13.5 Psychotherapy: Who’s in the Mix?
LO 9 Describe how culture interacts with the therapy process.

A Canadian psychologist talks with residents of a displaced persons camp in Port-
 WHEN TO LISTEN, WHEN TO TALK One of the challenges of providing therapy in a country like the United States, where ethnic minorities comprise over a third of the population (Yen, 2012, May 17), is meeting the needs of clients from vastly different cultures. A therapist living in a diverse city like San Francisco or Houston may serve clients from multiple cultures in a single week, and each of those cultures has its own set of social norms dictating when to be quiet, when to speak, and how to express oneself.
WHEN TO LISTEN, WHEN TO TALK One of the challenges of providing therapy in a country like the United States, where ethnic minorities comprise over a third of the population (Yen, 2012, May 17), is meeting the needs of clients from vastly different cultures. A therapist living in a diverse city like San Francisco or Houston may serve clients from multiple cultures in a single week, and each of those cultures has its own set of social norms dictating when to be quiet, when to speak, and how to express oneself.
For Dr. Foster, this part of the job is relatively straightforward. All his clients are Northern Plains Indians, which means they follow similar social rules. And because Dr. Foster belongs to this culture, its norms are second nature to him. He has come to expect, for example, that a young Lakota client will not begin talking until he, the therapist, has spoken first. Dr. Foster is an elder, and elders are shown deference. Thus, to make a younger client feel more comfortable, he might begin a session by talking for 3 or 4 minutes. Once the client does open up, he limits his verbal and nonverbal feedback, sitting quietly and avoiding eye contact. In mainstream American culture, people continuously respond to each other with facial animation and filler words like “wow” and “uh-
Another facet of Lakota communication—
across the WORLD
Know Thy Client
 Clearly, it is important for a therapist to know the cultural context in which he works. But does that mean therapists and clients should be matched according to race, ethnicity, or gender? Some clients feel more -comfortable discussing private thoughts and feelings with a therapist who shares their experience—
Clearly, it is important for a therapist to know the cultural context in which he works. But does that mean therapists and clients should be matched according to race, ethnicity, or gender? Some clients feel more -comfortable discussing private thoughts and feelings with a therapist who shares their experience—
When the therapist and client do come from different worlds, it is the therapist’s job to get in touch with the client’s unique perspective. That includes being respectful of cultural norms. Western therapists working in India or sub-
Within any group, there is vast variation from one individual to the next, but cultural themes do emerge. The Sioux and Blackfeet Indians, for example, are very relationship-
SHOULD THERAPISTS AND CLIENTS BE MATCHED IN TERMS OF RACE, ETHNICITY, OR GENDER?
Immigrant populations face their own set of challenges. Men often have a difficult time adjusting to the declining social status and income that comes with moving to a new country. Women tend to fare better, adapting to the new culture and finding jobs more quickly, which can lead to tension between spouses (Prochaska & Norcross, 2014). Keep in mind that these are only general trends; assuming they apply to an entire population promotes stereotyping.
