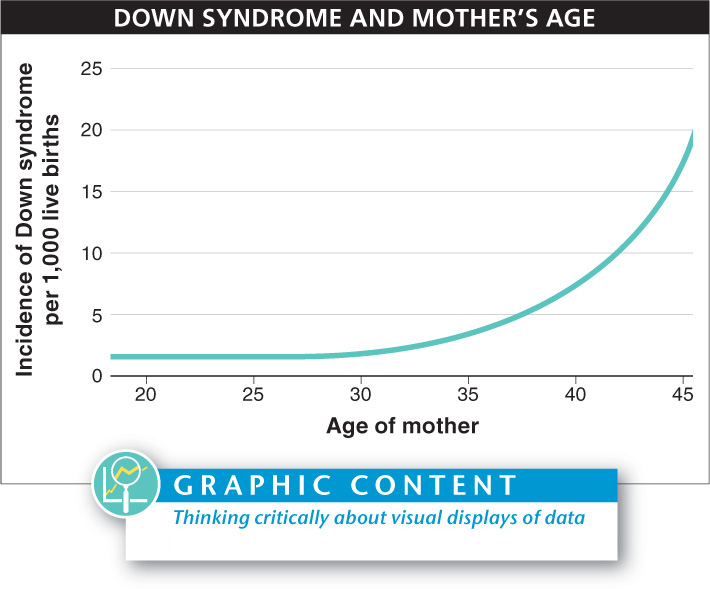
Reproduction becomes riskier for women as they become older. Increasingly, their gametes contain incorrect numbers of chromosomes or chromosomes that have been damaged (FIGURE 6-34). These problems can lead to effects on the offspring that range from minor to fatal.
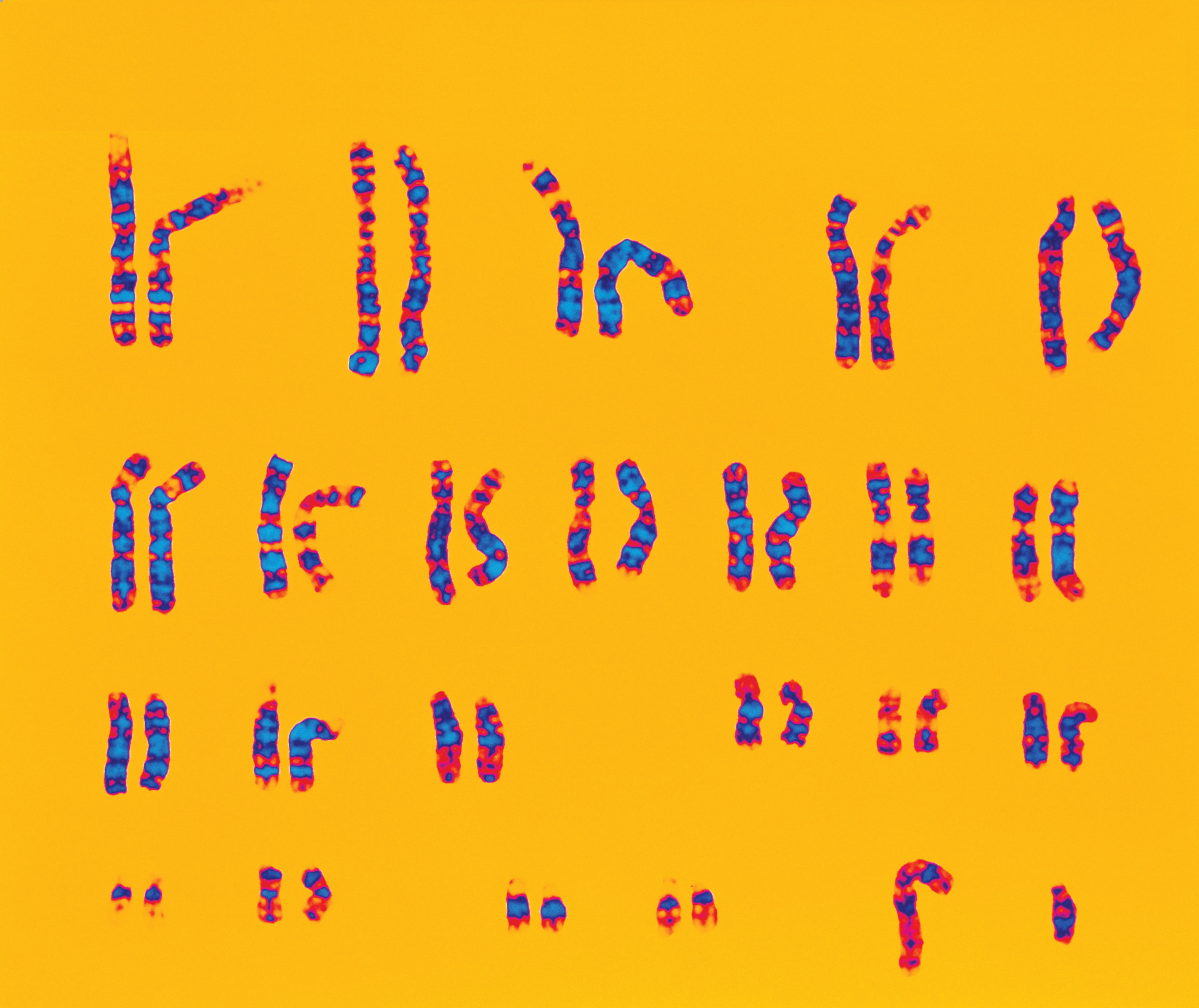
To find out whether their offspring may have a disorder associated with incorrect numbers of chromosomes, parents can request a quick test for some common genetic problems even before their baby is born. This information is available from an analysis of an individual’s karyotype, a visual display of the complete set of chromosomes. A karyotype can be made for adults or children, but it is most commonly done for a fetus. A karyotype is a useful diagnostic tool because it can be prepared very early in the fetus’s development to assess whether it has an abnormality in the number of chromosomes or in their structure. And because the test shows all of the chromosomes, even the sex chromosomes, it also reveals the sex of the fetus.
Preparing a karyotype takes five steps. (1) Some cells must be obtained from the individual. (2) The cells are then encouraged to divide by culturing them in a test tube with nutrients. (3) After a few days to two weeks of cell division, the cells are treated with a chemical that stops them exactly midway through cell division—
The first step—
