2.5 The Hemispheres
THE GIRL WITH HALF A BRAIN
 As Brandon Burns began his long journey to recovery, a 17-year-old girl in Bristol, Pennsylvania, was enjoying a particularly successful senior year of high school. Christina Santhouse was an honor roll student for the fourth year in a row, and she had been named captain of the varsity bowling team. But these accomplishments did not come so easily. It took Christina twice as much time as classmates to do homework assignments and projects because her brain needed extra time to process information. She had to invent a new bowling technique to use in games because the left side of her body was partially paralyzed, and she was constantly aware of being “different” from the other kids at school. Christina wasn’t simply different from her classmates, however. She was extraordinary because she managed to do everything her classmates did (and more) with nearly half of her brain missing.
As Brandon Burns began his long journey to recovery, a 17-year-old girl in Bristol, Pennsylvania, was enjoying a particularly successful senior year of high school. Christina Santhouse was an honor roll student for the fourth year in a row, and she had been named captain of the varsity bowling team. But these accomplishments did not come so easily. It took Christina twice as much time as classmates to do homework assignments and projects because her brain needed extra time to process information. She had to invent a new bowling technique to use in games because the left side of her body was partially paralyzed, and she was constantly aware of being “different” from the other kids at school. Christina wasn’t simply different from her classmates, however. She was extraordinary because she managed to do everything her classmates did (and more) with nearly half of her brain missing.

Christina’s remarkable story began when she was 7 years old. She was a vibrant, healthy child who loved soccer and playing outside with her friends. Barring an occasional ear infection, she basically never got sick—that is, until the day she suffered her first seizure. It was the summer of 1995 and Christina’s family was vacationing on the Jersey Shore. While playing in a swimming pool with her cousins, Christina hopped onto the deck to chase a ball. At that moment, she noticed that something wasn’t quite right. She looked down and saw her left ankle twitching uncontrollably. Her life was about to change dramatically.
Christina continued to experience tremors in her ankle. As the days and weeks wore on, those tremors moved up her left side and eventually spread throughout her body. In time, she was having seizures every 3 to 5 minutes. Christina was evaluated by various doctors, who suspected she had Rasmussen’s encephalitis, a rare disease that causes severe swelling in one side of the brain, impairing movement and thinking and causing seizures that come as often as every few minutes (National Institute of Neurological Disorders and Stroke, 2011b). As one doctor put it, “The disease eats away at your brain like a Pac-Man.”
Christina and her mother decided to seek treatment at The Johns Hopkins Hospital in Baltimore, the premiere center for children with seizure disorders. They met with Dr. John Freeman, a pediatric neurologist and an expert in hemispherectomy, a surgery to remove nearly half of the brain. A rare and last-resort operation, the hemispherectomy is only performed on patients suffering from severe seizures that can’t be controlled in other ways. After examining Christina, Dr. Freeman made the same diagnosis of her condition—Rasmussen’s encephalitis—and indicated that the seizures would get worse, and they would get worse fast. He recommended a hemispherectomy and told Christina (and her mother) to let him know when she had reached her limit with the seizures. Then they would go ahead with the operation.
Why did Dr. Freeman recommend this drastic surgery to remove nearly half of Christina’s brain? And what side of the brain did he suggest removing? Before addressing these important questions, we need to develop a general sense of the brain’s geography.
Christina, in her own words:
Right Brain, Left Brain: The Two Hemispheres
LO 8 Describe the functions of the two brain hemispheres and how they communicate.
