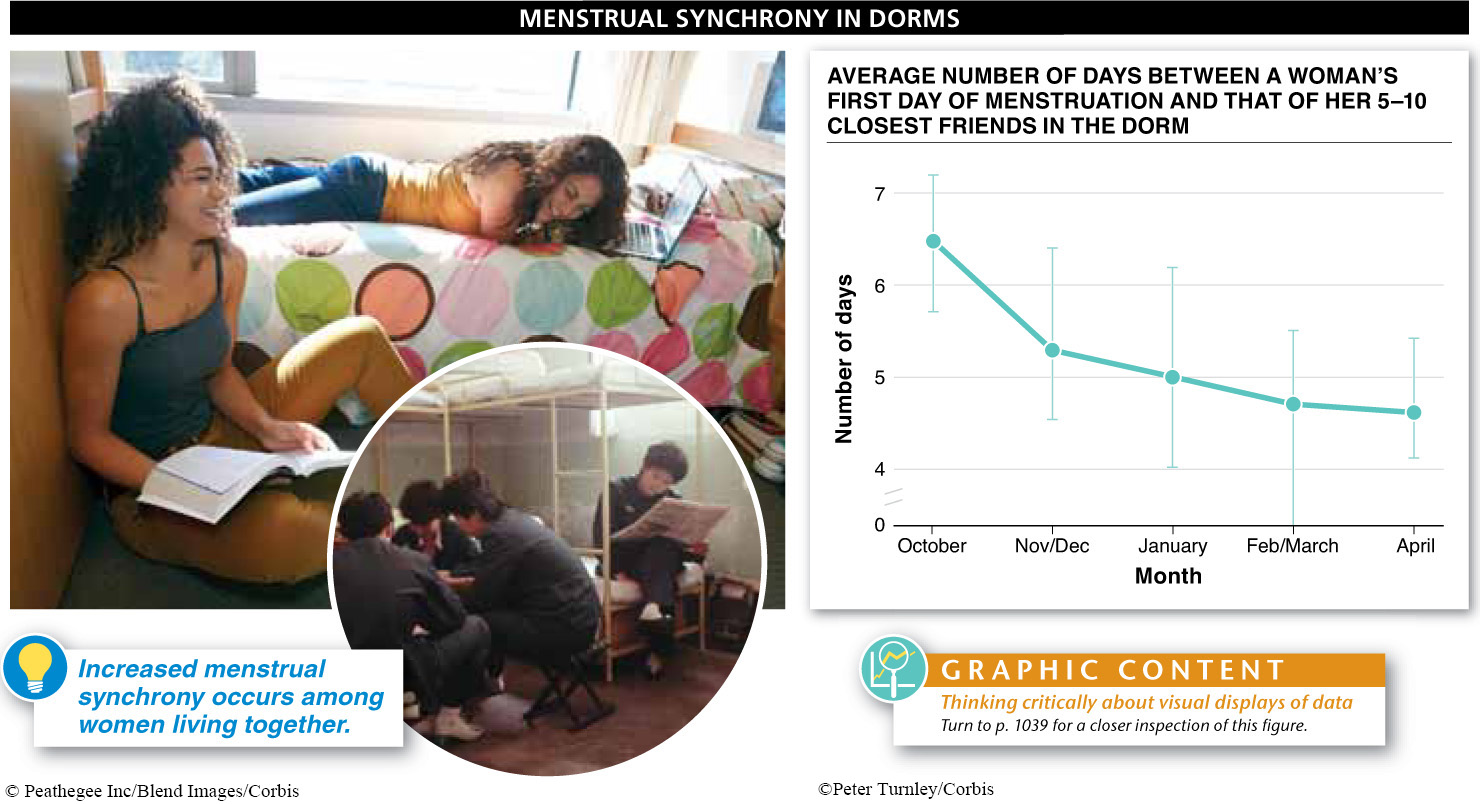
If you are female, here’s something you may have noticed if you are living in a dormitory (or a prison): when women live in close proximity, their reproductive cycles become synchronized over time so that they menstruate and—
1019
It’s not clear why such synchrony of reproductive cycles would occur, however. And other researchers have been critical of the original data analyses and have argued that the different lengths of women’s cycles make it impossible for them to become truly synchronized. Results from recent studies have been conflicting; several have found evidence for menstrual synchrony, but others have not. The jury is still out on this hotly contested issue.
