9.3 Depressants
Two members of the Beatles, Ringo Starr and John Lennon, both had long periods when they had alcohol use disorder. Starr reported that he “wasted” some years on alcohol, initially feeling that drinking gave him confidence but realizing later that it really didn’t (Graff, 1989). And Lennon was frequently drunk during his 18-month separation from his wife, Yoko Ono.
What Are Depressants?
Alcohol is a depressant. Other depressants are opiates, barbiturates, and benzodiazepines such as diazepam (Valium). In contrast to stimulants, depressants tend to slow a person down, decreasing behavioral activity and level of awareness. Regular use of depressants tends to lead to tolerance, and discontinuing the use of depressants or cutting back on the dosage or frequency can produce withdrawal symptoms. In this section, we will discuss the effects of use and use disorders of three types of depressants: alcohol, barbiturates, and benzodiazepines.
Alcohol
Approximately 6% of Americans aged 12 or older (15 million people) are considered to have alcohol use disorder. Those who start to drink alcohol earlier in life are more likely to develop the disorder (SAMHSA, 2010).
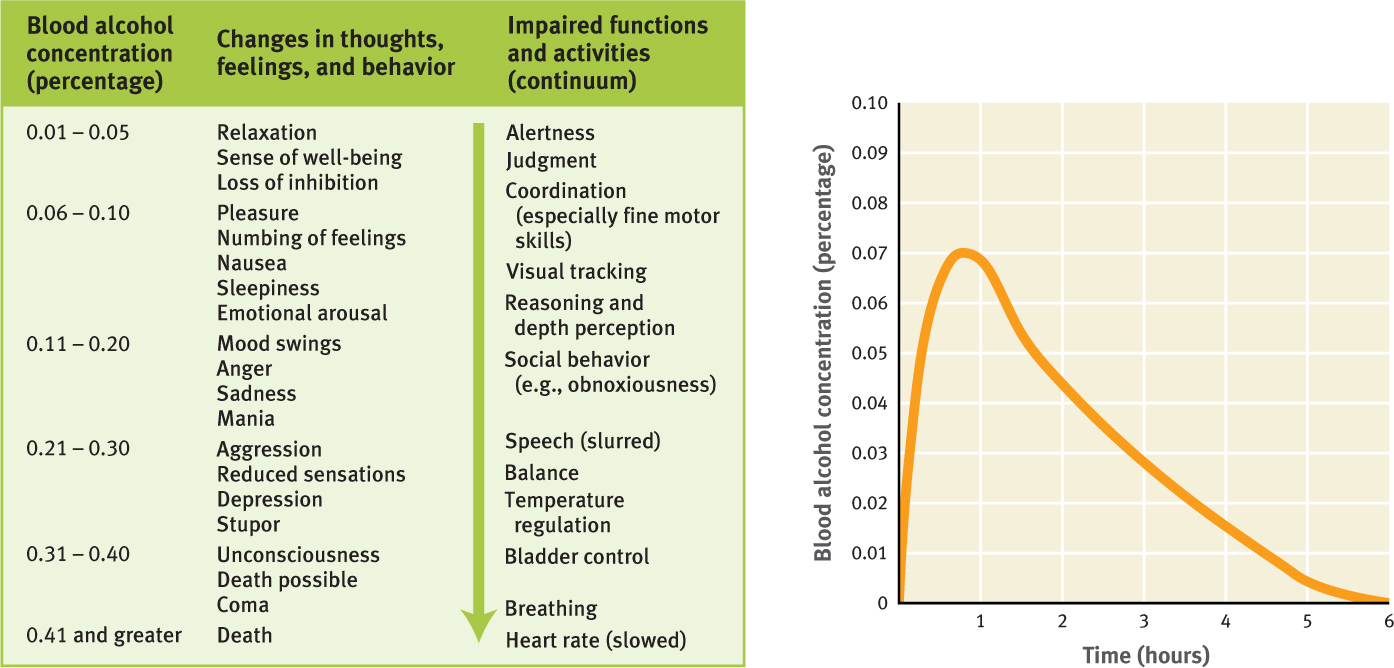
Blood Alcohol Concentration
The crucial variable that determines intoxication is blood alcohol concentration, which is affected by the number of drinks consumed, the period of time over which they were consumed, the time since the person has last eaten, the person’s body weight, and the person’s gender. Different concentrations of alcohol in the blood are associated with different neurological and psychological states (see Figure 9.6). In the United States, Canada, and Mexico, 0.08% is the legal limit of blood alcohol concentration for driving.
