Depression
The general trend from late childhood through adolescence is toward less confidence, with more moments of emotional despair and anger than earlier—as well as more moments of happiness (Neumann et al., 2011). A dip in self-esteem at puberty is found for children of every ethnicity and gender (Fredricks & Eccles, 2002; Greene & Way, 2005; Kutob et al., 2010). Some studies report rising self-esteem thereafter, but variations are many, as are individual differences.
On average, self-esteem is lower in girls compared to boys, lower in Asian-Americans compared to African-Americans, and lower in younger adolescents compared to older adolescents (Bachman et al., 2011). Many studies report a gradual rise in self-esteem from early adolescence through at least age 30, but all find notable variability as well as some continuity, as you would expect since genes remain the same even as age increases. That means that seriously depressed adolescents cannot be promised “you’ll feel better soon”—depression lightens, but it rarely disappears (Huang, 2010).
Adolescents of any background with low self-esteem often turn to drugs, sex, self-harm, and dieting—all of which deepen depression (Biro et al., 2006; Trzesniewski et al., 2006). Some communities have lower rates of depression because they promote strong and supportive relationships between teenagers and adults; studies find that parents, as well as peers, affect self-esteem (Hall-Lande et al., 2007). One factor in an individual’s level of self-esteem may be the adolescents’ own neurological propensity (differential sensitivity again).
One of the first major surveys on depression in children in Canada was conducted by the Ontario Child Health Study on youths aged 6 to 16 in the late 1980s. Findings indicated that depression rates ranged by age from 2.7 to 7.8 percent. More recently, based on Statistics Canada’s Canadian Community Health Survey—Mental Health and Well-being (2003), Cheung and Dewa (2006) reported that for adolescents aged 15 to 18, the lifetime prevalence rate for depression was just under 8 percent. More females (11 percent) were depressed than males (4 percent). Also, teenagers living in the Maritimes had lower rates of depression than Ontario teens, while for those in British Columbia, the rates were higher. These gender and regional differences may be the result of variations in health care systems across the country that affect the accessibility of mental health services (Cheung & Dewa, 2006).
Clinical DepressionSome adolescents sink into clinical depression, a feeling of a deep sadness and hopelessness that disrupts all normal, regular activities. The origins and causes, such as alleles and early care, predate adolescence. Then puberty—with its myriad physical and emotional ups and downs—plunges some into despair. The rate of clinical depression more than doubles during this time, to an estimated 15 percent, affecting about 1 in 5 girls and 1 in 10 boys.
It is not known whether the reasons for these gender differences are primarily biological, psychological, or social (Alloy & Abramson, 2007). Obviously, sex hormones differ, but girls also experience social pressures from their families, peers, and cultures that boys do not. Perhaps the combination of biological and psychosocial stresses causes some to slide into depression.
Genes also play a factor. For instance, adolescent girls are especially likely to be depressed if their mothers are belligerent, disapproving, and contemptuous. However, some girls seem genetically protected. They have equally difficult mothers, but they escape depression, probably because they are innately less vulnerable (Whittle et al., 2011).
One study found that the short allele of the serotonin transporter promoter gene (5-HTTLPR) increased the rate of depression among girls everywhere but increased depression among boys only if they lived in communities of low SES (Uddin et al., 2010). It is not surprising that certain genes make depression more likely, but the gender-specific neighbourhood correlation is puzzling. Perhaps boys are more likely to become depressed if they see no job prospects, and that is more likely in economically disadvantaged neighbourhoods.
A cognitive explanation has been offered for gender differences in depression. Rumination—talking about, remembering, and mentally replaying past experiences—is more common among girls than boys. If unpleasant incidents are replayed, rumination may lead to depression (Ayduk & Kross, 2008).
Adolescent depression is expressed in many ways, including eating disorders, school alienation, and sexual risk taking, all already discussed. In addition, an increasing number of depressed adolescents turn to self-harm, specifically cutting themselves to draw blood, or burning themselves to relieve anxiety. Cutting and burning are not intended as suicide attempts; they temporarily halt the unbearable emotions that triggered self-abuse. However, such actions may become addictive, leading to deeper depression. That deeper depression is linked to suicide (Asarnow et al., 2011).
SuicideSerious depression can lead to thoughts about killing oneself (called suicidal ideation). Suicidal ideation can in turn lead to parasuicide, also called attempted suicide or failed suicide. It includes any deliberate self-harm that could have been lethal. Parasuicide is the best word to use because “failed” implies that death is success. “Attempt” is likewise misleading because, especially in adolescence, the difference between attempted and completed suicide is often luck, timing, and medical response. Depression and parasuicide are more common among females, but completed suicide is higher for males (except in China). A major reason for the greater percentage of males who complete suicide has to do with the method: Males typically jump from high places or shoot themselves (immediately lethal), whereas females often swallow pills or cut their wrists (allowing time for possible intervention or second thoughts). Another explanation is that girls talk about their emotions, allowing friends and families to help them. Boys withdraw; their warning signs are less obvious.
