15.2 Psychological Treatments: Healing the Mind through Interaction
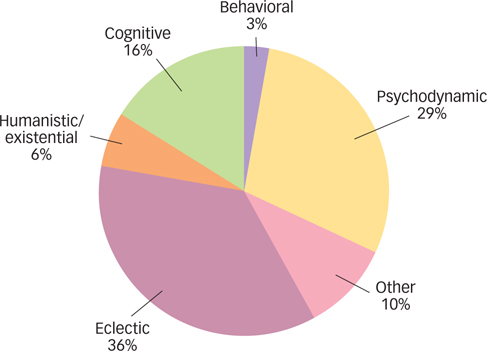
Psychological therapy, or psychotherapy, is an interaction between a socially sanctioned clinician and someone suffering from a psychological problem, with the goal of providing support or relief from the problem. Currently, over 500 different forms of psychotherapy exist. A survey of 1,000 psychotherapists asked them to describe their main theoretical orientation (Norcross, Hedges, & Castle, 2002; see FIGURE 15.1). Over a third reported using eclectic psychotherapy, a form of psychotherapy that involves drawing on techniques from different forms of therapy, depending on the client and the problem. This allows therapists to apply an appropriate theoretical perspective suited to the problem at hand, rather than adhering to a single theoretical perspective for all clients and all types of problems. Nevertheless, as FIGURE 15.1 shows, the majority of psychotherapists use a single approach, such as psychodynamic therapy, humanistic and existential therapies, or behavioral and cognitive therapies. We’ll examine each of those four major branches of psychotherapy in turn.
psychotherapy
An interaction between a socially sanctioned clinician and someone suffering from a psychological problem, with the goal of providing support or relief from the problem.
eclectic psychotherapy
A form of psychotherapy that involves drawing on techniques from different forms of therapy, depending on the client and the problem.
Psychodynamic Therapy
Psychodynamic psychotherapy has its roots in Freud’s psychoanalytically oriented theory of personality. Psychodynamic psychotherapies are therapies that explore childhood events and encourage individuals to use the understanding that results to develop insight into their psychological problems. Psychoanalysis was the first psychodynamic therapy to develop, but it has largely been replaced by modern psychodynamic therapies, such as interpersonal psychotherapy.
psychodynamic psychotherapies
Therapies that explore childhood events and encourage individuals to use the understanding that results to develop insight into their psychological problems.
482
Psychoanalysis
As you saw in the Personality chapter, psychoanalysis assumes that people are born with aggressive and sexual urges that are repressed during childhood development through the use of defense mechanisms. Psychoanalysts encourage their clients to bring these repressed conflicts into consciousness so that the clients can understand them and reduce their unwanted influences.
Traditional psychoanalysis involves four or five sessions per week over an average of 3 to 6 years (Ursano & Silberman, 2003). During a session, the client reclines on a couch, facing away from the analyst, and is asked to express whatever thoughts and feelings come to mind. Occasionally, the therapist may comment on some of the information presented by the client but does not express his or her values and judgments. The stereotypic image you might have of psychological therapy—
The goal of psychoanalysis is for the client to understand the unconscious in a process Freud called developing insight. Some key techniques that psychoanalysts use to help the client develop insight include free association, in which the client reports every thought that enters the mind and the therapist looks for recurring themes, and dream analysis, in which the therapist looks for dream elements that might symbolize unconscious conflicts or wishes. Psychoanalysts also assess the client’s resistance, or a reluctance to cooperate with treatment for fear of confronting unpleasant unconscious material. For example, the therapist might suggest that the client’s problem with obsessive health worries could be traced to a childhood rivalry with her mother for her father’s love and attention. The client could find the suggestion insulting and resist the interpretation, which might signal to the therapist that this is indeed an issue the client could be directed to confront in order to develop insight.
resistance
A reluctance to cooperate with treatment for fear of confronting unpleasant unconscious material.
What might a client’s resistance signal to a psychoanalyst?
