Other Disorders
Eating Disorders
13-21 What are the three major eating disorders?
 Our bodies are naturally disposed to maintain a steady weight, storing energy reserves in case food becomes unavailable. But psychological influences can overwhelm biological wisdom. Nowhere is this more painfully clear than in eating disorders.
Our bodies are naturally disposed to maintain a steady weight, storing energy reserves in case food becomes unavailable. But psychological influences can overwhelm biological wisdom. Nowhere is this more painfully clear than in eating disorders.
401

- In anorexia nervosa, people—usually female adolescents—starve themselves. Anorexia often begins as an attempt to lose weight, but the dieting doesn’t end. Even when far below normal weight, the self-starved person feels fat, fears being fat, and focuses obsessively on losing weight, sometimes exercising excessively. At some point in their lifetime, 0.6 percent of Americans meet the criteria for anorexia nervosa (Hudson et al., 2007). Many people with the disorder come from competitive, high-achieving families. They tend to have low self-esteem, to set impossible standards, and to fret about falling short of expectations (Polivy & Herman, 2002; Sherry & Hall, 2009).
- In bulimia nervosa, food binges alternate with vomiting, laxative use, fasting, and excessive exercise. Unlike anorexia, bulimia is marked by weight shifts within or above normal ranges, making this disorder easier to hide. Binge-purge eaters are preoccupied with food (especially sweet and high-fat foods) and obsessed with their weight and appearance. They experience bouts of guilt, depression, and anxiety, especially during and following binges (Hinz & Williamson, 1987; Johnson et al., 2002). About 1 percent of Americans, mostly women in their late teens or early twenties, have had bulimia.
- In binge-eating disorder, significant binge eating is followed by remorse. But people with the disorder do not purge, fast, or exercise excessively after their food binges, and so may be overweight. At some point during their lifetime, 2.8 percent of Americans have had binge-eating disorder (Hudson et al., 2007).
So, how can we explain eating disorders? Heredity matters. Identical twins share these disorders somewhat more often than fraternal twins do (Culbert et al., 2009; Klump et al., 2009).
But environment also matters. Body ideals vary across culture and time. In India, women students rate their ideal body size as close to their actual shape. In impoverished areas of the world, including much of Africa—where plump means prosperous and thinness can signal poverty or illness—bigger is better (Knick meyer, 2001; Swami et al., 2010).
Bigger does not seem better in Western cultures, where the rise in eating disorders over the last 50 years has coincided with a dramatic increase in women having a poor body image (Feingold & Mazzella, 1998). Part of the pressure on women stems from images of unnaturally thin models and celebrities (Tovee et al., 1997). Viewing such images, women—especially those who can’t resist comparing their bodies with others’—often feel ashamed, depressed, and dissatisfied with their own bodies (Myers & Crowther, 2009; Posavac et al., 1998; Stice & Shaw, 1994).
In one study, researchers tested media influences by giving some adolescent girls (but not others) a 15-month subscription to a teen fashion magazine (Stice et al., 2001). Vulnerable magazine readers (girls who felt dissatisfied, idealized thinness, and lacked social support) showed increased body dissatisfaction and eating disorder tendencies.
But there’s much more to body dissatisfaction and anorexia than media effects, note Christopher Ferguson and his colleagues (2011). Peer influences, such as teasing, also matter. So do wealth, increased marriage age, and, especially, competition for available mates. 
RETRIEVE + REMEMBER
Question 13.15
People with _______ (anorexia nervosa/bulimia nervosa) continue to want to lose weight even when they are underweight. Those with _______ (anorexia nervosa/bulimia nervosa) tend to have weight that fluctuates within or above normal ranges.
anorexia nervosa; bulimia nervosa
Dissociative Disorders
13-22 What are dissociative disorders, and why are they controversial?
Among the most bewildering disorders are the rare dissociative disorders. The person’s conscious awareness is said to become separated—dissociated—from painful memories, thoughts, and feelings. In this state, people may suddenly lose their memory or change their identity, often in response to an overwhelmingly stressful situation.
402

Dissociation itself is not so rare. Now and then, any one of us may have a fleeting sense of being unreal, of being separated from our body, of watching ourselves as if in a movie. But a massive dissociation of self from ordinary consciousness occurs in dissociative identity disorder (DID). At different times, two or more distinct identities seem to control the person’s behavior, each with its own voice and mannerisms. Thus, the person may be prim and proper one moment, loud and flirtatious the next. Typically, the original personality denies any awareness of the other(s).