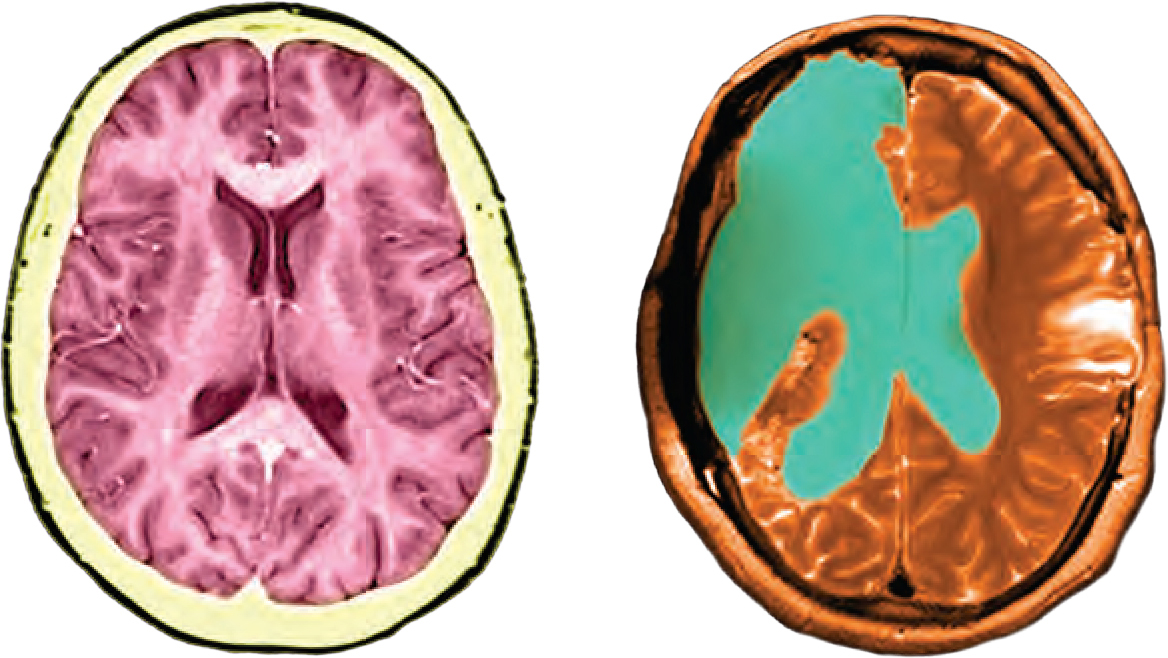
If you look at a photo or an illustration of the brain, you will see a walnut-shaped wrinkled structure—this is the cerebrum (Latin for “brain”), the largest and most conspicuous part of the brain. The cerebrum includes virtually all parts of the brain except the brainstem structures, which you will learn about later. Like a pecan or walnut, the cerebrum has two distinct halves, or hemispheres. Looking at the brain from above, you can see a deep groove running from the front of the head to the back, dividing it into the right cerebral hemisphere and the left cerebral hemisphere. Although the hemispheres look like mirror images of one another, with similar structures on the left and right, they do not have identical jobs nor are they perfectly symmetrical. Generally speaking, the right hemisphere controls the left side of the body, and the left hemisphere controls the right. This explains why Brandon, who was shot on the left side of his head, suffered paralysis and loss of sensation on the right half of his body. Christina’s situation is roughly the opposite. Rasmussen’s encephalitis struck the right side of her brain, which explains why her left ankle started twitching at the pool and why all of her subsequent seizures affected the left side of her body. Thus, it might come as no surprise that Dr. Freeman recommended the removal of the right hemisphere of her brain.
CHRISTINA MAKES THE DECISION
 Within 2 months, Christina’s seizures were occurring every 3 minutes, hundreds of times a day. She was unable to play soccer or go outside during school recess, and she sat on a beanbag chair in class so she wouldn’t hurt herself when overcome with a seizure. “I couldn’t do anything anymore,” Christina says. “I wasn’t enjoying my life.” In February 1996 the doctors at Johns Hopkins removed the right hemisphere of Christina’s brain. The operation lasted some 14 hours.
Within 2 months, Christina’s seizures were occurring every 3 minutes, hundreds of times a day. She was unable to play soccer or go outside during school recess, and she sat on a beanbag chair in class so she wouldn’t hurt herself when overcome with a seizure. “I couldn’t do anything anymore,” Christina says. “I wasn’t enjoying my life.” In February 1996 the doctors at Johns Hopkins removed the right hemisphere of Christina’s brain. The operation lasted some 14 hours.
