15.3 Medical and Biological Treatments: Healing the Mind by Physically Altering the Brain
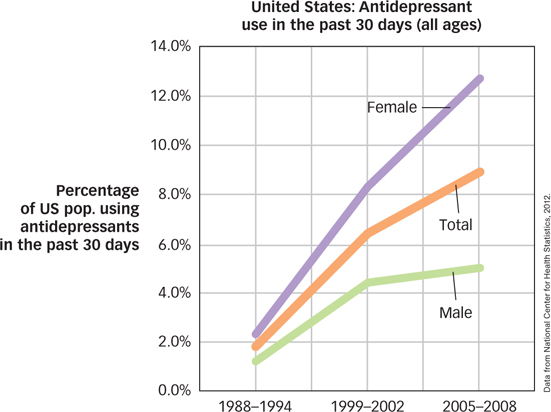
Ever since someone discovered that a whack to the head can affect the mind, people have suspected that direct brain interventions might hold the keys to a cure for psychological disorders. Archaeological evidence, for example, indicates that the occasional human thousands of years ago was “treated” for some malady by the practice of trephining (drilling a hole in the skull), perhaps in the belief that this would release evil spirits that were affecting the mind (Alt et al., 1997). Surgery for psychological disorders is a last resort nowadays, and treatments that focus on the brain usually involve interventions that are less dramatic. The use of drugs to influence the brain was also discovered in prehistory (alcohol, for example, has been around for a long time). Since then, drug treatments have grown in variety, effectiveness, and popularity, and they are now the most common medical approach in treating psychological disorders (see FIGURE 15.2).
492
Antipsychotic Medications
Antipsychotic drugs are medications that are used to treat schizophrenia and related psychotic disorders. The first antipsychotic drug, back in the 1950s, was chlorpromazine (brand name Thorazine), which was originally developed as a sedative. Other related medications, such as thioridazine (Mellaril) and haloperidol (Haldol), followed. Before the introduction of antipsychotic drugs, people with schizophrenia often exhibited bizarre symptoms and were sometimes so disruptive and difficult to manage that the only way to protect them (and other people) was to keep them in hospitals for people with mental disorders, which were initially called asylums but now are referred to as psychiatric hospitals. In the period following the introduction of these drugs, the number of people in psychiatric hospitals decreased by more than two thirds. Antipsychotic drugs made possible the deinstitutionalization of hundreds of thousands of people and gave a major boost to the field of psychopharmacology, the study of drug effects on psychological states and symptoms.
antipsychotic drugs
Medications that are used to treat schizophrenia and related psychotic disorders.
psychopharmacology
The study of drug effects on psychological states and symptoms.
Antipsychotic medications are believed to block dopamine receptors. As you read in the Psychological Disorders chapter, the effectiveness of schizophrenia medications led to the dopamine hypothesis, suggesting that schizophrenia may be caused by excess dopamine in the brain. Research has indeed found that dopamine overactivity in some areas of the brain is related to the more bizarre positive symptoms of schizophrenia, such as hallucinations and delusions (Marangell et al., 2003). Unfortunately, the negative symptoms of schizophrenia, such as emotional numbing and social withdrawal, may be related to dopamine underactivity in other areas of the brain. This may explain why antipsychotic medications do not relieve negative symptoms well.
What are the advantages of the newer, atypical antipsychotic medications?
After the introduction of antipsychotic medications, there was little change in the available treatments for schizophrenia for more than a quarter of a century. However, in the 1990s, a new class of antipsychotic drugs was introduced. These newer drugs, which include clozapine (Clozaril), risperidone (Risperdal), and olanzapine (Zyprexa), have become known as atypical antipsychotics (the older drugs are now often referred to as conventional or typical antipsychotics). Unlike the older antipsychotic medications, these newer drugs appear to block both dopamine and serotonin receptors. Serotonin has been implicated in some of the core difficulties in schizophrenia, such as cognitive and perceptual disruptions, as well as mood disturbances, which may explain why atypical antipsychotics can provide relief for both the positive and negative symptoms of schizophrenia (Bradford, Stroup, & Lieberman, 2002).
Like most medications, antipsychotic drugs have side effects. These can include motor disturbances such as involuntary movements of the face, mouth, and extremities. In fact, people often need to take another medication to treat the unwanted side effects of the conventional antipsychotic drugs. Side effects of the newer medications tend to be different and sometimes milder than those of the older antipsychotics. For that reason, the atypical antipsychotics are now usually the front-
Antianxiety Medications
Antianxiety medications are drugs that help reduce a person’s experience of fear or anxiety. The most commonly used antianxiety medications are the benzodiazepines, a type of tranquilizer that works by facilitating the action of the neurotransmitter gamma-
antianxiety medications
Drugs that help reduce a person’s experience of fear or anxiety.