1. Amniocentesis. This procedure can be done approximately three to four months into a pregnancy (FIGURE 6-36). In one quick motion (and without the use of anesthetic), a 3-
36

2. Chorionic villus sampling (CVS). In this procedure, rather than sampling cells from the amniotic fluid, a small bit of tissue is removed from the placenta, the temporary organ that allows the transfer of gases, nutrients, and waste products between a mother and fetus. A needle is inserted either through the abdomen or through the vagina and cervix, again using ultrasound for guidance. Then a small piece of the finger-
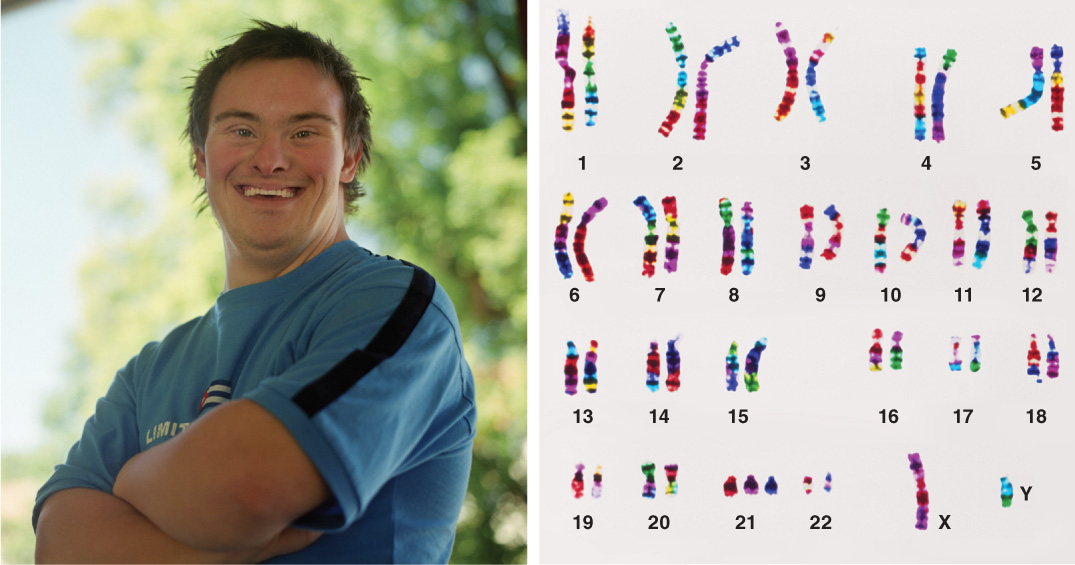
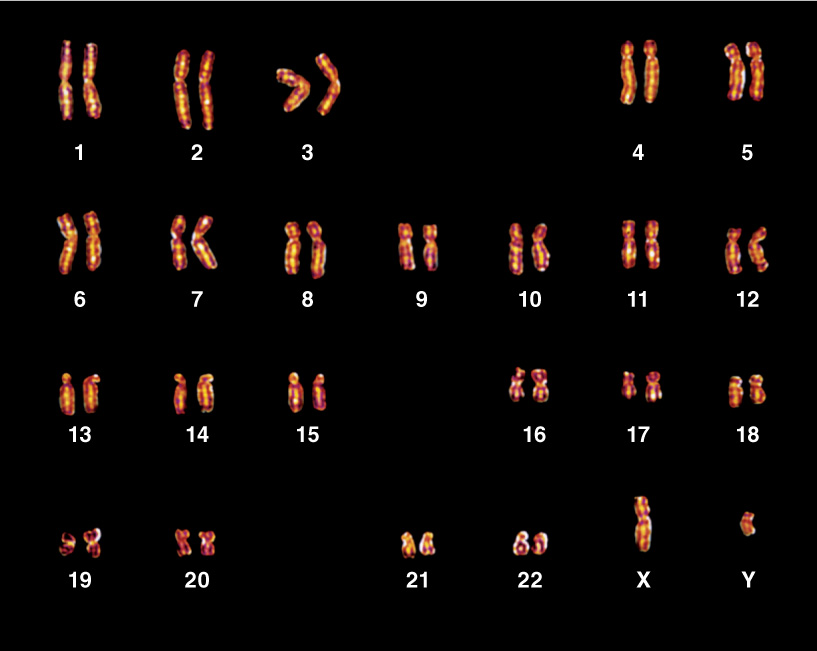
The resulting karyotype, whether from amniocentesis or CVS, will reveal whether the fetus carries an extra copy of any of the chromosomes or lacks a copy of one or more chromosomes. Of all the chromosomal disorders detected by karyotyping, Down syndrome is the most commonly observed. Named after John Langdon Down, the doctor who first described it, in 1866, the syndrome is revealed by the presence of an extra copy of chromosome 21 (FIGURE 6-37). (For this reason, the condition that causes Down syndrome is also called “trisomy 21.”) Striking about 1 in every 1,000 children born, Down syndrome is characterized by a suite of physical and mental characteristics that includes learning disabilities, a flat facial profile, heart defects, and increased susceptibility to respiratory difficulties.
