Instructor's Notes
The following resources are available for this selection through the “Resources” panel or by clicking on the “Browse Resources for this Unit” button:
- An autograded multiple-
choice quiz - A summary activity with a sample summary as feedback
- A synthesis prompt
Gary S. Becker
Julio J. Elías Cash for Kidneys: The Case for a Market for Organs

GARY S. BECKER, a Nobel Prize–winning professor of economics and sociology at the University of Chicago, collaborated with Julio J. Elías, professor of economics and business at the Universidad del CEMA in Argentina, on this proposal to solve the kidney shortage. As economists who seek real-
1
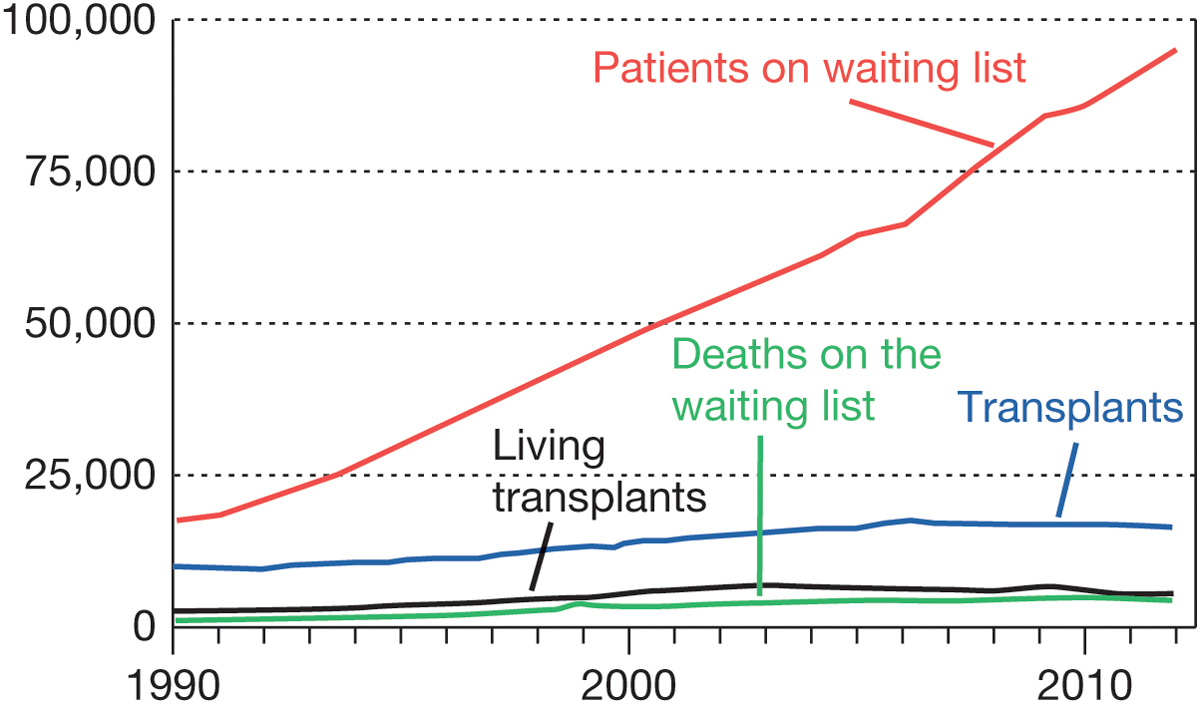
I n 2012, 95,000 American men, women and children were on the waiting list for new kidneys, the most commonly transplanted organ. Yet only about 16,500 kidney transplant operations were performed that year. Taking into account the number of people who die while waiting for a transplant, this implies an average wait of 4.5 years for a kidney transplant in the U.S.
2
The situation is far worse than it was just a decade ago, when nearly 54,000 people were on the waiting list, with an average wait of 2.9 years. For all the recent attention devoted to the health-
3
Finding a way to increase the supply of organs would reduce wait times and deaths, and it would greatly ease the suffering that many sick individuals now endure while they hope for a transplant. The most effective change, we believe, would be to provide compensation to people who give their organs—
4
Organ transplants are one of the extraordinary developments of modern science. They began in 1954 with a kidney transplant performed at Brigham & Women’s Hospital in Boston. But the practice only took off in the 1970s with the development of immunosuppressive drugs that could prevent the rejection of transplanted organs. Since then, the number of kidney and other organ transplants has grown rapidly, but not nearly as rapidly as the growth in the number of people with defective organs who need transplants. The result has been longer and longer delays to receive organs.