This brings us to one of the key themes of the chapter: When it comes to psychological treatment, there is no “one-
Let’s Get Through This Together
For some people, group therapy is a better fit than individual therapy. First developed in the 1940s, group therapy has adapted to the ever-

Self-
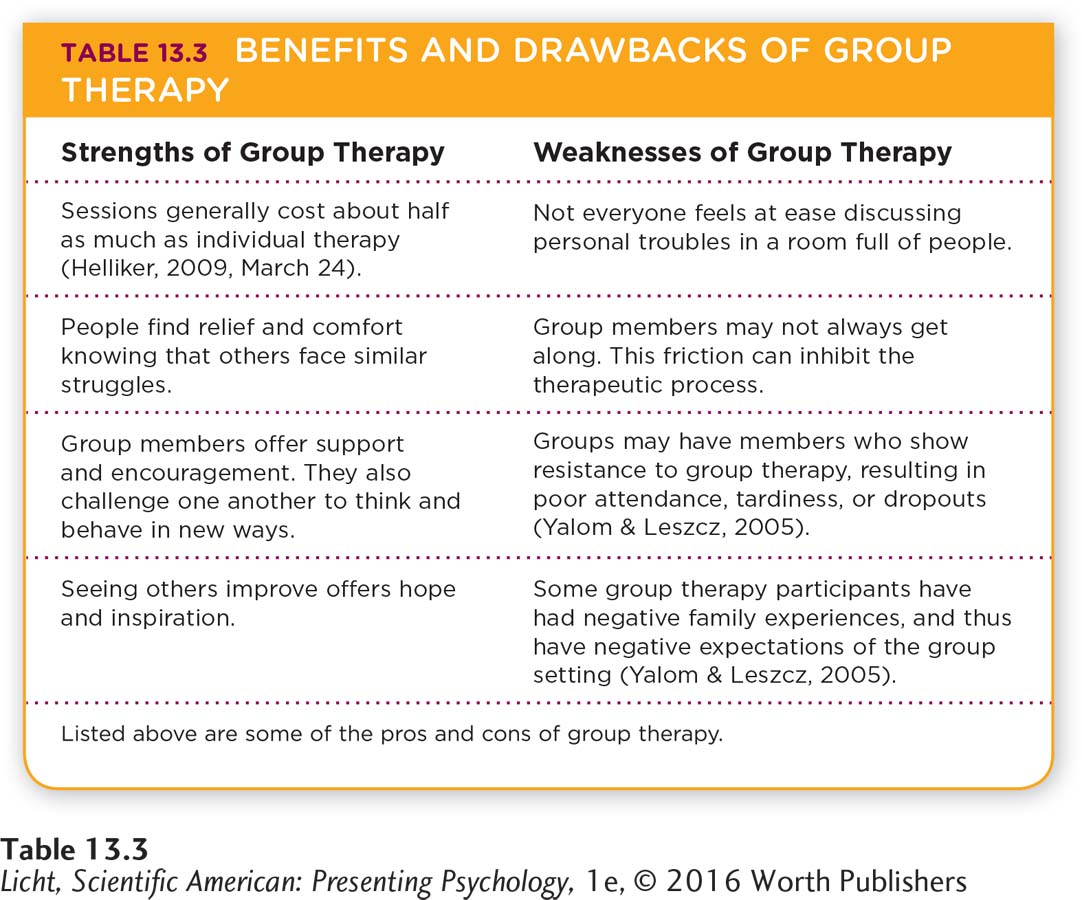
LO 10 Identify the benefits and challenges of group therapy.
GROUP THERAPY In a group therapy session, members share their problems as openly as possible, and research typically shows that group therapy is as effective as individual therapy for addressing many problems. It is actually the preferred approach for interpersonal issues, because it allows therapists to observe clients interacting with others. The therapist’s skills play an important role in the success of group sessions, and the dynamics between clients and therapists may be similar to those that arise in individual therapy. (Clients may demonstrate resistance or transference, for example.)
Synonyms
self-
family therapy family counseling
couples therapy marital therapy
SELF-
family therapy A type of therapy that focuses on the family as an integrated system, recognizing that the interactions within it can create instability or lead to the breakdown of the family unit.
FAMILY THERAPY Introduced in North America in the 1940s, family therapy focuses on the family as an integrated system, recognizing that the interactions within it can create instability or lead to the breakdown of the family unit (Corey, 2013). Family therapy explores relationship problems rather than the symptoms of particular disorders, teaching communication skills in the process. The family is viewed as a dynamic, holistic entity, and the goal is to understand each person’s role in the system, not to root out troublemakers, assign blame, or identify one member who must be “fixed.” Because families typically seek the resolution of a specific problem, the course of therapy tends to be brief (Corey, 2013). Suppose a teenage girl has become withdrawn at home and is acting out in school, and the whole family decides to participate in therapy. The therapist begins by helping the parents identify ways they encourage her behaviors (not following through with consequences, for example), and may examine how their marital dynamics affect the kids. If it becomes evident that the marriage is in trouble, the parents might seek therapy without the rest of the family, which brings us to the next topic: couples therapy.