Over time and many therapy sessions, the client and psychoanalyst often develop a close relationship. Freud believed that the development and resolution of this relationship was a key process of psychoanalysis. Transference is an event that occurs when the analyst begins to assume a major significance in the client’s life and the client reacts to the analyst based on unconscious childhood fantasies. Successful psychoanalysis involves analyzing the transference so that the client understands this reaction and why it occurs.
transference
An event that occurs in psychoanalysis when the analyst begins to assume a major significance in the client’s life and the client reacts to the analyst based on unconscious childhood fantasies.

Beyond Psychoanalysis
Although Freud’s insights and techniques are fundamental, modern psychodynamic treatments differ from classic psychoanalysis in both their content and procedures. One of the most widely used psychodynamic treatments is interpersonal psychotherapy (IPT), a form of psychotherapy that focuses on helping clients improve current relationships (Weissman, Markowitz, & Klerman, 2000). Rather than using free association, therapists using IPT talk to clients about their interpersonal behaviors and feelings. The therapists pay particular attention to the client’s grief (an exaggerated reaction to the loss of a loved one), role disputes (conflicts with a significant other), role transitions (changes in life status, such as starting a new job, getting married, or retiring), or interpersonal deficits (lack of the necessary skills to start or maintain a relationship). The treatment assumes that, as interpersonal relations improve, symptoms will subside.
interpersonal psychotherapy (IPT)
A form of psychotherapy that focuses on helping clients improve current relationships.
483
Modern psychodynamic psychotherapies such as IPT also differ from classical psychoanalysis in the procedures used. For starters, in modern psychodynamic therapy, the therapist and client typically sit face-
In what ways do modern psychodynamic treatments differ from Freudian analysis?
Although psychodynamic therapy has been around for a long time and continues to be widely practiced, there is relatively little evidence for its effectiveness. Moreover, there is some evidence that some aspects of psychodynamic therapy may actually be harmful. For instance, research suggests that the more a therapist makes interpretations about perceived transference in the client, the worse the therapeutic alliance and the worse the clinical outcome (Henry et al., 1994). Psychodynamic therapy is not as widely used as it once was, but many psychologists still use it in practice, and many people say that they find it helpful.

Humanistic and Existential Therapies
Humanistic and existential therapies emerged in part as a reaction to the negative views that psychoanalysis holds about human nature. Humanistic and existential therapies share the assumption that psychological problems stem from feelings of alienation and loneliness, and that those feelings can be traced to failures to reach one’s potential (in the humanistic approach) or from failures to find meaning in life (in the existential approach). Although interest in these approaches peaked in the 1960s and 1970s, some therapists continue to use these approaches today. Two well-
How does a humanistic view of human nature differ from a psychodynamic view?
Person-Centered Therapy
Person-centered therapy (or client-centered therapy) assumes that all individuals have a tendency toward growth and that this growth can be facilitated by acceptance and genuine reactions from the therapist. Psychologist Carl Rogers (1902-
person-centered therapy (or client-centered therapy)
Assume that individuals have a tendency toward growth and that this growth can be facilitated by acceptance and genuine reactions from the therapist.
484
Person-
The goal is not to uncover repressed conflicts, as in psychodynamic therapy, but instead to try to understand the client’s experience and reflect that experience back to the client in a supportive way, encouraging the client’s natural tendency toward growth. This style of therapy is reminiscent of psychoanalysis in its way of encouraging the client toward the free expression of thoughts and feelings.
Gestalt Therapy

Gestalt therapy was founded by Frederick “Fritz” Perls (1893–
gestalt therapy
Has the goal of helping the client become aware of his or her thoughts, behaviors, experiences, and feelings and to “own” or take responsibility for them.
Gestalt therapy emphasizes the experiences and behaviors that are occurring at that particular moment in the therapy session. For example, if a client is talking about something stressful that occurred during the previous week, the therapist might ask, “How do you feel now as you describe what happened to you?” Clients are also encouraged to put their feelings into action. One way to do this is the empty chair technique, in which the client imagines that another person (e.g., a spouse, a parent, or a co-
Behavioral and Cognitive Therapies
Unlike the talk therapies described earlier, behavioral and cognitive treatments emphasize actively changing a person’s current thoughts and behaviors as a way to decrease or eliminate the patient’s psychopathology. In the evolution of psychological treatments, clients started out lying down in psychoanalysis, then sitting in psychodynamic and related approaches, but they are often standing and engaging in behavior-
Behavior Therapy
What primary problem did behaviorists have with psychoanalytic ideas?