5
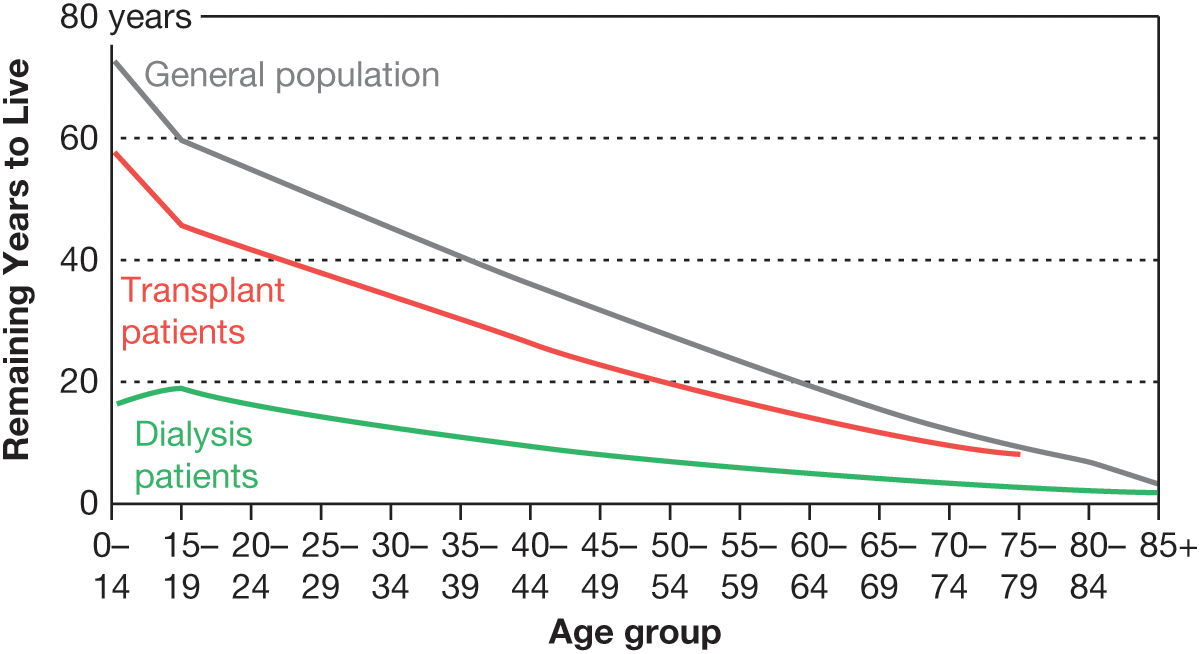
Many of those waiting for kidneys are on dialysis, and life expectancy while on dialysis isn’t long. For example, people age 45 to 49 live, on average, eight additional years if they remain on dialysis, but they live an additional 23 years if they get a kidney transplant. That is why in 2012, almost 4,500 persons died while waiting for kidney transplants. Although some of those waiting would have died anyway, the great majority died because they were unable to replace their defective kidneys quickly enough.
6
The toll on those waiting for kidneys and on their families is enormous, from both greatly reduced life expectancy and the many hardships of being on dialysis. Most of those on dialysis cannot work, and the annual cost of dialysis averages about $80,000. The total cost over the average 4.5-
7
Individuals can live a normal life with only one kidney, so about 34% of all kidneys used in transplants come from live donors. The majority of transplant kidneys come from parents, children, siblings and other relatives of those who need transplants. The rest come from individuals who want to help those in need of transplants.
8
In recent years, kidney exchanges—
9
Exhortations and other efforts to encourage more organ donations have failed to significantly close the large gap between supply and demand. For example, some countries use an implied consent approach, in which organs from cadavers are assumed to be available for transplant unless, before death, individuals indicate that they don’t want their organs to be used. (The U.S. continues to use informed consent, requiring people to make an active declaration of their wish to donate.) In our own highly preliminary study of a few countries—
10
Other studies have found more positive effects from switching to implied consent, but none of the effects would be large enough to eliminate the sizable shortfall in the supply of organs in the U.S. That shortfall isn't just an American problem. It exists in most other countries as well, even when they use different methods to procure organs and have different cultures and traditions.