Hormones regulate the timing and development of egg production, called the ovarian cycle, which occurs approximately every 28 days. Hormones also regulate the menstrual cycle, during which the uterus prepares for the possible implantation and nurturing of a fertilized egg, and sheds its lining when fertilization does not occur. We describe each of these cycles and how each influences the other (FIGURE 25-17).
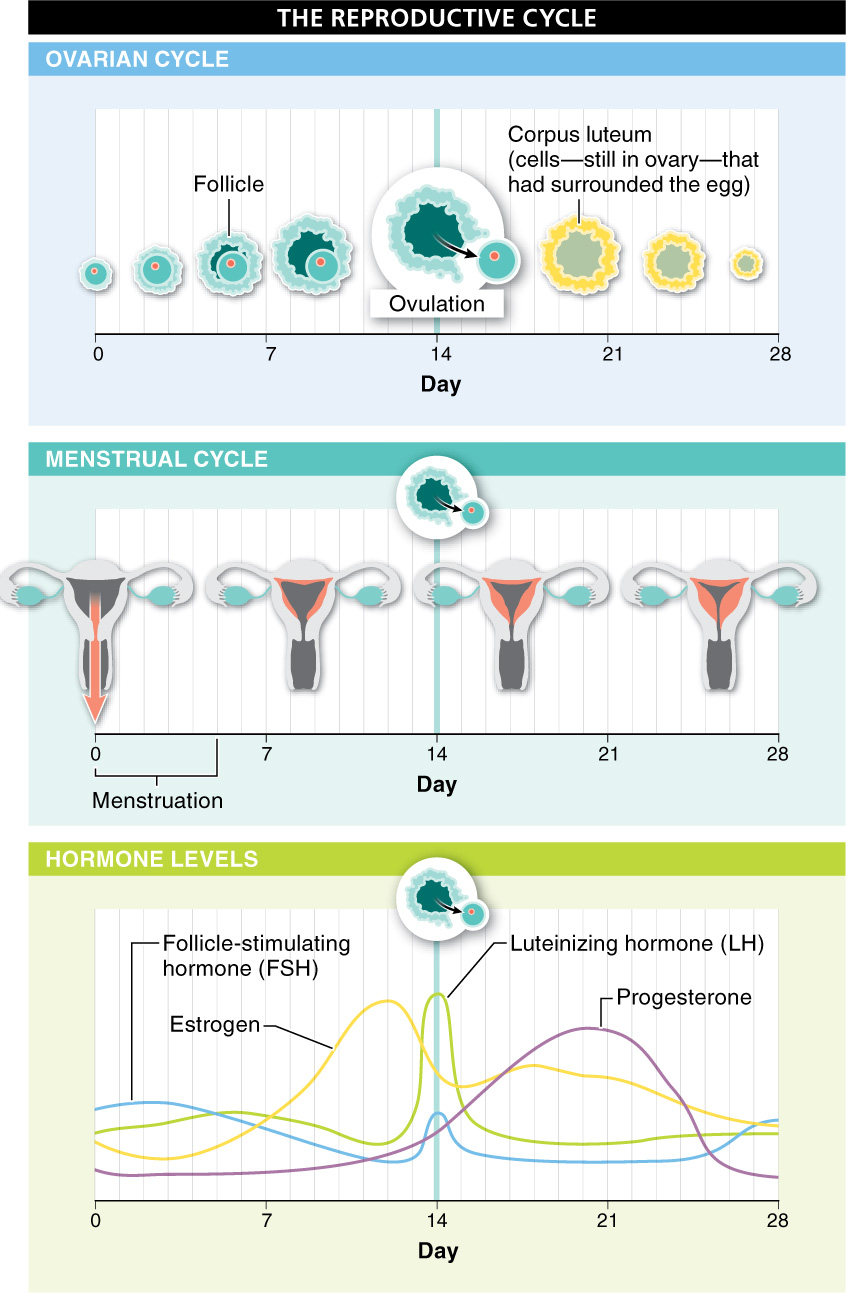
In the normal monthly cycle, hormones direct the development of a follicle and the release of an egg (ovulation), while simultaneously preparing the uterus for implantation. Let’s follow the changes in hormone levels and their effects during the 28-
1020
- Menstruation. Traditionally, the first day of menstrual bleeding, a woman’s “period,” or menstruation, is considered the first day of the menstrual cycle. Three to five days of bleeding occur as the lining of the uterus (the endometrium) is sloughed off.