When Christina emerged from the marathon surgery, her head was pounding with pain. “I remember screaming and asking for medicine,” she recalls. The migraines persisted for months but eventually tapered off, and ultimately the surgery served its purpose: Christina no longer experienced debilitating seizures.
Split Brain
LO 9 Explain lateralization and how split-brain operations affect it.

Removing nearly half of a brain may sound barbaric, but hemispherectomies have proven to be effective for eliminating and reducing seizures. In a study of the 111 children who had hemispherectomies at Johns Hopkins between 1975 and 2001, 65% no longer suffered seizures at all, and 21% experienced infrequent, “nonhandicapping” seizures. The remaining 14% still had seizures described as “troublesome” (Kossoff et al., 2003).
Christina: How does your condition affect your confidence and social life?
Hemispherectomies are exceptionally rare, used only when seizures occur many times a day, cannot be tempered with drugs, and stem from problems in one hemisphere (Choi, 2007, May 24). A less extreme, last-resort surgery for drug-resistant seizures is the split-brain operation, which essentially disconnects the right and left hemispheres. Normally, the two hemispheres are linked by a bundle of nerve fibers known as the corpus callosum  . Through the corpus callosum, the left and right sides of the brain communicate and work together to process information. But this same band of nerve fibers can also serve as a passageway for the electrical storms responsible for seizures. With the split-brain operation, the corpus callosum is severed so that these storms can no longer pass freely between the hemispheres (Wolman, 2012, March 15).
. Through the corpus callosum, the left and right sides of the brain communicate and work together to process information. But this same band of nerve fibers can also serve as a passageway for the electrical storms responsible for seizures. With the split-brain operation, the corpus callosum is severed so that these storms can no longer pass freely between the hemispheres (Wolman, 2012, March 15).
Specialization and the Split-Brain Operation
In addition to helping many patients with severe, drug-resistant epilepsy (Abou-Khalil, 2010), the consequences of split-brain operations have provided researchers with an excellent opportunity to explore the specialization of the hemispheres. Before we start to look at this research, you need to understand how visual information is processed. Each eye receives visual sensations, but that information is sent to the opposite hemisphere, and shared between the hemispheres via the corpus callosum (Chapter 3). Specifically, information presented in the right visual field is processed in the left hemisphere, and information presented in the left visual field is processed in the right hemisphere.
Equipped with this knowledge, American neuropsychologist Roger Sperry (1913–1994) and his student Michael Gazzaniga (1939–) conducted groundbreaking research on epilepsy patients who had undergone split-brain operations to alleviate their seizures. (This research ultimately led to Sperry’s 1981 Nobel Prize in Physiology or Medicine.) Not only did Sperry and Gazzaniga’s “split-brain” participants experience fewer seizures, they had surprisingly normal cognitive abilities and showed no obvious changes in “temperament, personality, or general intelligence” as a result of their surgeries (Gazzaniga, 1967, p. 24). But under certain circumstances, the researchers observed, they behaved as though they had two separate brains (Gazzaniga, 1967, 1998; Figure 2.7). Because the hemispheres were disconnected, the researchers could study each hemisphere separately to explore its own unique capabilities (or “specializations”).