11
Paying donors for their organs would finally eliminate the supply-
12
We have estimated how much individuals would need to be paid for kidneys to be willing to sell them for transplants. These estimates take account of the slight risk to donors from transplant surgery, the number of weeks of work lost during the surgery and recovery periods, and the small risk of reduction in the quality of life.
13
Our conclusion is that a very large number of both live and cadaveric kidney donations would be available by paying about $15,000 for each kidney. That estimate isn’t exact, and the true cost could be as high as $25,000 or as low as $5,000—
14
Since the number of kidneys available at a reasonable price would be far more than needed to close the gap between the demand and supply of kidneys, there would no longer be any significant waiting time to get a kidney transplant. The number of people on dialysis would decline dramatically, and deaths due to long waits for a transplant would essentially disappear.
15
Today, finding a compatible kidney isn’t easy. There are four basic blood types, and tissue matching is complex and involves the combination of six proteins. Blood and tissue type determine the chance that a kidney will help a recipient in the long run. But the sale of organs would result in a large supply of most kidney types, and with large numbers of kidneys available, transplant surgeries could be arranged to suit the health of recipients (and donors) because surgeons would be confident that compatible kidneys would be available.
16
The system that we’re proposing would include payment to individuals who agree that their organs can be used after they die. This is important because transplants for heart and lungs and most liver transplants only use organs from the deceased. Under a new system, individuals would sell their organs “forward” (that is, for future use), with payment going to their heirs after their organs are harvested. Relatives sometimes refuse to have organs used even when a deceased family member has explicitly requested it, and they would be more inclined to honor such wishes if they received substantial compensation for their assent.
17
The idea of paying organ donors has met with strong opposition from some (but not all) transplant surgeons and other doctors, as well as various academics, political leaders and others. Critics have claimed that paying for organs would be ineffective, that payment would be immoral because it involves the sale of body parts and that the main donors would be the desperate poor, who could come to regret their decision. In short, critics believe that monetary payments for organs would be repugnant.
18
But the claim that payments would be ineffective in eliminating the shortage of organs isn’t consistent with what we know about the supply of other parts of the body for medical use. For example, the U.S. allows market-
19
Another illuminating example is the all-
Any claim about the supposed immorality of organ sales should be weighed against the morality of preventing thousands of deaths each year. . . .
20
Whether paying donors is immoral because it involves the sale of organs is a much more subjective matter, but we question this assertion, given the very serious problems with the present system. Any claim about the supposed immorality of organ sales should be weighed against the morality of preventing thousands of deaths each year and improving the quality of life of those waiting for organs. How can paying for organs to increase their supply be more immoral than the injustice of the present system?
21
Under the type of system we propose, safeguards could be created against impulsive behavior or exploitation. For example, to reduce the likelihood of rash donations, a period of three months or longer could be required before someone would be allowed to donate their kidneys or other organs. This would give donors a chance to re-
22
Though the poor would be more likely to sell their kidneys and other organs, they also suffer more than others from the current scarcity. Today, the rich often don’t wait as long as others for organs since some of them go to countries such as India, where they can arrange for transplants in the underground medical sector, and others (such as the late Steve Jobs) manage to jump the queue by having residence in several states or other means. The sale of organs would make them more available to the poor, and Medicaid could help pay for the added cost of transplant surgery.
23
The altruistic giving of organs might decline with an open market, since the incentive to give organs to a relative, friend or anyone else would be weaker when organs are readily available to buy. On the other hand, the altruistic giving of money to those in need of organs could increase to help them pay for the cost of organ transplants.
24
Paying for organs would lead to more transplants—
25
Initially, a market in the purchase and sale of organs would seem strange, and many might continue to consider that market “repugnant.” Over time, however, the sale of organs would grow to be accepted, just as the voluntary military now has widespread support.
26
Eventually, the advantages of allowing payment for organs would become obvious. At that point, people will wonder why it took so long to adopt such an obvious and sensible solution to the shortage of organs for transplant.