- FSH produced. As the uterine lining sheds, the levels of estrogen, the chief female sex hormone, drop. Reduced levels of estrogen cause the pituitary gland to release follicle-
stimulating hormone (FSH). - Follicle develops. FSH, just as its name indicates, causes a few follicles in the ovaries to grow and develop, although only one follicle reaches full maturity. Within this one follicle, the primary oocyte completes its first meiotic division and becomes a secondary oocyte.
- Estrogen produced. As the follicles develop, they produce estrogen, gradually increasing the level of estrogen in the blood.
- LH released. The high levels of estrogen trigger the release of a burst of luteinizing hormone (LH) and more FSH.
- Ovulation. The burst of LH triggers ovulation, causing the secondary oocyte to erupt from the follicle and out of the ovary. This release occurs approximately halfway through the menstrual cycle, around day 14, and signals the end of the follicular phase.
- Progesterone produced. As the second half, or luteal phase, of the reproductive cycle begins, the follicle cells that had surrounded the oocyte develop into a structure called the corpus luteum (Latin for “yellow body”). These cells begin secreting smaller amounts of estrogen, but increasing amounts of progesterone.
- Endometrium thickens. Just as its name suggests, progesterone (pro = for; gestare = to bear) causes the body to prepare for gestation of an embryo, in case fertilization occurs. Progesterone’s primary effect is to cause a thickening of the endometrium, or lining of the uterus. The endometrium becomes increasingly rich with blood vessels and deposits of glycogen that can nourish a developing embryo.
1021
At this point, the process can go in one of two directions, depending on whether or not the egg is fertilized (FIGURE 25-18).
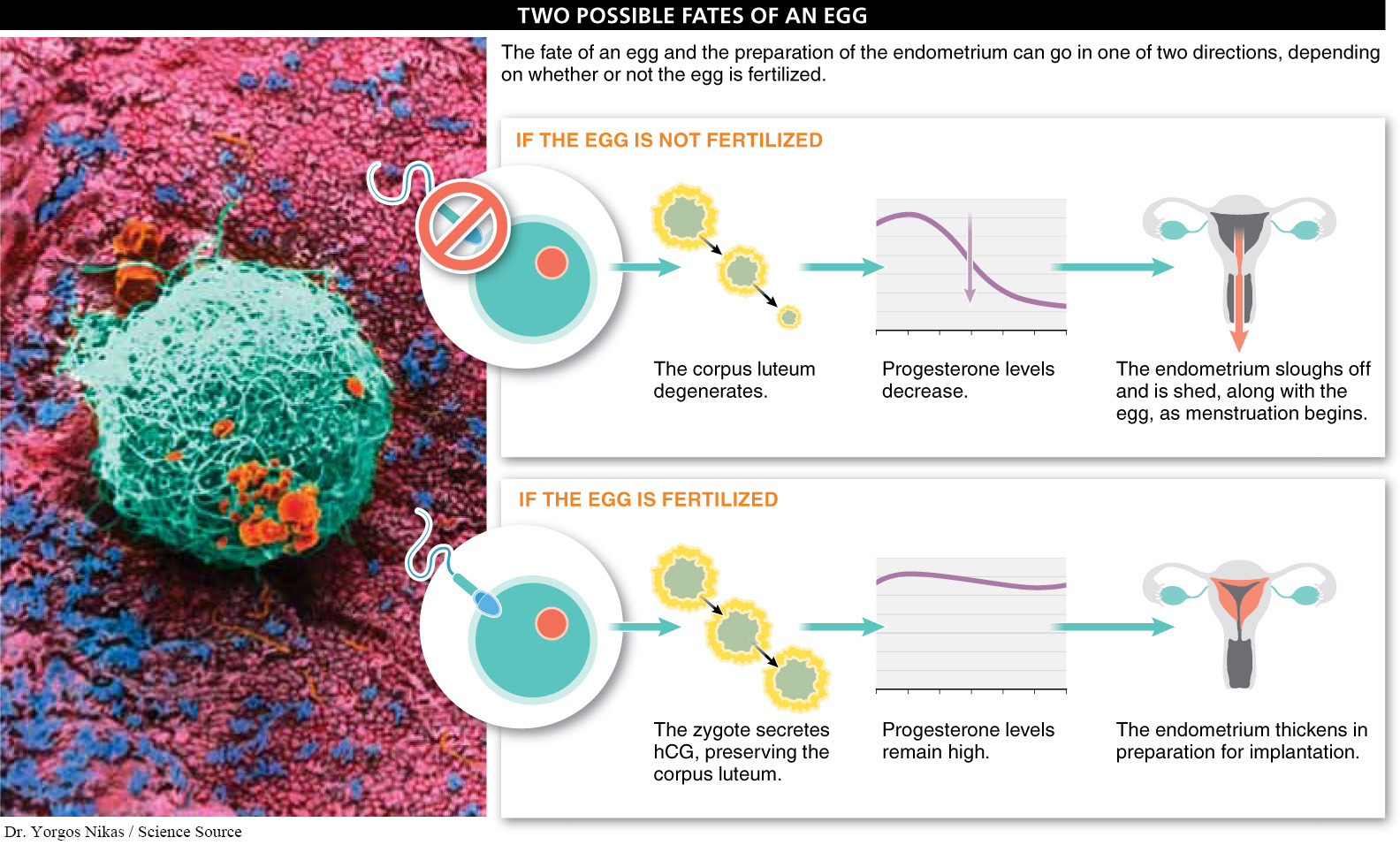