Suicide is the second leading cause of death among Canadian teenagers, next to accidents. In 2009, almost one-quarter (23 percent) of all deaths among 15- to 19-year-olds was the result of suicide (Statistics Canada, 2012f). Some gender differences were evident in this age group: The suicide rate for boys was 145 per 100 000, whereas for girls it was considerably less, at 57 per 100 000 (Statistics Canada, 2012g, 2012h). These statistics represent a fluctuation in suicide rates for youth aged 15 to 19 between 2005 and 2009, from 213 deaths in 2005 to 185 deaths in 2007 to 202 deaths in 2009, per 1000 youth. Over these same five years, rates steadily decreased for children aged 10 to 14 years, from 43 deaths to 25 deaths per 1000 (Statistics Canada, 2014b).
Youths from low-income families are at higher risk for suicide than youths from higher-SES families (Cheung & Dewa, 2006), though wealth and education do not decrease the incidence of suicide. One possibility is that adolescents from high-SES families may not know how to cope with a failing grade or a broken relationship. Rates of suicide are also higher for gay adolescents who have been rejected by family (Saewyc, 2011). There are regional differences in suicide, too. As is the case with depression, in British Columbia the rate of suicidal youths is higher than in Ontario (Cheung & Dewa, 2006). Alarmingly, the suicide rates for Aboriginal youth are about five to seven times higher than non-Aboriginal youth. More specifically, Inuit youth have the highest suicide rates in the world, at about eleven times the national average (Health Canada, 2013).
ESPECIALLY FOR Journalists You just heard that a teenage girl jumped off a tall building and died. How should you report the story? 
Many people mistakenly think suicide is more frequent in adolescence for four reasons:
- The rate, low as it is, is far higher than it appeared to be decades ago.
- Statistics on “youth” often include emerging adults, aged 18 to 25, whose suicide rates are higher than those of adolescents.
- Adolescent suicides capture media attention, and people of all ages make a logical error (called base rate neglect), noticing the published cases and not considering the millions of non-suicidal youth.
- Parasuicide may be more common in adolescence than later.
Because they are more emotional than analytical, adolescents are particularly affected when they hear about a suicide, either via media reports or from peers (Insel & Gould, 2008). That makes them susceptible to cluster suicides, a term for several suicides within a group over a brief span of time—a few weeks or months. If a high school student’s “tragic end” is sentimentalized, that elicits suicidal ideation among his or her peers. Media attention increases the risk.
Delinquency and Disobedience
Like low self-esteem and suicidal ideation, bouts of anger are common in adolescence. In fact, the moody adolescent could be both depressed and delinquent because externalizing and internalizing behaviour are more closely connected in adolescence than at any other age (Loeber & Burke, 2011). That is why teenagers jailed for assault (externalizing) are suicide risks (internalizing).
Externalizing actions are obvious. Many adolescents slam doors, defy parents, and complain to friends about parents or teachers. Some teenagers—particularly boys—act out by breaking laws. They steal, damage property, or injure others.
Before further discussing juvenile rebellion, we should emphasize that adolescents who commit serious crimes are unusual. Most teenagers usually obey the law, with moments of hot anger (loud profanity) or minor rebellion (smoking a joint), but nothing more. Dozens of longitudinal studies confirm that increased anger after puberty is normal, but anger is usually expressed in acceptable ways. For a few, anger explodes: Teens break something or hurt someone. And a few of that few have been aggressive throughout childhood, becoming worse after puberty.
Breaking the LawBoth the prevalence (how widespread) and the incidence (how frequent) of crime increase during adolescence and continue at high levels in emerging adulthood. Arrest statistics in every nation reflect this, although some nations have much higher arrest rates overall than others.
In Canada in 2006, 180 000 youth were implicated with violating the Criminal Code, which does not include traffic tickets. The rate was 6885 per 100 000, an increase of 3 percent over the previous year. However, 60 percent of these youths were not formally charged (Taylor-Butts & Bressan, 2008). As you can see in TABLE 10.2, Canadian youths committed 9560 violent offences (e.g., physical and sexual assault, robbery) and 1052 drug offences in 2010/2011.