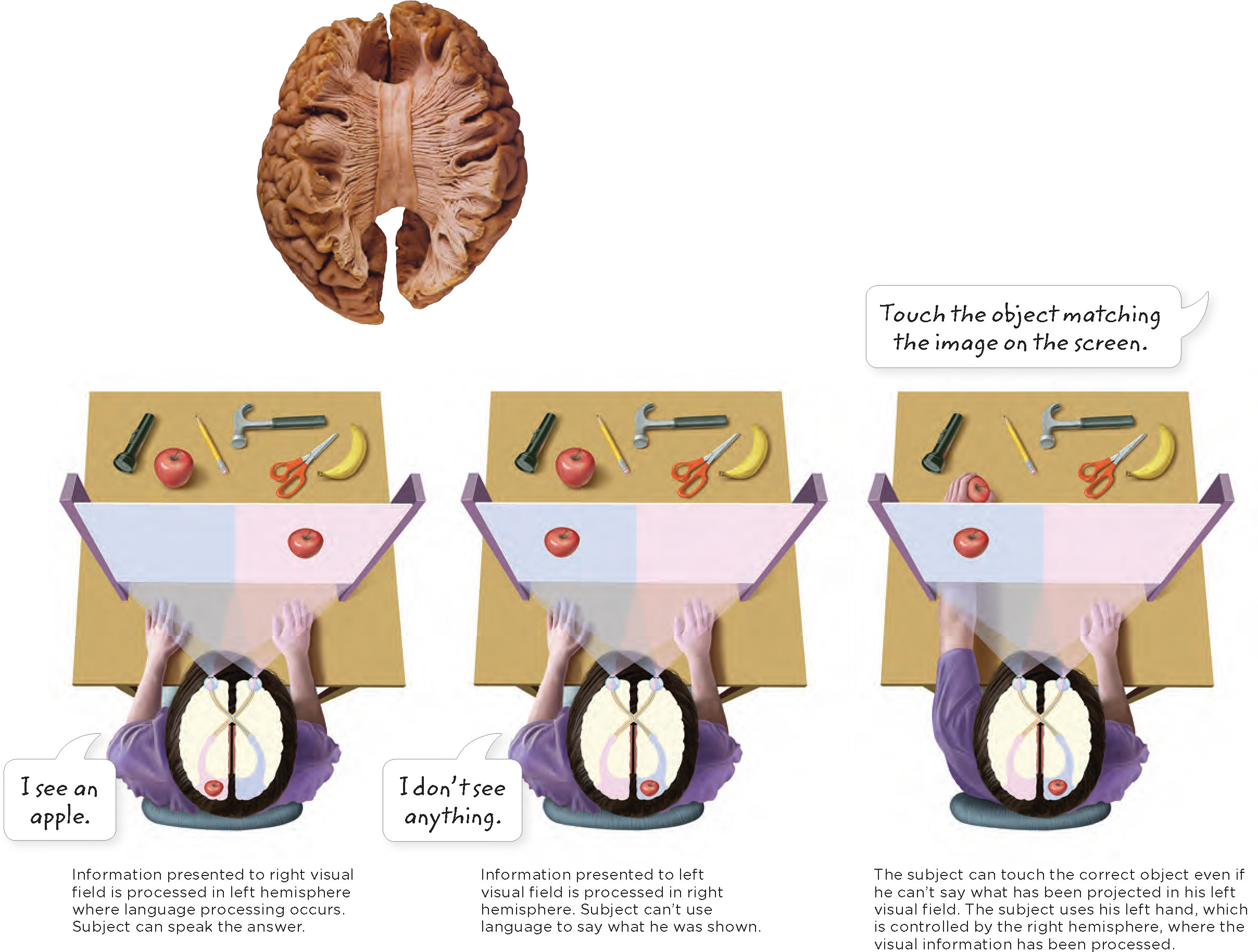
Imagine that the researchers flashed an image (let’s say an apple) on the right side of a screen, ensuring that it would be processed by the brain’s left hemisphere. The split-brain participant could articulate what she had seen (“I saw an apple”). If, however, the apple appeared on the left side of the screen (processed by the right hemisphere), she would claim she saw nothing. But when asked to identify the image in a nonverbal way (pointing or touching with her left hand), she could do this without a problem (Gazzaniga, 1967, 1998). These findings are extremely useful in understanding the capabilities of the left and right hemispheres.