Whereas Freud developed psychoanalysis as an offshoot of hypnosis and other techniques used by other clinicians before him, behavior therapy was developed based on laboratory findings from earlier behavioral psychologists. As you read in the Psychology: Evolution of a Science chapter, behaviorists rejected theories that were based on “invisible” mental properties that were difficult to test and impossible to observe directly. Behaviorists found psychoanalytic ideas particularly hard to test: How do you know whether a person has an unconscious conflict? Behavioral principles, in contrast, focused solely on behaviors that could be observed (e.g., avoidance of a feared object, such as refusing to get on an airplane). Behavior therapy is a type of therapy that assumes that disordered behavior is learned and that symptom relief is achieved through changing overt maladaptive behaviors into more constructive behaviors. A variety of behavior therapy techniques have been developed for many disorders, based on the learning principles you encountered in the Learning chapter, including operant conditioning procedures (which focus on reinforcement and punishment) and classical conditioning procedures (which focus on extinction). Here are three examples of behavior therapy techniques in action:
behavior therapy
A type of therapy that assumes that disordered behavior is learned and that symptom relief is achieved through changing overt maladaptive behaviors into more constructive behaviors.
485

token economy
A form of behavior therapy in which clients are given “tokens” for desired behaviors, which they can later trade for rewards.
- Eliminating Unwanted Behaviors. How would you change a 3-
year- old boy’s habit of throwing tantrums at the grocery store? A behavior therapist might investigate what happens immediately before and after the tantrum: Did the child get candy to “shut him up?” The study of operant conditioning shows that behavior can be influenced by its consequences (the reinforcing or punishing events that follow). Adjusting these consequences might help change the behavior. Making them less reinforcing (no candy!) and more punishing (a period of time- out facing the wall in the grocery store while the parent watches from nearby rather than providing a rush of attention) could eliminate the problem behavior. - Promoting Desired Behaviors. Candy and a time-
out can have a strong influence on child behavior, but they work less well with adults. How might you get an individual with schizophrenia to engage in activities of daily living? How would you get a cocaine addict to stop using drugs? A behavior therapy technique that has proven to be quite effective in such cases is the token economy, a form of behavior therapy in which clients are given “tokens” for desired behaviors, which they can later trade for rewards. For instance, in the case of cocaine dependence, the desired behavior is not using cocaine. Programs that reward nonuse (verified by urine samples) with vouchers that can be exchanged for rewards such as money, bus passes, clothes, and so on, have shown an ability to significantly reduce cocaine use and associated psychological problems (Petry, Alessi, & Rash, 2013). Similar systems are used to promote desired behaviors in classrooms, the work- place, and commercial advertising (e.g., airline and credit card rewards programs). Table : Table 15.1 Exposure Hierarchy for Social PhobiaItem
Fear (0-
100) 1. Have a party and invite everyone from work
99
2. Go to a holiday party for 1 hour without drinking
90
3. Invite Cindy to have dinner and see a movie
85
4. Go for a job interview
80
5. Ask boss for a day off from work
65
6. Ask questions in a meeting at work
65
7. Eat lunch with co-
workers 60
8. Talk to a stranger on a bus
50
9. Talk to cousin on the telephone for 10 minutes
40
10. Ask for directions at a gas station
35
Source: Information from Ellis, 1991.
