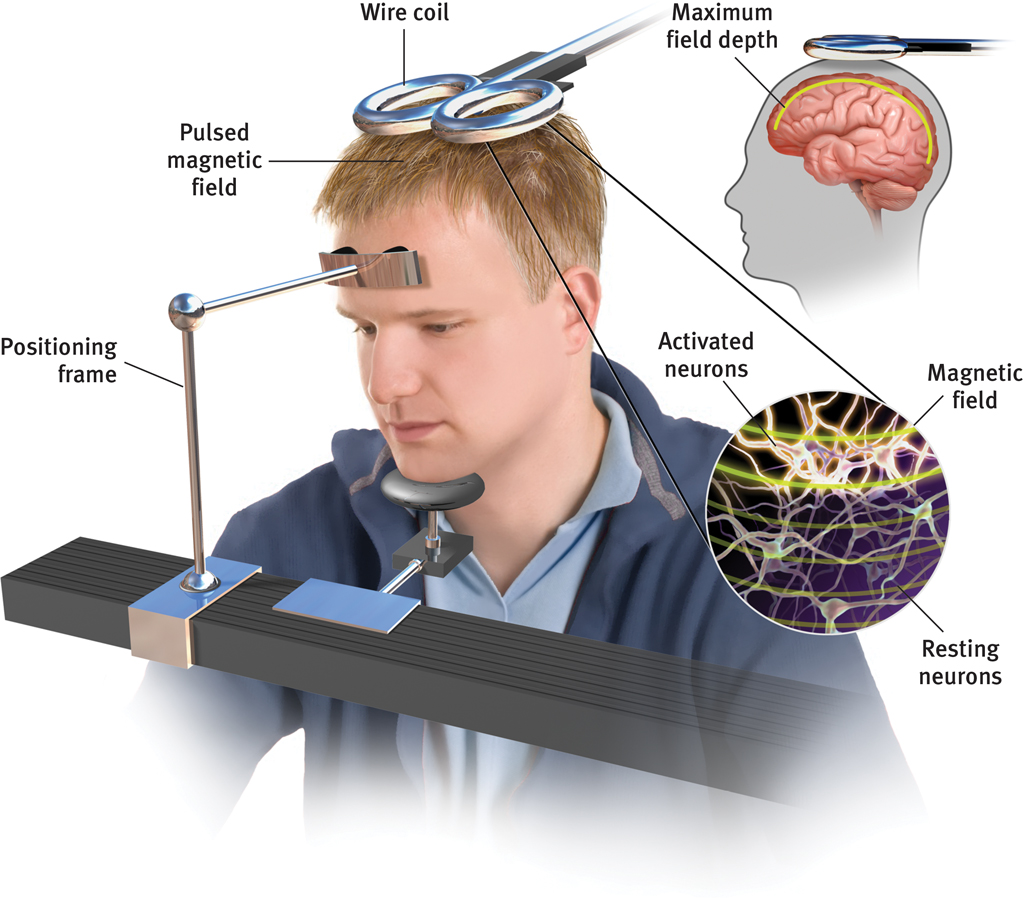
Magnetic StimulationDepressed moods sometimes improve when repeated pulses surge through a magnetic coil held close to a person’s skull (FIGURE 56.3). The painless procedure—called repetitive transcranial magnetic stimulation (rTMS)—is performed on wide-awake patients over several weeks. Unlike ECT, the rTMS procedure produces no brain seizures, memory loss, or other serious side effects aside from possible headaches.
Figure 56.3 Magnets for the mind Repetitive transcranial magnetic stimulation (rTMS) sends a painless magnetic field through the skull to the surface of the cortex. Pulses can be used to alter activity in various cortical areas.
A meta-analysis of 17 clinical experiments found that one other stimulation procedure alleviates depression: massage therapy (Hou et al., 2010).
Seven initial studies have found rTMS to be a “promising treatment,” with results comparable to antidepressants (Berlim et al., 2013). How it works is unclear. One possible explanation is that the stimulation energizes the brain’s left frontal lobe (Helmuth, 2001). Repeated stimulation may cause nerve cells to form new functioning circuits through the process of long-term potentiation.