Lateralization
The split-brain experiments offered an elegant demonstration of lateralization, the tendency for the left and right hemispheres to excel in certain activities. When images are flashed in the right visual field, the information is sent to the left side of the brain, which excels in language processing. This explains why the split-brain participants were able to articulate the image they had seen on the right side of the screen. Images appearing in the left visual field are sent to the right side of the brain, which is generally not responsible for processing language but instead excels at visual spatial tasks. This is why the participants were tongue tied when asked to report what they had seen on the left side of the screen. They could, however, reach out and point to it. What hand do you think they used? The image was flashed in the left visual field and the sensory information was sent to the right hemisphere, which is unable to put into words what was seen. The left hand, which is controlled by the right hemisphere, pointed to the object (Gazzaniga, 1998; Gazzaniga, Bogen, & Sperry, 1965). The bottom line: The left hemisphere plays a crucial role in language processing and the right hemisphere plays a crucial role in managing visual spatial tasks.
This is only a generalization, however. While there are clear differences in the way the hemispheres process information (and the speed at which they do it), they can also process the same types of information. In a split-brain patient, communication between the hemispheres is limited. This is not the case for someone with an intact corpus callosum. Regardless of the type of information coming in or being processed, our hemispheres are constantly integrating and sharing information (Lilienfeld, Lynn, Ruscio, & Beyerstein, 2011). Next time you hear someone claim that some people are more “left-brained” or “right-brained,” ask him to identify the research that backs up such a claim. Similarly, beware of catchy sales pitches for products designed to increase your “logical and analytical” left-brain thinking or to help you tap into the “creative” side of your right brain. This way of thinking is oversimplified.
Keep this in mind while reading the upcoming sections on specialization in the left and right sides of the brain. The two hemispheres may each have certain areas of expertise, but they work as a team to create your experience of the world.
Language and the Left
Armed with this new knowledge of the split-brain experiments, let’s return our focus to Brandon. Brandon’s injury occurred on the left side of his brain, devastating his ability to use language. Before the battle of Fallujah, he had breezed through western novels at breakneck speeds. After his injury, even the simplest sentence baffled him. Words on a page looked like nothing more than black lines and curls. Brandon remembers, “It was like a puzzle that I couldn’t figure out.”
Handedness and Language Dominance

Brandon’s difficulties language are fairly typical for someone with a brain injury to the left hemisphere, because regions on the left side of the brain tend to predominate in language. This is not true for everyone, however. In a study examining handedness and language dominance, researchers administered a test to participants to determine degree of handedness (righty or lefty) and used brain scan technology to determine their predominant side for language processing. They found that around 27% of strongly left-handed participants and 4% of strongly right-handed participants had language dominance in the right hemisphere (Knecht et al., 2000). What does this mean? The left hemisphere controls language in most but not all people, and it doesn’t necessarily correspond to right- or left-handedness.
Broca’s Area
LO 10 Identify areas in the brain responsible for language production and comprehension.
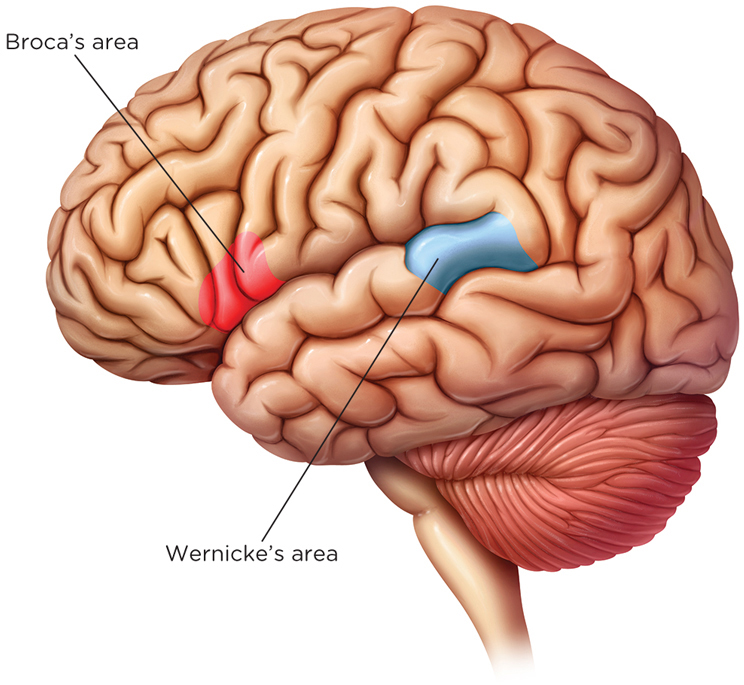
Evidence for the “language on the left” trend appeared as early as 1861, when a French surgeon by the name of Pierre Paul Broca (1824–1880) encountered two patients who had, for all practical purposes, lost the ability to talk. One of the patients could only say the word “tan,” and the other had an oral vocabulary of only five words. When Broca later performed autopsies on the men, he found that both had sustained damage to the same area on the side of the left frontal lobe (right around the temple; Figure 2.8). Over the years, Broca identified several other speech-impaired patients with damage to the same area, a region now called Broca’s area (brō-kəz) (Greenblatt, Dagi, & Epstein, 1997), which is involved in speech production.