- Reducing Unwanted Emotional Responses. One of the most powerful ways to reduce fear is by gradual exposure to the feared object or situation. Exposure therapy is an approach to treatment that involves confronting an emotion-
arousing stimulus directly and repeatedly, ultimately leading to a decrease in the emotional response . This technique depends on the processes of habituation and response extinction. For example, in Christine’s case, her clinician gradually exposed her to the content of her obsessions (dirt and germs), which became less and less distressing with repeated exposure. Similarly, for clients who are afraid of social interaction and are unable to function at school or work, a behavioral treatment might involve exposure first to imagined situations in which they talk briefly with one person, then a bit longer talk to a medium-sized group, and finally, giving a speech to a large group. It’s now known that in vivo (live) exposure is more effective than imaginary exposure (Choy, Fyer, & Lipsitz, 2007). In other words, if a person fears social situations, it is better for that person to practice social interaction than merely to imagine it. Behavioral therapists use an exposure hierarchy to expose the client gradually to the feared object or situation. Easier situations are practiced first, and as fear decreases, the client progresses to more difficult or frightening situations (see TABLE 15.1). exposure therapy
An approach to treatment that involves confronting an emotion-
arousing stimulus directly and repeatedly, ultimately leading to a decrease in the emotional response.
486

Cognitive Therapy
Whereas behavior therapy focuses primarily on changing a person’s behavior, cognitive therapy focuses on helping a client identify and correct any distorted thinking about self, others, or the world (Beck, 2005). For example, behaviorists might explain a phobia as the outcome of a classical conditioning experience such as being bitten by a dog, where the dog bite leads to the development of a dog phobia through the association of the dog with the experience of pain. Cognitive theorists might instead emphasize the interpretation of the event and focus on a person’s new or strengthened belief that dogs are dangerous to explain the fear.
cognitive therapy
Focuses on helping a client identify and correct any distorted thinking about self, others, or the world.
Cognitive therapies use a technique called cognitive restructuring, a therapeutic approach that teaches clients to question the automatic beliefs, assumptions, and predictions that often lead to negative emotions and to replace negative thinking with more realistic and positive beliefs. Specifically, clients are taught to examine the evidence for and against a particular belief or to be more accepting of outcomes that may be undesirable yet still manageable. For example, a depressed client may believe that she is stupid and will never pass her college courses—
cognitive restructuring
A therapeutic approach that teaches clients to question the automatic beliefs, assumptions, and predictions that often lead to negative emotions and to replace negative thinking with more realistic and positive beliefs.
487
|
Clinician |
Last week, I asked you to keep a thought record of both the situations that made you feel very depressed and the automatic thoughts that popped into your mind. Were you able to do that? |
|
Client |
Yes. |
|
Clinician |
Wonderful, I’m glad you were able to complete this assignment. Let’s take a look at this together. What’s the first situation that you recorded? |
|
Client |
Well … I went out on Friday night with my friends, which I thought would be fun. But I was feeling kind of down about things and I ended up not really talking to anyone. Instead I just sat in the corner and drank all night. I got so drunk that I passed out at the party. I woke up the next day feeling embarrassed and more depressed than ever. |
|
Clinician |
OK, and what thoughts automatically popped into your head? |
|
Client |
My friends think I’m a loser and will never want to hang out with me again. |
|
Clinician |
What evidence can you think of that supports this thought? |
|
Client |
Well … um … I got really drunk and so they have to think I’m a loser. I mean, who does that? |
|
Clinician |
Is there any other evidence you can think of that supports those thoughts? |
|
Client |
No. |
|
Clinician |
All right. Now let’s take a moment to think about whether there is any evidence that doesn’t support those thoughts. Did anything happen that suggests that your friends do want to keep hanging out with you? |
|
Client |
Well … my friends brought me home safely and then called the next day and joked about what happened and my one friend Tommy said something like, “we’ve all been there,” and that he wants to hang out again this weekend. |
|
Clinician |
This is very interesting. So on one hand, you feel depressed and have thoughts that you are a loser and your friends don’t like you. But on the other hand, you have some pretty real- |
|
Client |
Yeah, I guess you’re right if you put it that way. I didn’t think about it like that. |
|
Clinician |
So now if we were going to replace your first thoughts, which don’t seem to have a lot of real- |
|
Client |
Probably something like, my friends probably weren’t happy about the fact that I got so drunk because then they had to take care of me, but they are my friends and were there for me and want to keep hanging out with me. |
|
Clinician |
Excellent job. I think that sounds just right based on the evidence. |
How might a client restructure a negative self-
In addition to cognitive restructuring techniques, which try to change a person’s thoughts to be more balanced or accurate, some forms of cognitive therapy also include techniques for coping with unwanted thoughts and feelings, techniques that resemble meditation (see the Consciousness chapter). One such technique, called mindfulness meditation, teaches an individual to be fully present in each moment; to be aware of his or her thoughts, feelings, and sensations; and to detect symptoms before they become a problem. In one study, people recovering from depression were about half as likely to relapse during a 60-
mindfulness meditation
Teaches an individual to be fully present in each moment; to be aware of his or her thoughts, feelings, and sensations; and to detect symptoms before they become a problem.