COUPLES THERAPY Let’s face it, most couples have issues. High on the list are conflicts about money (“You are so stingy!”), failures to communicate (“You never listen!”), languishing physical bonds (“No dear, not tonight”), children, and jealousy (Storaasli & Markman, 1990). But when these problems begin to cause significant distress, couples therapy is a smart choice. Couples therapists are trained in many of the therapeutic approaches described earlier, and they tend to focus on conflict management and communication. One goal of couples therapy and relationship education programs is to provide guidance on how to communicate within relationships (Scott, Rhoades, Stanley, Allen, & Markman, 2013).
Couples therapy can yield positive results for many couples—
TAKING STOCK: AN APPRAISAL OF GROUP, FAMILY, AND COUPLES THERAPY Like any treatment, group therapy has its strengths and limitations (Table 13.3). Group members may not get along, or they may feel uncomfortable discussing sensitive issues. But conflict and discomfort are not necessarily bad when it comes to therapy (group or otherwise), because such feelings often motivate people to reevaluate how they interact with others, and perhaps try new approaches.
Evaluating group therapies can be difficult because there is so much variation in approaches (psychodynamic, cognitive behavioral, and so on). However, strong evidence exists that couples and marital therapy are effective for treating a wide range of problems (Shadish & Baldwin, 2003). The outcomes for group therapy rival those of individual therapy for many types of clients and problems (Burlingame & Baldwin, 2011; Yalom & Leszcz, 2005). As with individual therapies, the role of the group therapist is of critical importance: Empathy, good facilitation skills, listening, and careful observation are important predictors of successful outcomes. So, too, are the preparation of the group members, the therapist’s verbal style, and the “climate” and cohesion of the group (Burlingame & Baldwin, 2011).
Does Psychotherapy Work?
LO 11 Evaluate the effectiveness of psychotherapy.
Now that we have familiarized ourselves with the strengths and weaknesses of various therapeutic approaches, let’s direct our attention to overall outcomes. How effective is psychotherapy in general? This question is not easily answered, partly because therapeutic “success” is so difficult to quantify. What constitutes success in one therapy context may not be the same in another. And for therapists trying to measure the efficacy of methods they use, eliminating bias can be very challenging.
That being said, there is solid evidence suggesting that therapy usually “works,” especially if it is long-
Apply This
I THINK I NEED HELP: WHAT SHOULD I DO?
If you suspect you or someone you care about is suffering from a psychological disorder or needs support coping with a divorce, death, or major life change, do not hesitate to seek professional help. The first step is figuring out what kind of therapy fits best for the person and the situation (individual, family, group, and so on). Then there is the issue of cost: Therapy can be expensive. These days, one 60-
Many people have health insurance that helps pay for medication and psychotherapy. In 2010 the Mental Health Parity and Addiction Equity Act (MHPAEA) took effect, requiring all group health insurance plans (with 50 employees or more) to provide mental health treatment benefits as part of their plan—
The next step is finding the right therapist, that is, the right qualified therapist. Helping others manage their mental health issues is a tremendous responsibility that only licensed professionals should take on. But who exactly meets the criteria for a “qualified professional”? It depends on where you live. Different states have different licensing requirements, and because these requirements vary from state to state, we encourage you to verify the standing of a therapist’s license with your state’s Department of Regulatory Agencies. The pool of potential therapists might include clinical psychologists with PhDs or PsyDs, counseling psychologists, individuals with EdDs, psychiatrists, psychiatric nurses, social workers, marriage and family therapists, pastoral counselors, and more. (See Appendix B for more information about education and careers in psychology.) If you don’t seek psychological help from a trained and certified professional in person, you should be very cautious about seeking assistance online.![]()
Nonstandard Treatment: Self-Help and E-Therapy
Type “psychology” or “self-
LO 12 Summarize the strengths and weaknesses of online psychotherapy.
e-
With more people gaining access to the Internet and more therapists trying to specialize and make themselves marketable, online therapies are multiplying. A relative newcomer to the treatment world, e-
While we are on the topic of the Internet, we cannot resist a tie-

Mental health nurse practitioner Cassandra Donlon chats with a client via computer at the Roseburg, Oregon, Veterans Affairs Medical Center. With online technologies such as Skype and Google Hangouts, therapists can conduct sessions with clients on the opposite side of the globe.