Skeptics question the genuineness of DID. First, they find it suspicious that DID has such a short history. Between 1930 and 1960, the number of DID diagnoses in North America was 2 per decade. By the 1980s, when the DSM contained the first formal code for this disorder, the number of reported cases had exploded to more than 20,000 (McHugh, 1995a). The average number of displayed personalities also mushroomed—from 3 to 12 per patient (Goff & Simms, 1993).
Second, note the skeptics, DID is much less common outside North America, although in other cultures some people are said to be “possessed” by an alien spirit (Aldridge-Morris, 1989; Kluft, 1991). In Britain, DID—which some consider “a wacky American fad” (Cohen, 1995)—is rare. In India and Japan, it is essentially nonexistent. Such findings, say skeptics, point to a cultural explanation. They propose that this disorder is created by therapists in a particular social context (Merskey, 1992). Rather than being provoked by trauma, dissociative symptoms tend to be exhibited by suggestible, fantasy-prone people (Giesbrecht et al., 2008, 2010).
Third, instead of being a real disorder, some ask, could DID be an extension of the way we vary the “selves” we present, as when we display a goofy, loud self while hanging out with friends, and a subdued, respectful self around grandparents? If so, say the critics, clinicians who discover multiple personalities may merely have triggered role playing by fantasy-prone people. After all, patients do not enter therapy saying, “Allow me to introduce myselves.” Rather, note these skeptics, some therapists go fishing for multiple personalities: “Have you ever felt like another part of you does things you can’t control? Does this part of you have a name? Can I talk to the angry part of you?” Once patients permit a therapist to talk, by name, “to the part of you that says those angry things,” they begin acting out the fantasy. Like actors who lose themselves in their roles, vulnerable patients may “become” the parts they are acting out. The result may be the experience of another self.
Other researchers and clinicians believe DID is a real disorder. They find support for this view in the distinct brain and body states associated with differing personalities (Putnam, 1991). DID patients have exhibited activity in brain areas linked with traumatic memories (Elzinga et al., 2007).
If DID is a real disorder, how can we best understand it? Both the psychodynamic and the learning perspectives interpret DID symptoms as ways of dealing with anxiety. Psychoanalysts see them as defenses against the anxiety caused by unacceptable impulses. In this view, an immoral second personality allows the discharge of forbidden impulses. Learning theorists see dissociative disorders as behaviors reinforced by anxiety reduction.
Other psychologists include dissociative disorders under the umbrella of posttraumatic stress disorder. In this view, DID would be a natural, protective response to traumatic experiences during childhood (Dalenberg et al., 2012). Many DID patients recall suffering physical, sexual, or emotional abuse as children (Gleaves, 1996; Lilienfeld et al., 1999). In one study of 12 murderers diagnosed with DID, 11 had suffered severe abuse, even torture, in childhood (Lewis et al., 1997). One had been set afire by his parents. Another had been used in child pornography and was scarred from being made to sit on a stove burner. Some critics wonder, however, whether vivid imagination or therapist suggestion contributes to such recollections (Kihlstrom, 2005). Disrupted sleep may also contribute, with intrusions of dreamlike experiences into waking consciousness (Lynn et al., 2012).
403
So the debate continues. On one side are those who believe multiple personalities are the desperate efforts of people trying to detach from a horrific existence. On the other are the skeptics who think DID is a condition constructed out of the therapist-patient interaction and acted out by fantasy-prone, emotionally vulnerable people.
RETRIEVE + REMEMBER
Question 13.16
The proponents of psychodynamic and learning perspectives agree that dissociative identity disorder symptoms are ways of dealing with anxiety. How do their explanations differ?
The psychodynamic explanation of DID symptoms is that they are defenses against anxiety generated by unacceptable urges. The learning perspective attempts to explain these symptoms as behaviors that have been reinforced by relieving anxiety in the past.
Personality Disorders
13-23 What characteristics are typical of personality disorders in general, and what biological and psychological factors are associated with antisocial personality disorder?
There is little debate about the reality of personality disorders. These disruptive, inflexible, and enduring behavior patterns interfere with a person’s social functioning. Some people with these disorders withdraw and avoid social contact. Some interact but do so without responding emotionally. Others show insecurity and instability as they manipulate others or pull them close, then push them away.