The same amount of alcohol will have a slightly greater effect on a woman than a man of the same size and weight because men and women metabolize the drug differently (Frezza et al., 1990). This sex difference arises in part because women have, on average, less total water content in their bodies than do men, which means that ingested alcohol is less diluted (Greenfield, 2002; Van Thiel et al., 1988).
GETTING THE PICTURE

Not only do the effects of a given amount of alcohol differ by gender, but there are also individual differences. Some people have a more intense response to alcohol than do others. This variability appears to be mediated in part by genes (Webb et al., 2011), but it is also related to the level of tolerance a person has acquired.
Binge Drinking
Binge drinking, or heavy episodic drinking, occurs when a person drinks until his or her blood alcohol concentration reaches at least 0.08% in a 2-hour period (which generally translates into four or more drinks for women, five or more for men; one drink is equivalent to 12 ounces of beer, 5 ounces of wine, or 1.5 ounces of 80-proof liquor) (National Institute on Alcohol Abuse and Alcoholism National Advisory Council, 2004). Binge drinking is likely to occur when a person sets out to get drunk (Schulenberg et al., 1996). Repetitive binge drinking can lead to alcohol use disorder.
Alcohol Use Disorder
Chronic drinking leads to tolerance and withdrawal, thus fulfilling the minimum two criteria for alcohol use disorder (sometimes referred to as alcoholism). According to the National Institute on Alcohol Abuse and Alcoholism (2012), alcoholism is marked by four symptoms:
- craving, which is a strong need, or urge, to drink;
- loss of control, which consists of an episode of drinking during which the person finds it difficult to stop compulsively drinking;
- physical dependence, which brings withdrawal symptoms, such as nausea, sweating, shakiness, and anxiety after stopping drinking; and
- tolerance, which causes a person to need to drink greater amounts of alcohol to get “high.”
CASE 9.3 • FROM THE INSIDE: Alcohol Use Disorder
Caroline Knapp describes her alcohol use disorder in her memoir Drinking: A Love Story (1997):
By that point I don’t even think the alcohol worked anymore. Certainly drinking was no longer fun. It had long ago ceased to be fun. A few glasses of wine with a friend after work could still feel reassuring and familiar, but drinking was so need driven by the end, so visceral and compulsive, that the pleasure was almost accidental. Pleasure just wasn’t the point. At the end I didn’t even feel like myself until I had a drink or two, and I remember that scared me a little: alcohol had become something I felt I needed in order to return to a sense of normalcy, in order to think straight. After one or two drinks I’d feel like I’d come back into my own skin—more clearheaded, more relaxed—but the feeling would last for only half an hour or so. Another few drinks and I’d be gone again, headed toward oblivion.
(p. 231)
In Case 9.3, Knapp describes the four elements of alcoholism: craving (“need driven”), loss of control (she would continue to drink until she was “headed toward oblivion”), physical dependence (“something I felt I needed in order to return to normalcy”), and tolerance (the alcohol didn’t have as strong an effect as it had initially).
Alcohol use disorder is also associated with memory problems, in particular, blackouts, periods of time during which the drinker cannot later remember what transpired while he or she was intoxicated. Knapp (1997) described her blackouts: “Sometimes I’d wake up at Sam’s [a friend’s] house, in his bed, wearing one of his T-shirts. I don’t think we ever had sex but I can’t say for sure”.