SOCIAL MEDIA and psychology
Therapist or Friend?
 Imagine that you are the psychotherapist serving a small community college. You talk to students about their deepest fears and conflicts. They tell you about their mothers, fathers, lovers, and foes. In some respects, you know these students better than their closest friends do. But your clients are not your buddies. They are your clients. So what do you say when a client asks you to become a friend on Facebook, a contact on LinkedIn, or a follower on Instagram?
Imagine that you are the psychotherapist serving a small community college. You talk to students about their deepest fears and conflicts. They tell you about their mothers, fathers, lovers, and foes. In some respects, you know these students better than their closest friends do. But your clients are not your buddies. They are your clients. So what do you say when a client asks you to become a friend on Facebook, a contact on LinkedIn, or a follower on Instagram?
Our answer to that question is a definitive no. The relationship between therapist and client should remain a professional one, both online and offline. But that doesn’t mean that social media have no place in the mental health field. Psychologists are among the many professionals using social media to connect with colleagues and market their services to potential clients. They may be avid Twitter users, tweeting their latest musings about current events and everyday life. Social media may even come in handy for therapy itself, as when a client with public speaking anxiety shows his therapist a video of himself giving a speech (Kolmes, 2012, December).
But along with new opportunities come new risks. Psychologists who use social media to communicate with colleagues, for instance, may inadvertently compromise confidentiality in seeking advice about how to tailor therapy for a particular client. (As you well know, what’s said online stays online.) Others may go online to investigate clients’ statements about themselves (He claims to have 400 Facebook friends; let me just take a peek and confirm; Kolmes, 2012, December).
DOES FACEBOOK HAVE A PLACE IN THERAPY?
As you can see, the emergence of social media presents new challenges and new opportunities for therapists. This is an area in which we would like to see more research. Stay tuned. . . . 
 PASSIONATE PROVIDERS Before wrapping up, we thought you might like to know what Dr. Dan Foster and Laura Lichti are doing these days. Dr. Foster is as busy as ever, working with one other psychologist and a mental health technician to provide mental health services to Rosebud’s 13,000 residents. In addition to working up to 70 hours per week, he and his wife Becky (also a doctorate-
PASSIONATE PROVIDERS Before wrapping up, we thought you might like to know what Dr. Dan Foster and Laura Lichti are doing these days. Dr. Foster is as busy as ever, working with one other psychologist and a mental health technician to provide mental health services to Rosebud’s 13,000 residents. In addition to working up to 70 hours per week, he and his wife Becky (also a doctorate-
It’s been a time of growth for Laura, who is now working as a behavior therapist for people with intellectual and developmental disabilities. She also opened her own private practice, which focuses on grief counseling for people of all ages, and began teaching psychology at a community college. “I love the variety,” Laura says. “It keeps me very busy!”
Lee Bernhard
show what you know
Question 1
1. A large study in Los Angeles County found that non-
less; the same
more; the same
more; a different
equally; a different
b. more; the same
Question 2
2. E-
licensing issues; privacy issues
Question 3
3. If you were trying to convince a friend that treatment for psychological disorders works for many groups of people, how would you summarize the effectiveness of psychotherapy? What would you say about the role of culture in its outcome?
Answers will vary, but may be based on the following information. In general, therapy “works,” especially if it is long-
Question 4
4. A single man has had trouble dealing with his coworkers and has not been on a second date in over a year because of his poor interpersonal skills. His therapist decides the best course of treatment is _________________, which is led by one or two mental health professionals, involves three or more clients, and allows the therapists to observe the client interacting with others.
group therapy
Question 5
5. Under what conditions might group therapy fail or be inappropriate?
Answers will vary (see Table 13.3). Group therapy would be inappropriate for an individual who is not comfortable talking or interacting with others and is unwilling to share his or her own thoughts, feelings, or problems. A group may fail if group members do not get along, are continually late for meetings, or drop out. The skills of the group therapist also play a role in the success of treatment (for example, empathy, facilitation skills, observation skills).