Cognitive Behavioral Therapy
How does cognitive behavioral therapy differ from psychodynamic therapy?
Historically, cognitive and behavioral therapies were considered distinct systems of therapy. Today, most therapists working with anxiety and depression use a blend of cognitive and behavioral therapeutic strategies, often referred to as cognitive behavioral therapy (CBT). In contrast to traditional behavior therapy and cognitive therapy, CBT is problem focused, meaning that it is undertaken for specific problems (e.g., reducing the frequency of panic attacks or returning to work after a bout of depression), and action oriented, meaning that the therapist tries to assist the client in selecting specific strategies to help address those problems. The client is expected to do things, such as engage in exposure exercises, practice behavior change skills or use a diary to monitor relevant symptoms (e.g., the severity of a depressed mood or panic attack symptoms). This is in contrast to psychodynamic or other therapies in which goals may not be explicitly discussed or agreed on and the client’s only necessary action is to attend the therapy session.
cognitive behavioral therapy (CBT)
A blend of cognitive and behavioral therapeutic strategies.
488
Hot Science: “Rebooting” Psychological Treatment
“Rebooting” Psychological Treatment
Modern psychotherapy has advanced far beyond the days of Freud and his free-
For example, research suggests that biases in the ways that people process information cause psychological disorders. Cognitive bias modification (CBM) is a computerized intervention that focuses on eliminating these biases (MacLeod & Mathews, 2012). Specifically, people with social anxiety show selective attention for threatening information (e.g., when shown several faces, they have an automatic tendency to look at the angrier one). In one form of CBM for social anxiety, the patient completes a computerized training program in which he or she is repeatedly shown pairs of faces, one angry and one neutral, that flash on the screen very quickly (for 500 milliseconds), after which a letter appears behind one of them and the patient’s task is to name that letter. In CBM, the letter nearly always appears behind the neutral face, which over time teaches the person to ignore the angry face and attend to the neutral face, thus reducing the tendency to attend to threatening faces. The training is intended to generalize beyond faces to reduce attention to threatening stimuli in general. CBM has been tested for the treatment of a range of different psychological disorders (Beard, Sawyer, & Hofmann, 2012) and represents an exciting new direction in treatment development. However, it is important to note that in CBM, as with many novel treatments, several nonreplications followed the initial successful trials (e.g., Enock & McNally, 2013), suggesting that the jury is still out regarding the effectiveness of this new type of treatment.

In addition to new forms of treatment that can be administered in clinics, advances in technology are allowing psychologists to bring the clinic into people’s everyday lives. Psychologists are now using computers, cellular phones, and wearable biosensors to measure patients’ experiences in the real world in real time, and also to administer interventions well beyond the clinic walls (e.g., using text messages to remind patients not to smoke or to practice the skills they learned during their last therapy session). The development of “mobile health” or “mHealth” interventions has been extremely exciting; however, one recent review found that more than half of interventions that used mobile technologies fail to show any benefit (Kaplan & Stone, 2013). So although the development of portable technological devices has opened up lots of new opportunities for intervention, it is important that psychologists carefully evaluate which can help improve health outcomes and which are simply fancier ways of providing ineffective treatment.