493
What are some reasons for caution when prescribing antianxiety medications?
Nonetheless, these days, doctors are relatively cautious when prescribing benzodiazepines. One concern is that these drugs can be highly addictive. They also have side effects, especially drowsiness, but also negative effects on coordination and memory. And benzodiazepines combined with alcohol can depress respiration, potentially causing accidental death.
Antidepressants and Mood Stabilizers
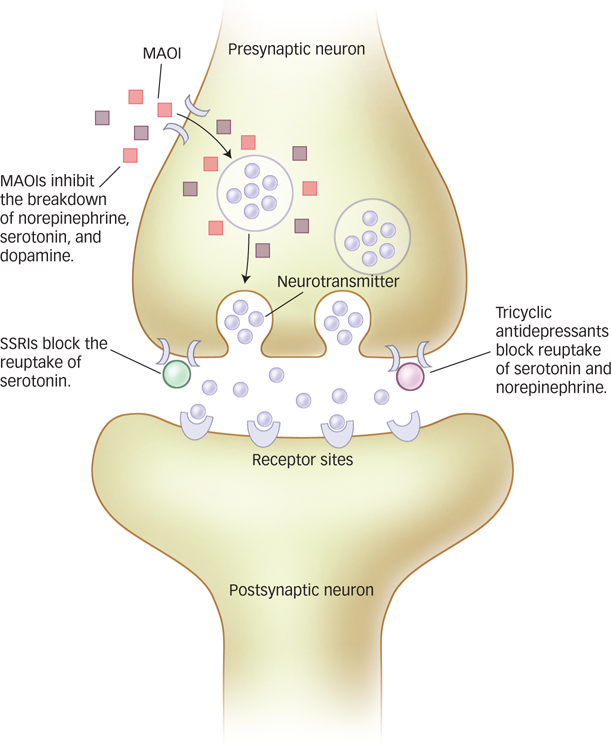
Antidepressants are a class of drugs that help lift people’s moods. Two classes of antidepressants were introduced in the 1950s, the monoamine oxidase inhibitors (MAOIs) and the tricyclic antidepressants. MAOIs prevent the enzyme monoamine oxidase from breaking down neurotransmitters such as norepinephrine, serotonin, and dopamine. However, despite their effectiveness, MAOIs are rarely prescribed anymore due to side effects such as dizziness and loss of sexual interest, as well as potentially dangerous interactions with other common medications. Tricyclic antidepressants are still sometimes used, but they also have serious side effects, including dry mouth, constipation, difficulty urinating, blurred vision, and racing heart (Marangell et al., 2003).
antidepressants
A class of drugs that help lift people’s moods.

Today, the most commonly used antidepressants are the selective serotonin reuptake inhibitors, or SSRIs, which include drugs such as fluoxetine (Prozac), citalopram (Celexa), and paroxetine (Paxil). The SSRIs work by blocking the reuptake of serotonin in the brain, which makes more serotonin available in the synaptic space between neurons. The greater availability of serotonin in the synapse gives the neuron a better chance of “recognizing” and using this neurotransmitter in sending the desired signal. The SSRIs were developed based on hypotheses that low levels of serotonin are a causal factor in depression. Supporting this hypothesis, SSRIs are effective for depression, as well as for a wide range of other problems. SSRIs are called selective because, unlike the tricyclic antidepressants, which work on the serotonin and norepinephrine systems, SSRIs work more specifically on the serotonin system (see FIGURE 15.3).
What are the most common antidepressants used today? How do they work?
Finally, antidepressants such as Effexor (venlafaxine) and Wellbutrin (ibupropion) offer other alternatives. Effexor is an example of a serotonin and norepinephrine reuptake inhibitor (SNRI), whereas SSRIs act only upon serotonin, SNRIs act on both serotonin and norepinephrine. Wellbutrin, in contrast, is a norepinephrine and dopamine reuptake inhibitor. These and other newly developed antidepressants appear to have fewer (or at least different) side effects than the tricyclic antidepressants and MAOIs.