If the egg is not fertilized, the egg disintegrates and the corpus luteum degenerates, sloughs off, and is shed, along with the disintegrating egg. Abruptly removing this source of estrogen and progesterone causes the lining of the uterus to slough off, and menstruation begins. With continuing reduction in estrogen levels, the pituitary gland is spurred to release FSH, and the process begins again.
If the egg is fertilized, which usually occurs in the Fallopian tube, the zygote begins to develop and after several days begins to secrete human chorionic gonadotropin (hCG). This hormone prevents degradation of the corpus luteum, which continues to secrete progesterone, thereby maintaining the endometrium. In the next section, we investigate what happens next in development of the embryo.
What does the process of being an egg donor entail?
Females have about one million follicles, or potential eggs, when they are born, but most women ovulate fewer than 500 times over the course of their life. This leaves a lot of potential eggs lying around. In the normal course of events, these follicles just disintegrate, but in recent decades, modern medicine has made it possible for a woman to donate her eggs to another woman. The process involves several steps.
First, if you choose to be a donor, each day for about a week you have an injection of a drug that suppresses your own reproductive cycle. The suppression is followed by a week of injections of a fertility drug that contains large amounts of two hormones, LH (luteinizing hormone) and FSH (follicle-
Normal reproductive cycling continues from puberty until menopause—the cessation of ovulation and menstruation—
TAKE-HOME MESSAGE 25.8
In the ovaries, a cell within a follicle is stimulated to develop into a fertile egg by coordinated secretions of the hormones estrogen, FSH, and LH. Preparation of the uterus for implantation of a fertilized egg is coordinated by progesterone.
Describe the role of follicle-
Reduced levels of estrogen during menstruation cause the pituitary gland to release FSH. FSH causes follicles in the ovaries to develop, and the primary oocyte within one of these follicles divides to form a secondary oocyte.
1022