The most troubling and heavily researched personality disorder is antisocial personality disorder. A person with this disorder is typically a male who shows no conscience in his actions, even toward friends and family. When an antisocial personality combines a keen intelligence with no conscience, the result may be a charming and clever con artist—or even a fearless, focused, ruthless soldier, CEO, or politician (Dutton, 2012).
Lack of conscience usually becomes plain before age 15, as the person begins to lie, steal, fight, or display unrestrained sexual behavior (Cale & Lilienfeld, 2002). Not all such children become antisocial adults. Those who do (about half of them) will generally be unable to keep a job, irresponsible as a spouse and parent, and violent or otherwise criminal (Farrington, 1991). People with antisocial personality disorder behave impulsively and then feel and fear little (Fowles & Dindo, 2009). Antisocial does not mean criminal (Skeem & Cooke, 2010). But do all criminals have antisocial personality disorder? Definitely not. Most criminals show concern for their friends and family members.
Antisocial personality disorder is woven of both biological and psychological strands. No single gene codes for a complex behavior such as crime. There is, however, a genetic tendency toward a fearless and uninhibited life. Twin and adoption studies reveal that biological relatives of people with antisocial and unemotional tendencies are at increased risk for antisocial behavior (Frisell et al., 2012; Tuvblad et al., 2011).
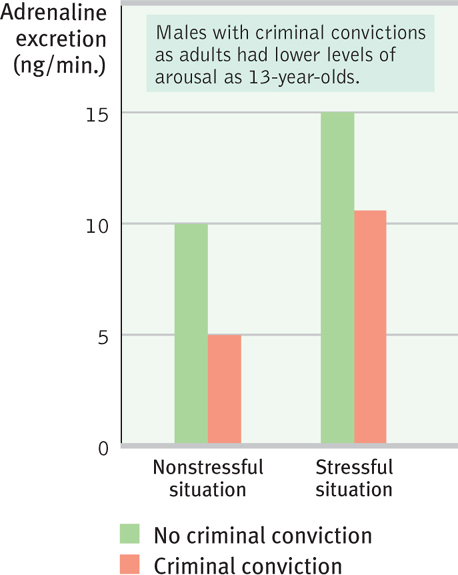
The genetic vulnerability of those with antisocial personality disorder appears as low arousal. Awaiting events that most people would find unnerving, such as electric shocks or loud noises, they show little bodily arousal (Hare, 1975; van Goozen et al., 2007). Long-term studies have shown that their levels of stress hormones were lower than average when they were youngsters, before committing any crime (FIGURE 13.14). Even at age 3, children who were slow to develop conditioned fears were later more likely to commit a crime (Gao et al., 2010).
404
With antisocial behavior, as with so much else, nature and nurture interact to leave their marks on the brain. To explore the neural basis of antisocial personality disorder, scientists are identifying brain activity differences in antisocial criminals. Shown emotionally evocative photographs, such as a man holding a knife to a woman’s throat, they display lower than normal heart rate and perspiration responses, and less activity in brain areas that typically respond to emotional stimuli (Harenski et al., 2010; Kiehl & Buckholtz, 2010). They also display a hyper-reactive dopamine reward system that predisposes their impulsive drive to do something rewarding, despite the consequences (Buckholtz et al., 2010). One study compared PET scans of 41 murderers’ brains with those from people of similar age and sex. The murderers’ frontal lobes, an area that helps control impulses, displayed reduced activity (Raine, 1999, 2005). This reduction was especially apparent in those who murdered impulsively. In a follow-up study, researchers found that violent repeat offenders had 11 percent less frontal lobe tissue than normal (Raine et al., 2000). This helps explain another finding: People with antisocial personality disorder fall far below normal in aspects of thinking such as planning, organization, and inhibition, which are all frontal lobe functions (Morgan & Lilienfeld, 2000). Such data remind us: Everything psychological is also biological.
The findings described in this chapter make clear the need for research and treatment to help the growing number of people, especially teenagers and young adults, who suffer the bewilderment and pain of a psychological disorder. Although mindful of their pain, we can also be encouraged by the many successful people who pursued brilliant careers while enduring psychological difficulties. Eighteen of them were U.S. presidents, according to one psychiatric analysis of their biographies (Davidson et al., 2006). The bewilderment, fear, and sorrow caused by psychological disorders are real. But, as Chapter 14 shows, hope, too, is real.