Most antidepressants can take up to a month before they start to have an effect on mood. Besides relieving symptoms of depression, almost all of the antidepressants effectively treat anxiety disorders, and many of them can resolve other problems, such as eating disorders. In fact, several companies that manufacture SSRIs have marketed their drugs as treatments for anxiety disorders rather than for their antidepressant effects. Although antidepressants can be effective in treating major depression, they are not recommended for treating bipolar disorder because, in the process of lifting one’s mood, they might actually trigger a manic episode in a person with bipolar disorder. Instead, bipolar disorder is commonly treated with mood stabilizers, which are medications used to suppress swings between mania and depression. Commonly used mood stabilizers include lithium and valproate.
494
Herbal and Natural Products
In a survey of more than 2,000 Americans, 7% of those suffering from anxiety disorders and 9% of those suffering from severe depression reported using alternative “medications” such as herbal medicines, megavitamins, homeopathic remedies, or naturopathic remedies to treat these problems (Kessler et al., 2001). Major reasons people use these products are that they are easily available over the counter, are less expensive, and are perceived as “natural” alternatives to synthetic or manmade “drugs.” Are herbal and natural products effective in treating mental health problems, or are they just “snake oil?”
The answer to this question isn’t simple. Herbal products are not considered medications by regulatory agencies like the U.S. Food and Drug Administration, so they are exempt from rigorous research to establish their safety and effectiveness. Instead, herbal products are classified as nutritional supplements and regulated in the same way as food. There is little scientific information about herbal products, including possible interactions with other medications, possible tolerance and withdrawal symptoms, side effects, appropriate dosages, how they work, or even whether they work—
495
Why are herbal remedies used? Are they actually effective?
There is research support for the effectiveness of some herbal and natural products, but the evidence is not overwhelming (Lake, 2009). For example, some studies have shown that St. John’s wort (a wort, it turns out, is an herb) has an advantage over a placebo condition for the treatment of depression (e.g., Lecrubier et al., 2002), whereas other studies show no advantage (e.g., Hypericum Depression Trial Study Group, 2002). Omega-
Combining Medication and Psychotherapy
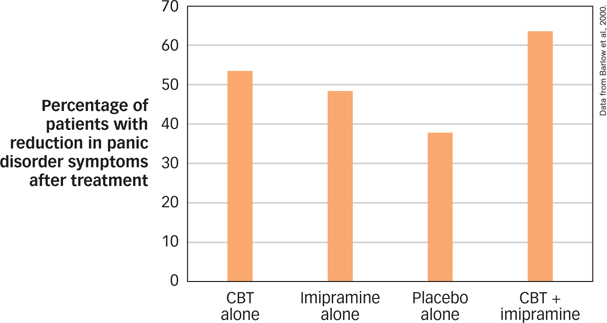
Given that psychological treatments and medications both have shown an ability to treat mental disorders effectively, some natural next questions are: Which is more effective? Is the combination of psychological and medicinal treatments better than either by itself? The answer often depends on the particular problem being considered. For example, in the cases of schizophrenia and bipolar disorder, researchers have found that medication is more effective than psychological treatment and so is considered a necessary part of treatment. But in the case of mood and anxiety disorders, medication and psychological treatments are equally effective. One study compared cognitive behavior therapy, imipramine (an antidepressant), and the combination of these treatments (CBT plus imipramine) with a placebo (administration of an inert medication) for the treatment of panic disorder (Barlow et al., 2000). After 12 weeks of treatment, either CBT alone or imipramine alone was found to be superior to a placebo. But the combination of CBT plus imipramine was not significantly better than that for either CBT or imipramine alone. In other words, either treatment was better than nothing, but the combination of treatments was not significantly more effective than one or the other (see FIGURE 15.5). More is not always better.
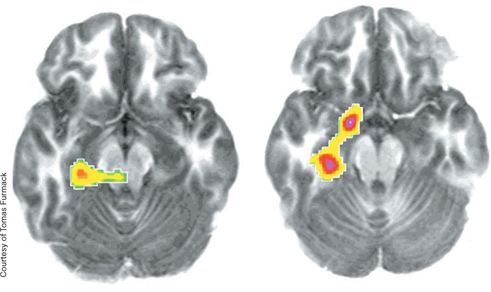
Given that both therapy and medications are effective, one question is whether they work through similar mechanisms. A study of people with social phobia examined patterns of cerebral blood flow following treatment using either citalopram (an SSRI) or CBT (Furmark et al., 2002). Participants in both groups were alerted to the possibility that they would soon have to speak in public. In both groups, those who responded to treatment showed similar reductions in activation in the amygdala, hippocampus, and neighboring cortical areas during neighboring cortical areas during this challenge (see FIGURE 15.6). The amygdala, located next to the hippocampus (see FIGURE 6.18) plays a significant role in memory for emotional information. These findings suggest that both therapy and medication affect the brain in regions associated with a reaction to threat.