Sedative-Hypnotic Drugs
Sedative-hypnotic drugs reduce pain and anxiety, relax muscles, lower blood pressure, slow breathing and heart rate, and induce sedation and sleep. In general, drugs in this class cause disinhibiting and depressant effects similar to those of alcohol (impaired physical coordination and mental judgment and increased aggressive or sexual behavior). Although these psychoactive substances can lower inhibitions and bring a sense of well-being, they also can cause memory problems, confusion, poor concentration, fatigue, and even respiratory arrest (NIDA, 2008e). When sedative-hypnotic drugs are mixed with another depressant, such as alcohol, the combined effect can be lethal: The person’s breathing and heart rate can slow to the point where the person dies. Chronic use of these drugs can lead to tolerance. Two general types of drugs are in this class: barbiturates and benzodiazepines.
Barbiturates
Barbiturates, which include amobarbital (Amytal), pentobarbital (Nembutal), and secobarbital (Seconal), are usually prescribed to treat sleep problems. Although use of a barbiturate is legal with a prescription, this type of medication is commonly abused by both those with a prescription and those who obtain the drug illegally. As with other depressants, repeated barbiturate use leads to tolerance, so the person takes ever larger doses to get to sleep or reduce anxiety. Repeated barbiturate use can also lead to withdrawal symptoms, including agitation and restlessness, hallucinations, confusion, and, in some cases, seizures (NIDA, 2005c). People with barbiturate use disorder who want to discontinue or decrease their intake of the drug should do so with care; they should first consult a knowledgeable physician to determine an appropriate schedule for tapering off without inducing dangerous withdrawal symptoms. If they discontinue the drug abruptly, they risk having convulsions and could even die.
Benzodiazepines
Benzodiazepines are usually prescribed to alleviate muscle pain, to aid sleep, or as a short-term treatment for anxiety (see Chapter 6); however, long-term use leads to tolerance and withdrawal. Examples of benzodiazepines include lorazepam (Ativan), triazolam (Halcion), clonazepam (Klonopin), diazapam (Valium), and alprazolam (Xanax). As with barbiturate use disorder, a person with benzodiazepine use disorder should gradually taper off of the drug, in consultation with a physician; abruptly stopping use can lead to seizures and psychosis. A benzodiazepine-like class of sedative drugs, referred to as nonbenzodiazepines, can also be abused and have similar effects, side effects, and risks. Examples include zolpidem (Ambien), eszopiclone (Lunesta), and zaleplon (Sonata).
Understanding Depressants
In what follows, we will first discuss how brain systems and neural communication are affected by depressants in general and then turn to the effects of alcohol in particular.
Neurological Factors
In this section, we consider a set of closely related topics: the effects of depressants on the brain systems and neural communication, biological by-products of alcohol use disorder, and the genetics of alcoholism.
Brain Systems and Neural Communication
Benzodiazepines (such as Xanax), barbiturates, and alcohol directly affect the GABAnergic system, which is widespread in the brain and primarily activates inhibitory neurons. The resulting inhibition affects neurons in brain structures that are involved in anxiety, such as the amygdala. As we’ve noted before, the amygdala plays a key role in fear, and hence inhibiting it dulls the sense of fear and the related feeling of anxiety. Thus, it is not surprising that people who experience anxiety, for whatever reasons, find the use of depressants particularly reinforcing.
Although alcohol consumption induces the production of dopamine, which is rewarding, chronic use of alcohol stimulates the production of a type of neurotransmitter called endogenous opioids, sometimes referred to as “pleasure chemicals.” (There is a class of drugs referred to as opioids or opiates, which we’ll discuss later in the chapter. The word endogenous—which means arises from an inside source—is used to distinguish the neurotransmitter opioids from the drugs of the same name.) Endogenous opioids are responsible for “runner’s high,” the feeling that occurs when someone has pushed herself or himself to a physical limit and experiences a sense of deep pleasure. In chronic drinkers, the activity of endogenous opioids occurs only in response to alcohol; when they stop drinking, their bodies no longer produce endogenous opioids. Thus, when a chronic drinker isn’t consuming alcohol, he or she may experience symptoms related to opioid withdrawal, which are unpleasant. This experience in turn may induce the person to consume more alcohol to produce more opioids (Gianoulakis, 2001). In addition, a single drink releases more opioids in heavy drinkers than in light drinkers (Mitchell et al., 2012). This is only a correlation, but one possible explanation for it is that some people may become heavy drinkers, in part, because their brains release more opioids in response to alcohol, thus activating the dopamine reward system.