Table : TABLE 10.2 Youth Admissions to Correctional Services, by Most Serious Offence
| Most serious offence |
2010/2011 |
| Total admissions of most serious offence |
43 344 |
| Total violent offences |
9 560 |
| Assault level 2 |
2 335 |
| Common assault |
2 395 |
| Sexual assault |
439 |
| Robbery |
2 512 |
| Other violent offences |
1 909 |
| Total property offences |
8 002 |
| Break and enter |
2 712 |
| Theft $5000 and under |
2 099 |
| Theft over $5000 |
442 |
| Possession stolen goods |
978 |
| Mischief |
1 264 |
| Other property offences |
507 |
| Other criminal code |
5 084 |
| Total other offences |
3 300 |
| Drug-related offences |
1 052 |
| Youth Criminal Justice Act (VJCA) and Young Offenders Act (YOA) |
2 007 |
| Other federal offences |
6 |
| Provincial and Municipal offences |
235 |
| Source: Statistics Canada, 2012k. |
Causes of DelinquencyTwo clusters of factors, one from childhood (primarily brain-based) and one from adolescence (primarily contextual), predict delinquency. Knowing this allows prevention to focus on causes.
The first of these clusters includes a short attention span, hyperactivity, inadequate emotional regulation, slow language development, low intelligence, early and severe malnutrition, autistic tendencies, maternal cigarette smoking, and being the victim of severe child abuse, especially if it includes blows to the head. Most of these factors are more common among boys than girls, which may be one reason why females account for only about 5 percent of the inmates in Canadian correctional facilities.
Any of these signs of neurological impairment (either inborn or caused by early experiences) increases the risk that a child will become a life-course-persistent offender (Moffitt et al., 2001). As the term implies, a life-course-persistent offender is someone who breaks the law before and after adolescence, as well as during it.
The second cluster of factors that predict delinquency encompasses risk factors that are primarily psychosocial. They include having deviant friends; having few connections to school; living in a crowded, violent, unstable neighbourhood; not having a job; using drugs and alcohol; and having close relatives (especially older siblings) in jail. These factors are more prevalent among low-income, urban adolescents, but are certainly not exclusive to them. At any income level, an adolescent who experiences several of these risks is likely to become an adolescence-limited offender, someone whose criminal activity starts at puberty and stops by age 21 (Moffitt, 2003). Adolescence-limited offenders break the law with their friends, facilitated by their chosen antisocial clique. More boys than girls are in this group, but some law-breaking cliques include both sexes (the gender gap in law-breaking is narrower in late adolescence than earlier or later) (Moffitt et al., 2001).
The criminal records of both types of teenagers may be similar. However, if adolescence-limited delinquents can be protected from various snares (e.g., quitting school, entering prison, drug addiction, early parenthood), they may outgrow their criminal behaviour. This is confirmed by other research: Few delinquent youth who are not imprisoned continue breaking the law in early adulthood (Monahan et al., 2009). This does not mean that adolescence-limited law-breaking should be ignored. Antisocial behaviour is dangerous, especially to other adolescents, who are victimized three times as often as adults (Baum, 2005). Fortunately, maturation puts an end to adolescence-limited law-breaking.
ESPECIALLY FOR Police Officers You see some 15-year-olds drinking beer in a local park when they belong in school. What do you do?
By contrast, life-course-persistent offending begins in childhood and continues in adulthood with more crime, less education, lower income, unhappy marriages, and violence (Huesmann et al., 2009). It extends to the next generation: If life-course-persistent offenders have children, those children are likely to become lawbreakers themselves, partly for genetic reasons but primarily because they will have been mistreated by their parents before and after birth.
One way to prevent adolescent crime is to analyze earlier behaviour patterns and stop delinquency before the police become involved. Three pathways can be seen:
- Stubbornness can lead to defiance, which can lead to running away—runaways are often victims as well as criminals (e.g., prostitutes, petty thieves).
- Shoplifting can lead to arson and burglary.
- Bullying can lead to assault, rape, and murder.
Each of these pathways demands a different response. The rebelliousness of the stubborn child can be channelled or limited until more maturation and less impulsive anger prevail. Those on the second pathway require stronger human relationships and moral education.
Those on the third pathway present the most serious problem. Bullies need to be stopped and helped in early childhood, as already discussed. If that does not occur, and a teenager is still a bully, intense treatment may deflect the pattern. If that does not occur, and a teenager is convicted of assault, rape, or murder, then arrest, conviction, and jail might be the only options. In all cases, intervention is more effective earlier than later (Loeber & Burke, 2011).
As you can see in Figure 10.4, both the crime rate and crime severity for Canadian youths ages 12 to 17 years decreased steadily over the 10-year period from 2001 to 2011. Although these data are solid, explanations are not. Possibilities include fewer school dropouts (more education means less crime); wiser judges (using community service and drug treatment to prevent escalation); better policing (arrests for misdemeanors are up, alerting parents); smaller families (parents attend more to each child); better contraception and legal abortion (wanted children less often become criminals); more immigrants (who are more law-abiding); less lead damage (reducing impulsivity); and stricter drug laws (binge drinking and use of drugs are down).