496
Do therapy and medications work through similar mechanisms?
One complication in combining medication and psychotherapy is that these treatments are often provided by different people. Psychiatrists are trained in the administration of medication in medical school (and they may also provide psychological treatment), whereas psychologists provide psychological treatment but cannot prescribe medication. This means that the coordination of treatment often requires cooperation between psychologists and psychiatrists.
The question of whether psychologists should be licensed to prescribe medications has been a source of debate (Fox et al., 2009). Only Illinois, Louisiana, and New Mexico currently allow licensed and specially trained psychologists prescription privileges, but other states are considering it (Munsey, 2008). Opponents argue that psychologists do not have the medical training to understand how medications interact with other drugs. Proponents argue that patient safety would not be compromised as long as rigorous training procedures were established. At present, the coordination of medication and psychological treatment usually involves a team effort of psychiatry and psychology.
Biological Treatments beyond Medications
Medication can be an effective biological treatment, but for some people, medications do not work or side effects are intolerable. If this group of people doesn’t respond to psychotherapy either, what other options do they have to achieve symptom relief? Some additional avenues of help are available, but some are risky or poorly understood.

Electroconvulsive therapy (ECT), sometimes referred to as shock therapy, is a treatment that involves inducing a brief seizure by delivering an electrical shock to the brain. The shock is applied to the person’s scalp for less than a second. ECT is primarily used to treat severe depression that has not responded to antidepressant medications, although it may also be useful for treating bipolar disorder (Khalid et al., 2008; Poon et al., 2012). Patients are pretreated with muscle relaxants and are under general anesthesia so they are not conscious of the procedure. The main side effect of ECT is impaired short-
electroconvulsive therapy (ECT)
A treatment that involves inducing a brief seizure by delivering an electrical shock to the brain.
Transcranial magnetic stimulation (TMS) is a treatment that involves placing a powerful pulsed magnet over a person’s scalp, which alters neuronal activity in the brain (see the Neuroscience and Behavior chapter). Unlike ECT, TMS is noninvasive, and side effects are minimal: They include mild headaches and a small risk of seizure, but TMS has no impact on memory or concentration. TMS may be particularly useful in treating depression that is unresponsive to medication (Avery et al., 2009). In fact, a study comparing TMS to ECT found that both procedures were effective, with no significant differences between them (Janicak et al., 2002). Other studies have found that TMS can also be used to treat auditory hallucinations in schizophrenia (Aleman, Sommer, & Kahn, 2007).
transcranial magnetic stimulation (TMS)
A treatment that involves placing a powerful pulsed magnet over a person’s scalp, which alters neuronal activity in the brain.
497
Other Voices: Diagnosis: Human
Diagnosis: Human

Should more people receive psychological treatment or medications? Or should fewer? On one hand, data indicate that most people with a mental disorder do not receive treatment and that untreated mental disorders are an enormous source of pain and suffering. On the other hand, some argue that we have become too quick to label normal human behavior as “disordered” and too willing to medicate any behavior, thought, or feeling that makes us uncomfortable. Ted Gup is one of these people. The following is a version of his op-
The news that 11 percent of school-
In his case, he was in the first grade. Indeed, there were psychiatrists who prescribed medication for him even before they met him. One psychiatrist said he would not even see him until he was medicated. For a year I refused to fill the prescription at the pharmacy. Finally, I relented. And so David went on Ritalin, then Adderall, and other drugs that were said to be helpful in combating the condition.
In another age, David might have been called “rambunctious.” His battery was a little too large for his body. And so he would leap over the couch, spring to reach the ceiling and show an exuberance for life that came in brilliant microbursts.
As a 21-
I had unknowingly colluded with a system that devalues talking therapy and rushes to medicate, inadvertently sending a message that self-
My son was no angel (though he was to us) and he was known to trade in Adderall, to create a submarket in the drug among his classmates who were themselves all too eager to get their hands on it. What he did cannot be excused, but it should be understood. What he did was to create a market that perfectly mirrored the society in which he grew up, a culture where Big Pharma itself prospers from the off-
And so a generation of students, raised in an environment that encourages medication, are emulating the professionals by using drugs in the classroom as performance enhancers. And we wonder why it is that they use drugs with such abandon. As all parents learn—
The issue of permissive drug use and over-
One of the new, more controversial provisions expands depression to include some forms of grief. On its face it makes sense. The grieving often display all the common indicators of depression—
Ours is an age in which the airwaves and media are one large drug emporium that claims to fix everything from sleep to sex. I fear that being human is itself fast becoming a condition. It’s as if we are trying to contain grief, and the absolute pain of a loss like mine. We have become increasingly disassociated and estranged from the patterns of life and death, uncomfortable with the messiness of our own humanity, aging and, ultimately, mortality.
