Aneuploidy in Humans
For unknown reasons, an incredibly high percentage of all human embryos that are conceived possess chromosome abnormalities. Findings from studies of women who are attempting pregnancy suggest that more than 30% of all conceptions are spontaneously aborted (miscarried), usually so early in development that the woman is not even aware of her pregnancy. Chromosome defects are present in at least 50% of spontaneously aborted human fetuses, with aneuploidy accounting for most of them. This rate of chromosome abnormality in humans is higher than in other organisms that have been studied; in mice, for example, aneuploidy is found in no more than 2% of fertilized eggs. Aneuploidy in humans usually produces such serious developmental problems that spontaneous abortion results. Only about 2% of all fetuses with a chromosome defect survive to birth.
SEX-
AUTOSOMAL ANEUPLOIDIES Autosomal aneuploidies resulting in live births are less common than sex-
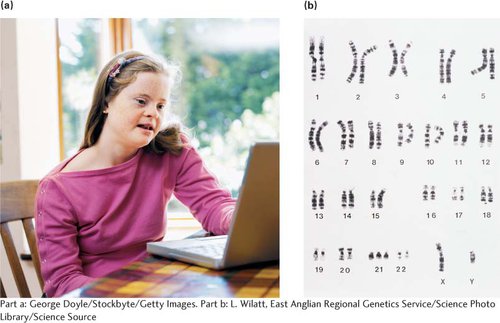
DOWN SYNDROME In 1866, John Langdon Down, physician and medical superintendent of the Earlswood Asylum in Surrey, England, noticed a remarkable resemblance among a number of his intellectually disabled patients: all of them possessed a broad, flat face, a small nose, and oval-
Down syndrome, also known as trisomy 21, is the most common autosomal aneuploidy in humans (Figure 6.19a). The worldwide incidence is about 1 in 700 human births, although the incidence increases among children born to older mothers. Approximately 92% of those who have Down syndrome have three full copies of chromosome 21 (and therefore a total of 47 chromosomes), a condition termed primary Down syndrome (Figure 6.19b). Primary Down syndrome usually arises from spontaneous nondisjunction in egg formation: about 75% of the nondisjunction events that cause Down syndrome are maternal in origin, most arising in meiosis I. Most children with Down syndrome are born to normal parents, and the failure of the chromosomes to divide has little hereditary tendency. A couple who has conceived one child with primary Down syndrome has only a slightly higher risk of conceiving a second child with Down syndrome (compared with other couples of similar age who have not had any children with Down syndrome). Similarly, the couple’s relatives are not more likely to have a child with primary Down syndrome.
About 4% of people with Down syndrome are not trisomic for a complete chromosome 21. Instead, they have 46 chromosomes, but an extra copy of part of chromosome 21 is attached to another chromosome through a translocation. This condition is termed familial Down syndrome because it has a tendency to run in families. The phenotypic characteristics of familial Down syndrome are the same as those of primary Down syndrome.
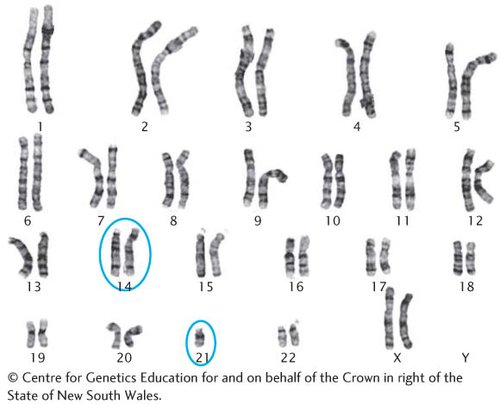
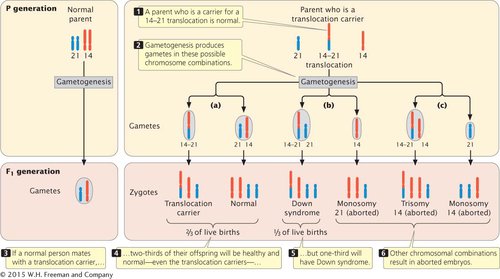
Familial Down syndrome arises in offspring whose parents are carriers of chromosomes that have undergone a Robertsonian translocation, most commonly between chromosome 21 and chromosome 14: the long arm of 21 and the short arm of 14 exchange places (Figure 6.20). This exchange produces one chromosome that includes the long arms of chromosomes 14 and 21 and another, very small chromosome that consists of the short arms of chromosomes 21 and 14. The small chromosome is generally lost after several cell divisions. Although exchange between chromosomes 21 and 14 is the most common cause of familial Down syndrome, the condition can also be caused by translocations between 21 and other chromosomes, such as 15.
People with this type of translocation, called translocation carriers, do not have Down syndrome. Although they possess only 45 chromosomes, their phenotypes are normal because they have two copies of the long arms of chromosomes 14 and 21, and apparently the short arms of these chromosomes (which are lost) carry no essential genetic information. Although translocation carriers are completely healthy, they have an increased chance of producing children with Down syndrome (Figure 6.21)  TRY PROBLEM 22.
TRY PROBLEM 22.
OTHER HUMAN TRISOMIES Few autosomal aneuploidies in humans besides trisomy 21 result in live births. Trisomy 18, also known as Edward syndrome, arises with a frequency of approximately 1 in 8000 live births. Babies with Edward syndrome have severe intellectual disability, low-
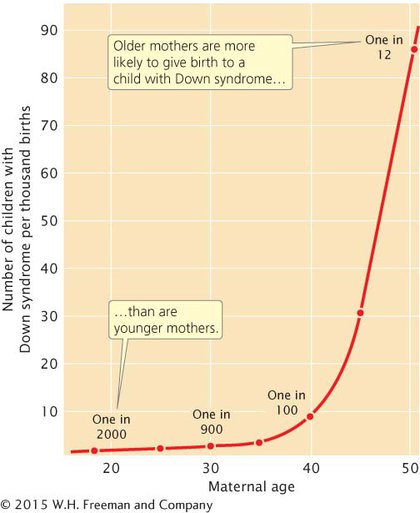
ANEUPLOIDY AND MATERNAL AGE Most cases of Down syndrome and other types of aneuploidy in humans arise from maternal nondisjunction, and the frequency of aneuploidy increases with maternal age (Figure 6.22). Why maternal age is associated with nondisjunction is not known for certain. Female mammals are born with primary oocytes suspended in prophase I of meiosis. Just before ovulation, meiosis resumes and the first division is completed, producing a secondary oocyte. At this point, meiosis is suspended again and remains so until the secondary oocyte is penetrated by a sperm. The second meiotic division takes place immediately before the nuclei of egg and sperm unite to form a zygote.
Primary oocytes may remain suspended in prophase I for many years before ovulation takes place and meiosis recommences. Components of the spindle and other structures required for chromosome segregation may break down during the long arrest of meiosis, leading to more aneuploidy in children born to older mothers. According to this theory, no age effect is seen in males because sperm are produced continuously after puberty, with no long suspension of the meiotic divisions.
ANEUPLOIDY AND CANCER Many tumor cells have extra chromosomes, missing chromosomes, or both; some types of tumors are consistently associated with specific chromosome mutations, including aneuploidy and chromosome rearrangements. The role of chromosome mutations in cancer will be explored in Chapter 16.
CONCEPTS
In humans, sex-
 CONCEPT CHECK 6
CONCEPT CHECK 6
Why are sex-
Dosage compensation prevents the expression of additional copies of X-