Wernicke’s Area
Around the same time Broca was doing his-research, a German doctor named Karl Wernicke (1848–1905) pinpointed a different place in the left hemisphere that seemed to control speech comprehension. Wernicke noticed that patients suffering damage to a small tract of tissue in the left temporal lobe, now called Wernicke’s area (ver-nə-kəz), struggled to make sense of what others were saying. Wernicke’s area is the brain’s headquarters for language comprehension. Broca’s and Wernicke’s work, along with other early findings, highlighted the left hemisphere’s critical role in language. Scientists initially suspected that Broca’s area was responsible for speech creation and Wernicke’s area for comprehension, but it is now clear the use of language is far more complicated. These areas may perform additional functions, such as processing music and interpreting hand gestures (Koelsch et al., 2002; Xu, Gannon, Emmorey, Smith, & Braun, 2009), and they cooperate with multiple brain regions to allow us to produce and understand language. Furthermore, some speech processing appears to occur in the right hemisphere.
The Role of the Right
Research involving two split-brain patients suggests the right hemisphere is more proficient than the left in some visual tasks (Corballis, 2003), such as determining whether two objects are identical as opposed to mirror images of one another (Funnell, Corballis, & Gazzaniga, 1999), or judging if lines are oriented in the same direction (Corballis, Funnell, & Gazzaniga, 2002). Other findings suggest the right hemisphere is crucial for understanding abstract and humorous use of language (Coulson & Van Petten, 2007); somewhat better than the left for following conversations that change topic (Dapretto, Lee, & Caplan, 2005); and important for our ability to recognize faces (Kanwisher, McDermott, & Chun, 1997).
show what you know
Question 2.12
1. The left hemisphere excels in language and the right hemisphere excels in visual spatial tasks. This specialization of the two hemispheres is known as:
- split-brain.
- callosotomy.
- hemispherectomy.
- lateralization.
d. lateralization.
Question 2.13
2. A man involved in a car accident suffered severe brain trauma. As he recovered, it became clear he was having difficulty producing speech, even though he could understand what people were saying to him. It is very likely he had suffered damage to the left frontal lobe in a part of the brain referred to as:
- Wernicke’s area.
- Broca’s area.
- the visual field.
- the corpus callosum.
b. Broca’s area.
Question 2.14
3. On rare occasions, medication does not work for people with severe seizures. In those cases, doctors might suggest a procedure known as a __________, which essentially disconnects the right and left hemispheres.
split-brain operation
Question 2.15
4. The corpus callosum enables information sharing between the two hemispheres. In some cases, surgeons sever the corpus callosum to prevent seizures from spreading between the two hemispheres. How would you explain to a middle school student why this surgical procedure is used and how it is helpful?
The corpus callosum is a bundle of nerve fibers that allows the two halves of the brain to communicate and work together to process information. This same band of nerve fibers can also serve as a passageway for electrical storms responsible for seizures. With the split-brain operation, the corpus callosum is severed so that these storms can no longer pass freely between the hemispheres.