37
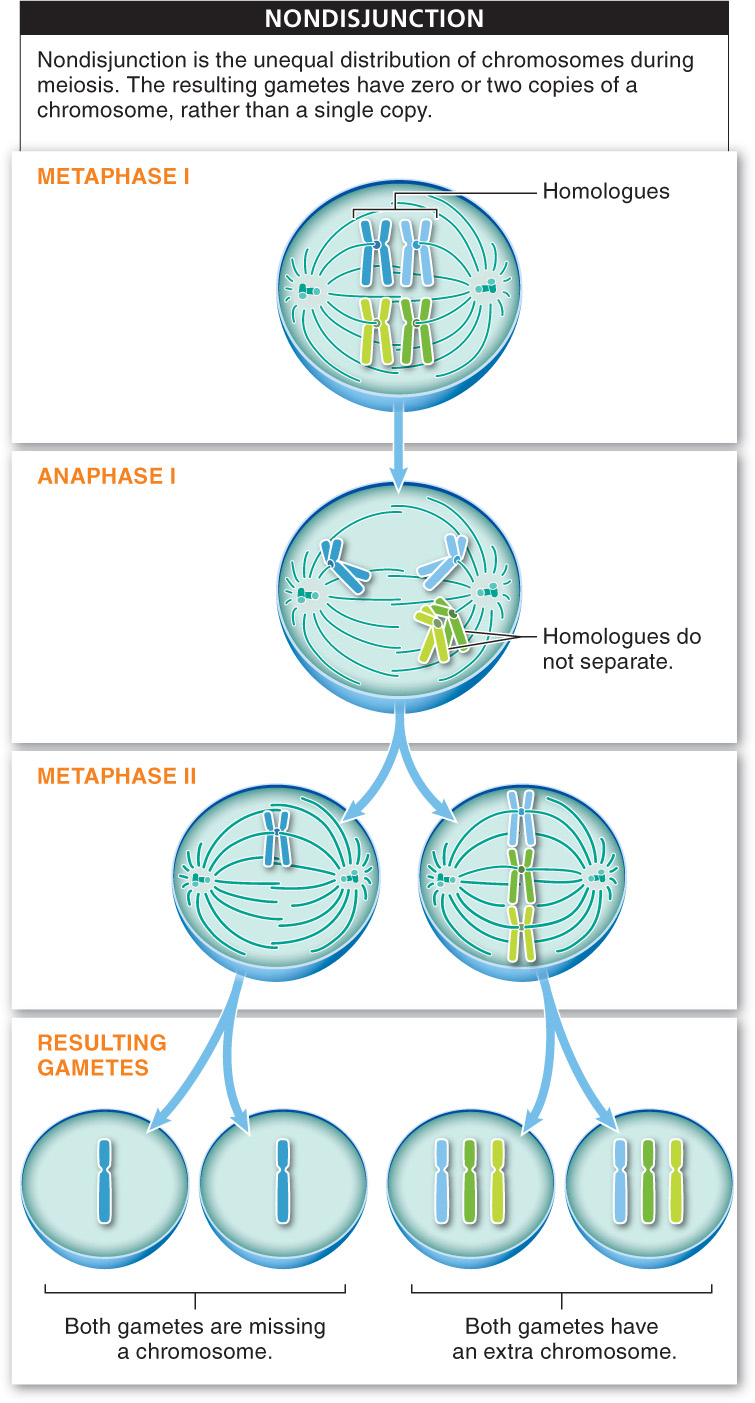
Down syndrome and other disorders caused by a missing chromosome or an extra copy of a chromosome are a consequence of nondisjunction, the unequal distribution of chromosomes during meiosis. Nondisjunction can occur at two different points in meiosis: homologues can fail to separate during meiosis I, or sister chromatids can fail to separate during meiosis II (FIGURE 6-38). In both cases, nondisjunction results in an egg or sperm with zero or two copies of a chromosome rather than a single copy. Any of the chromosomes can fail to separate during cell division, but the ramifications of trisomy (having an extra copy of one chromosome in every cell) are greater for chromosomes with larger numbers of genes.
When trisomy occurs for chromosomes with greater numbers of genes, the likelihood that the developing embryo will survive to birth is reduced. Consequently, we tend to see cases of trisomy that involve only the chromosomes with the fewest genes, such as chromosomes 13, 15, 18, 21, and 22. In fact, observations show that trisomy 1 is never seen (all such fertilized eggs die before implantation in the uterus), trisomy 13 occurs in 1 in 20,000 newborns (and most die soon after birth), while trisomy 21, as we’ve seen, occurs in 1 in 1,000 newborns (many of whom live long lives).
Why do older women have more babies with Down syndrome?
As we mentioned at the beginning of this section, as women become older there are increased problems associated with reproduction. Older women, for example, have more babies with Down syndrome. Why does the risk of having a baby with Down syndrome or some other disorder that results from trisomy increase with increasing age for women, but significantly less so for men? As women age, their gametes tend to have more errors. The reason is that those eggs began meiosis near the time the woman was born, and they may not complete it until she is 40 or more years old. During those decades, the cells may develop problems—
Whereas lacking a non-
TAKE-HOME MESSAGE 6.17
A karyotype is a visual display of a complete set of chromosomes. It is a useful diagnostic tool because it can be prepared early in fetal development to assess whether there is an abnormality in the number of chromosomes or in their structure, such as in Down syndrome. Down syndrome is caused by having an extra copy of chromosome 21.
What is nondisjunction and which are the two steps in meiosis during which it can occur?
Nondisjunction is the unequal distribution of chromosomes during meiosis, and can occur at two different points; homologous chromosomes can fail to separate during anaphase I, or sister chromatids can fail to separate during anaphase II. In either case, some or all of the gametes produced will have an inappropriate number of chromosomes.
38