Biological By-products of Alcohol Use Disorder
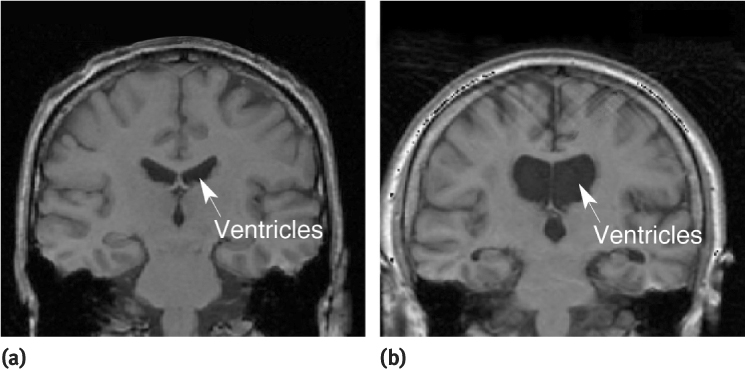
People who frequently drink a lot of alcohol may become malnourished when the calories in alcohol substitute for calories from food (Mehta et al., 2006). Such malnourishment can include a deficiency in vitamin B1, which eventually causes several key parts of the brain to atrophy—including brain structures important for storing new information in memory. Thus, drinking a lot of alcohol can indirectly lead to chronic memory problems (which produces a condition called Korsakoff’s syndrome). Figure 9.7 shows a result of such brain atrophy: the increased size of the fluid-filled hollow areas, the ventricles, in the center of the brain.
For people with alcohol use disorder, a hangover indicates that their bodies are going through alcohol withdrawal as the alcohol leaves the system (Cicero, 1978); drinking more alcohol can temporarily diminish the discomfort of the withdrawal symptoms.
Delirium tremens (DTs) The symptoms of alcohol withdrawal that include uncontrollable shaking, confusion, convulsions, visual hallucinations, and fever.
For a heavy drinker, withdrawal symptoms include headaches, weakness, tremors, anxiety, higher blood pressure, seizures, and increased heart and breathing rates. An extremely heavy drinker can also experience fever, agitation, and irritability, as well as more severe symptoms such as uncontrollable shaking, confusion, convulsions, and visual hallucinations. All these alcohol withdrawal symptoms are collectively referred to as delirium tremens (also simply called “the DTs”). Such withdrawal symptoms normally begin within 4 days after the person last drank alcohol (Romach & Sellers, 1991). Delirium tremens can be potentially lethal; when people with alcohol use disorder are ready to stop drinking, they should have a physician supervise the process.
Genetics of Alcoholism
The tendency to abuse drugs is affected by genes (Palmer et al., 2012). One sign of this is the fact that substance use disorders tend to run in families. However, only the genetics of alcoholism has been studied in depth. Researchers have found that biological offspring of alcoholics are about twice as likely to become alcoholics as people without such a family history (Nurnberger et al., 2004; Russell, 1990). Twin studies have also provided evidence for a genetic contribution to alcoholism (Carmelli et al., 1993). In addition, sometimes the offspring of alcoholics are adopted by parents who are not alcoholics, and researchers have studied some of these children after they’ve become adults. One striking finding is that even when they were raised by nonalcoholic parents, children whose biological parents were alcoholics are much more likely to abuse alcohol as adults than are those whose biological parents were not alcoholics (Kendler, Sundquist, et al., 2013). TABLE 9.8 summarizes the neurological factors that contribute to use disorders of depressants.
|
| *This factor is not unique to depressant use disorder. |
Psychological Factors
Many of the psychological factors that contribute to use disorders of stimulants also contribute to use disorders of depressants (see the starred items in TABLE 9.6); in particular:
- observational learning of depressant use, which promotes expectations about experiences from such use and promotes such use as a coping strategy;
- operant conditioning, in which
- ° positive reinforcement leads to positive expectations of depressant use and to reward craving;
- ° negative reinforcement can lead to relief craving and to depressant use becoming a chronic coping strategy; and
- classical conditioning, whereby drug cues elicit cravings.