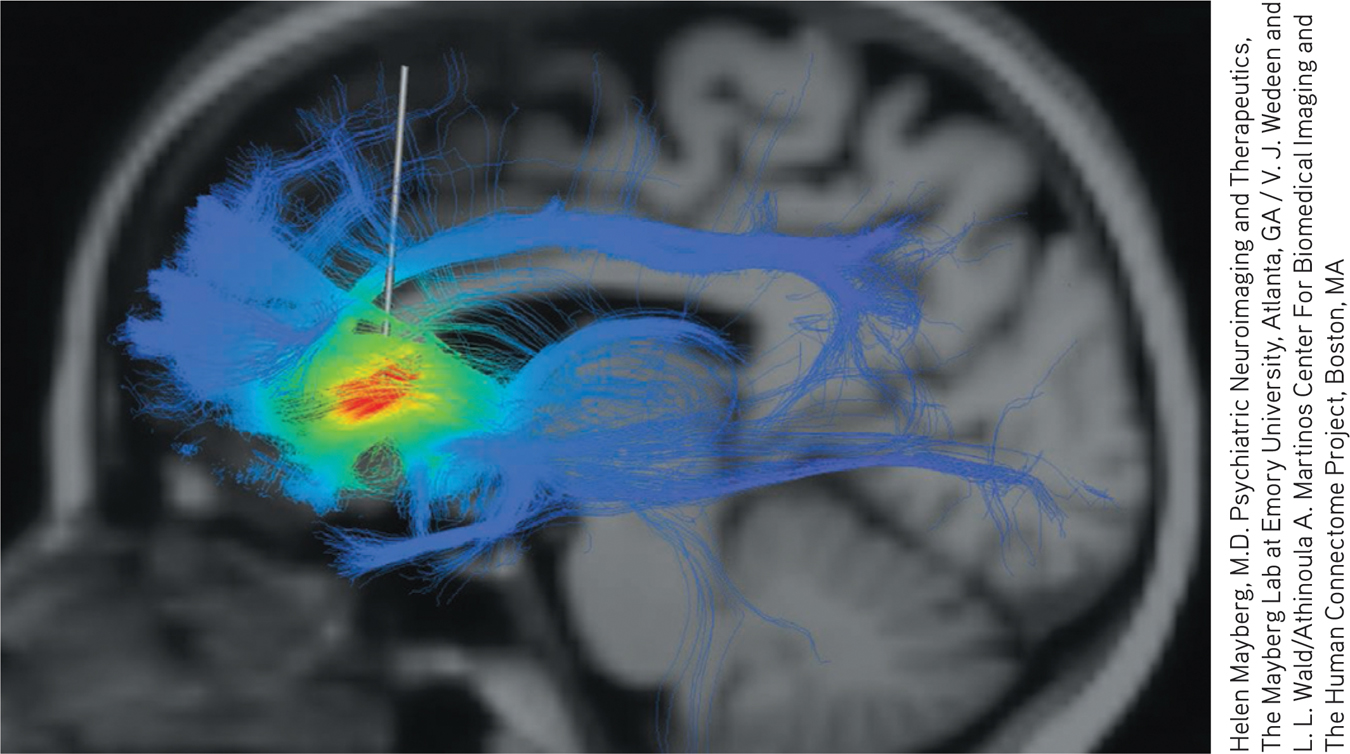
A depression switch? By comparing the brains of patients with and without depression, researcher Helen Mayberg identified a brain area (highlighted in red) that appears active in people who are depressed or sad, and whose activity may be calmed by deep-brain stimulation.
Deep-Brain StimulationOther patients whose depression has resisted both drugs that flood the body and ECT that jolts at least half the brain have benefited from an experimental treatment pinpointed at a brain depression center. Neuroscientist Helen Mayberg and her colleagues (2005, 2006, 2007, 2009) have been focusing on a neural hub that bridges the thinking frontal lobes to the limbic system. This area, which is overactive in the brain of a depressed or temporarily sad person, calms when treated by ECT or antidepressants. To experimentally excite neurons that inhibit this negative emotion-feeding activity, Mayberg drew upon the deep-brain stimulation technology sometimes used to treat Parkinson’s tremors. Since 2003, she and others have treated more than 100 depressed patients with deep brain stimulation to the neural “sadness center.” About one-third reportedly have responded “extremely well” and another 30 percent have modestly improved (Underwood, 2013). Some felt suddenly more aware and became more talkative and engaged; others improved only slightly if at all. Future research will explore whether Mayberg has discovered a switch that can lift depression. Other researchers are following up on reports that deep-brain stimulation can offer relief to people with obsessive-compulsive disorder and with drug and alcohol addictions (Corse et al., 2013; Luigjes et al., 2012; Rabins et al., 2009).
Page 687
RETRIEVAL PRACTICE
Severe depression that has not responded to other therapy may be treated with __________ __________ , which can cause brain seizures and memory loss. More moderate neural stimulation techniques designed to help alleviate depression include__________ __________ magnetic stimulation , and __________-__________ stimulation.