Cognitive behavioral therapies have been found to be effective for a number of disorders (Butler et al., 2006), including unipolar depression, generalized anxiety disorder, panic disorder, social phobia, posttraumatic stress disorder, and childhood depressive and anxiety disorders (see the Hot Science box).
Group Treatments: Healing Multiple Minds at the Same Time
It is natural to think of psychopathology as an illness that affects only the individual. Yet each person lives in a world of other people, and interactions with others may intensify and even create disorders. A depressed person may be lonely after moving away from friends and loved ones, or an anxious person could be worried about pressures from parents. These ideas suggest that people might be able to recover from disorders in the same way they got into them—
Couples and Family Therapy
When a couple is “having problems,” neither individual may be suffering from any psychopathology. Rather, it may be the relationship itself that is disordered. Couples therapy is when a married, cohabitating, or dating couple is seen together in therapy to work on problems usually arising within the relationship. For example, a couple might seek help because they are unhappy with their relationship. In this scenario, both members of the couple are expected to attend therapy sessions, and the problem is seen as arising from their interaction rather than from the problems of one half of the couple. Treatment strategies would target changes in both parties, focusing on ways to break their repetitive dysfunctional pattern.
489
There are cases in which therapy with even larger groups is warranted. An individual may be having a problem—

Group Therapy
Taking these ideas one step further, if individuals (or families) can benefit from talking with a psychotherapist, perhaps they can also benefit from talking with other clients who are talking with the therapist. This is group therapy, a technique in which multiple participants (who often do not know one another at the outset) work on their individual problems in a group atmosphere. The therapist in group therapy serves more as a discussion leader than as a personal therapist, conducting the sessions both by talking with individuals and by encouraging them to talk with one another.
group therapy
A technique in which multiple participants (who often do not know one another at the outset) work on their individual problems in a group atmosphere.
Why do people choose group therapy? One advantage is that attending a group with others who have similar problems shows clients that they are not alone in their suffering. In addition, group members model appropriate behaviors for one another and share their insights about how to deal with their problems. Group therapy is often just as effective as individual therapy (e.g., Jonsson & Hougaard, 2008). So, from a societal perspective, group therapy is much more efficient.
Group therapy also has disadvantages. It may be difficult to assemble a group of individuals who have similar needs. This is particularly an issue with CBT, which tends to focus on specific problems such as depression or panic disorder. Group therapy may become a problem if one or more members undermine the treatment of other group members—
What are the pros and cons of a group therapy approach?
Self-Help and Support Groups
An important offshoot of group therapy is the concept of self-
490

In some cases, though, self-
What are the pros and cons of self-
AA has more than two million members in the United States, with 185,000 group meetings that occur around the world (Mack, Franklin, & Frances, 2003). Members are encouraged to follow “12 steps” to reach the goal of lifelong abstinence from all drinking, and the steps include believing in a higher power, practicing prayer and meditation, and making amends for harm to others. A few studies examining the effectiveness of AA have been conducted, and it appears that individuals who participate tend to overcome problem drinking with greater success than those who do not participate in AA (Fiorentine, 1999; Morgenstern et al., 1997). However, several tenets of the AA philosophy are not supported by the research. We know that the general AA program is useful, but questions about which parts of this program are most helpful have yet to be studied.
Considered together, the many social approaches to psychotherapy reveal how important interpersonal relationships are for each of us. It may not always be clear how psychotherapy works, whether one approach is better than another, or what particular theory should be used to understand how problems have developed. What is clear, however, is that social interactions between people—
SUMMARY QUIZ [15.2]
Question 15.4
| 1. | The different psychodynamic therapies all share an emphasis on |
- the influence of the collective unconscious.
- the importance of taking responsibility for psychological problems.
- combining behavioral and cognitive approaches.
- developing insight into the unconscious sources of psychological disorders.
d.
491
Question 15.5
| 2. | Which type of therapy would likely work best for someone with an irrational fear of heights? |
- psychodynamic
- gestalt
- behavioral
- humanistic
c.
Question 15.6
| 3. | Self- |
- cognitive behavioral therapy.
- support groups.
- person-
centered therapy. - group therapy.
d.