Challenge and hardship have become pathologized and monetized. Instead of enhancing our coping skills, we undermine them and seek shortcuts where there are none, eroding the resilience upon which each of us, at some point in our lives, must rely. Diagnosing grief as a part of depression runs the very real risk of delegitimizing that which is most human—
The DSM would do well to recognize that a broken heart is not a medical condition, and that medication is ill-
But there is a sweetness even to the intensity of this pain I feel. It is the thing that holds me still to my son. And yes, there is a balm even in the pain. I shall let it go when it is time, without reference to the DSM, and without the aid of a pill.
Have we gone too far in labeling and treatment of mental disorders? Or have we not gone far enough? How can we make sure that we are not medicating normal behavior, while at the same time ensuring that we provide help to those who are suffering with a true mental disorder?
From the New York Times, April 3, 2013 © 2013 The New York Times. All rights reserved. Used by permission and protected by the Copyright Laws of the United States. The printing, copying, redistribution, or retransmission of this Content without express written permission is prohibited. http:/
498

Phototherapy, a therapy that involves repeated exposure to bright light, may be helpful to people who have a seasonal pattern to their depression. This could include people suffering from seasonal affective disorder (SAD; see the Psychological Disorders chapter). Typically, people are exposed to bright light in the morning, using a lamp designed for this purpose. Phototherapy has not been as well researched as psychological treatment or medication, but the handful of studies available suggest it is approximately as effective as antidepressant medication in the treatment of SAD (Thaler et al., 2011).
phototherapy
A therapy that involves repeated exposure to bright light.
In very rare cases, psychosurgery, the surgical destruction of specific brain areas, may be used to treat psychological disorders. Psychosurgery has a controversial history, beginning in the 1930s with the invention of the lobotomy by Portuguese physician Egas Moniz (1874–
psychosurgery
Surgical destruction of specific brain areas.
Today, psychosurgery is reserved only for extremely severe cases for which both no other interventions have been effective and the symptoms of the disorder are intolerable to the patient. Modern psychosurgery involves a very precise destruction of brain tissue in order to disrupt the brain circuits known to be involved in the generation of symptoms. For example, people suffering from OCD who fail to respond to treatment (including several trials of medications and cognitive behavioral treatment) may benefit from specific surgical procedures to destroy part of the corpus callosum (see FIGURE 3.16) and cingulate gyrus (the ridge just above the corpus collosum), two brain areas known to be involved in the generation of obsessions and compulsions. Because of the relatively small number of cases of psychosurgery, there are not as many studies of these techniques as there are for other treatments; however, available studies have shown that psychosurgery typically leads to substantial improvements in both the short and long term for people with severe OCD (Csigó et al., 2010; van Vliet et al., 2013).
Where do people turn if psychological treatment and medication are unsuccessful?
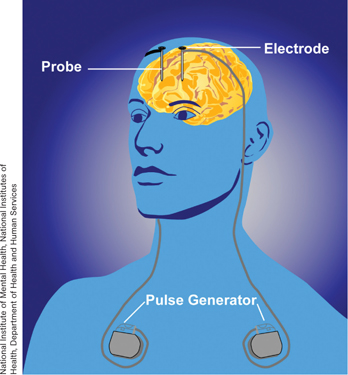
A final approach, called deep brain stimulation (DBS), combines the use of psychosurgery with the use of electric currents (as in ECT and TMS). In DBS, a treatment pioneered only recently, a small, battery-
499
SUMMARY QUIZ [15.3]
Question 15.7
| 1. | Antipsychotic drugs are used to treat |
- depression.
- schizophrenia.
- anxiety.
- mood disorders.
b.
Question 15.8
| 2. | Which of the following statements is NOT accurate regarding antidepressants? |
- Current antidepressants act on combinations of different neurotransmitter systems.
- Antidepressants have had significantly positive results in the treatment of bipolar disorder.
- Antidepressants are also prescribed to treat anxiety.
- Most antidepressants can take up to a month before they start to have an effect on mood.
b.
Question 15.9
| 3. | What do electroconvulsive therapy, transcranial magnetic stimulation, and phototherapy all have in common? |
- They incorporate herbal remedies in their treatment regimens.
- They may result in the surgical destruction of certain brain areas.
- They are considered biological treatments beyond medication.
- They are typically used in conjunction with psychotherapy.
c.