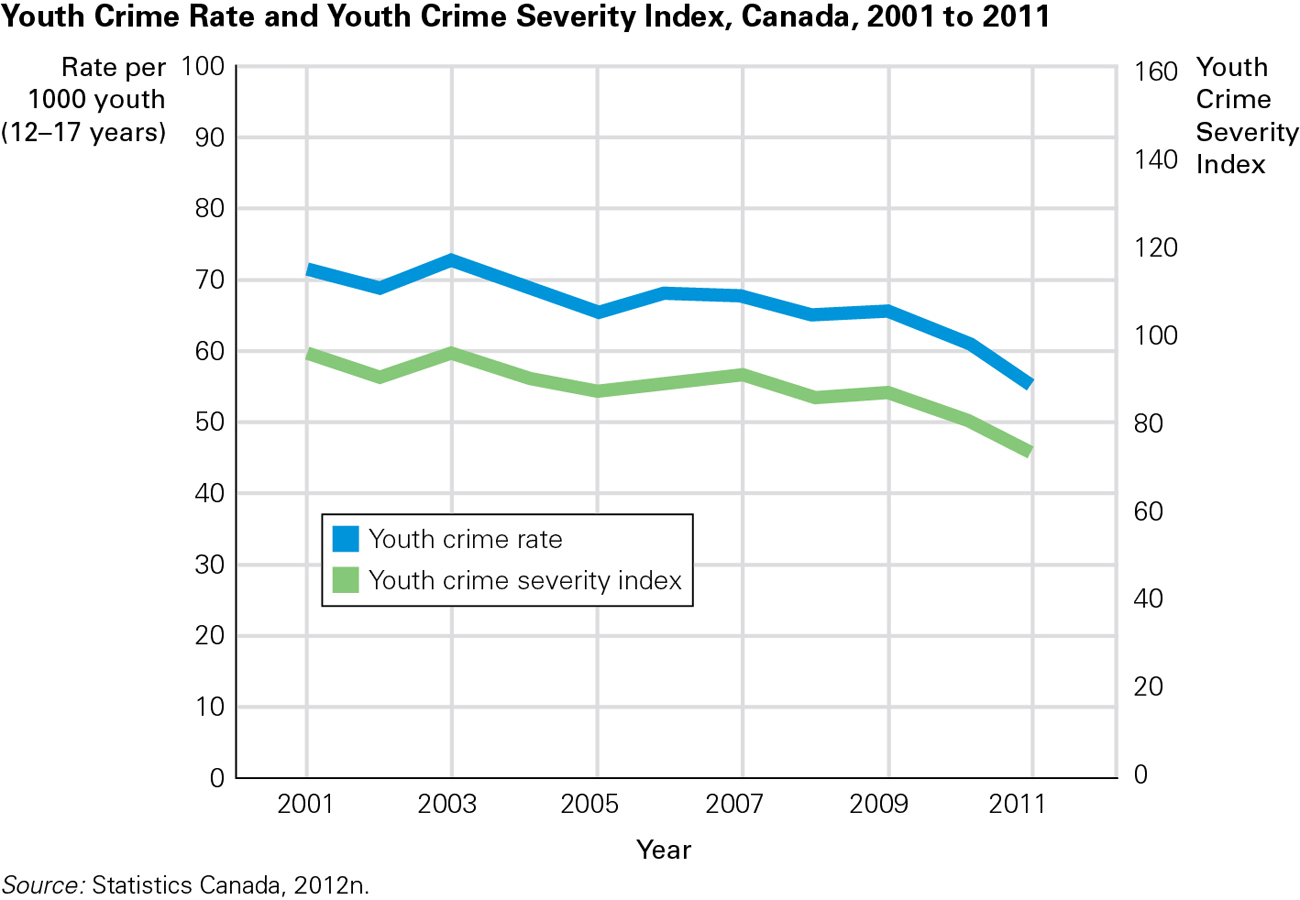
FIGURE 10.4 Good News? Youth crime has been steadily declining in Canada for several years. According to Statistics Canada, both the youth crime rate, which measures the volume of youth crime, and youth crime severity, a measure of the seriousness of youth crime, fell 10 percent in 2011, continuing a downward trend evident over the last decade. One reason for the continued decline may be that starting in 2003, when the Youth Criminal Justice Act was passed, the rate of youths diverted from the formal justice system has continually exceeded the rate of youths formally charged.
Source: Statistics Canada, 2012n.
KEY points
- The emotions of adolescents often include marked depression and anger, sometimes pathological, sometimes not.
- Clinical depression is more common in teenage girls than boys; experts disagree as to whether this is primarily caused by hormones, rumination, or society.
- Breaking the law is common among adolescents, with more arrests during these years than later.
- Some offenders are adolescence-limited—they stop breaking the law at adulthood; some are life-course-persistent—they become criminal adults.