Let’s examine in a bit more detail the role of coping strategies and expectations in alcohol use. Some people use alcohol as a way to cope with their problems. Consider Charles’s experience in Case 9.4.
CASE 9.4 • FROM THE OUTSIDE: Alcohol Use Disorder as a Coping Strategy
Charles, a high-school teacher with a long-standing problem of alcohol [use disorder], identified boredom and anger as key high-risk relapse factors. His problem with anger involved a pattern of avoiding interpersonal conflicts and letting his anger build up. Over time, Charles would reach a point of total frustration and use his angry thoughts and feelings to justify drinking binges. [He had perceived his anger to be a] “bad feeling that could only be expressed through drinking”…he often became upset and angry because of certain beliefs he held about how others “should” treat him.
(Daley & Salloum, 1999, p. 258)
Like Charles, other people use alcohol to try to cope with particular emotions. In Charles’s case, it was anger; for other people, the emotions might be sadness, anxiety, fear, shame, or any of a range of other emotions (Gaher et al., 2006). Particular factors lead some people to have a higher risk of using alcohol to cope. One such factor relates to the trait of anxiety sensitivity (see Chapter 6): People who are high in this trait find alcohol to be very calming, which explains why an anxiety disorder frequently precedes an alcohol use disorder in people who have both kinds of disorders (Robinson et al., 2011; Stewart et al., 2001).
Finally, even when they are not related to a coping strategy, expectations of what will happen as a result of drinking can also affect behavior after drinking (Kirsch & Lynn, 1999): People who drink to get “wasted” are in fact more likely to feel and act more drunk than are people who drink while having dinner with friends in a restaurant, even when people in both situations end up with the same blood alcohol concentration.
Social Factors

A variety of social factors can contribute to substance use disorders (see the starred items in TABLE 9.7). For depressants, including alcohol, such factors include:
- dysfunctional family interactions (such as child abuse or neglect);
- peers’ use of depressants;
- norms or perceived norms about depressant use (as in a subculture where drinking is the norm or is perceived to be so); and
- economic hardship and unemployment.
Another social factor is culture: Culture affects both the degree of alcohol abuse and the ways in which alcohol is used (Abbott & Chase, 2008). For example, the rate of alcohol use disorder among American women has increased over time. Historically, women in the United States had much lower rates of alcoholism than did men, but as social mores and roles for women changed, the incidence of alcoholism among women has come to approach that of men (Greenfield, 2002).
Cultures also create social norms for appropriate and inappropriate use of alcohol, such as allowing “fiesta” drunkenness on certain occasions (Finch, 2001; Room & Makela, 2000). Moreover, the media influence norms and perceived norms. One correlational study found that adolescents and young adults who saw more ads for alcohol drank more alcohol (Snyder et al., 2006), possibly because seeing more ads for alcohol led them to perceive the norm for alcohol use to be greater than it was.
Thinking Like A Clinician
When you see your neighbor in the hallway in the evenings, she sometimes can’t seem to walk in a straight line, her speech is slurred, and she reeks of alcohol. She frequently misses when she tries to put her key in the lock and begins giggling. Once you saw her vomit after such an incident. On a few occasions, she hasn’t been so obviously “wasted” and has turned to you and roughly said, “What are you staring at?” One time, when you smirked as she tried to put her key in the lock, she came over to you and threatened to “kick your butt.” Even during the daytime, though, she’s not very nice or friendly.
Do you think this neighbor has a problem with alcohol, and if so, does it reach the level to be considered alcohol use disorder? Why or why not? What supports or refutes the conclusion that she has an alcohol problem? What information would you want to know before making a confident decision? According to the neuropsychosocial approach, what factors might underlie this neighbor’s use of alcohol?