9.7 Altered States of Consciousness
Thus far in this chapter, we’ve discussed aspects of conscious experience that everyone normally experiences on a daily basis. Each day, you sometimes are awake and consciously experiencing the world; you sometimes are asleep and in mentally active REM sleep; and you sometimes are in the mentally quieter state of non-
In addition to these three mental states, people occasionally experience alterations in normal, everyday conscious experience. We’ll conclude the chapter by looking at three alterations in conscious states that are produced by meditation, hypnosis, and psychoactive drugs.

Meditation
Preview Questions
Question
 What is meditation designed to do and what are its two main techniques?
What is meditation designed to do and what are its two main techniques?
Question
How do we know that meditation improves mental abilities?
Try the following three-
For a minute or so, pay attention to your conscious thoughts. What ideas run through your mind?
Now try that step again, while attempting to concentrate on just one idea or image. Let nothing other than that one image enter your mind.
Finally, try to think of nothing at all. Attempt, for a minute, to clear your mind of words and images.
If you’re like most people, numerous thoughts flit in and out of your head. Even if you’re trying to concentrate on just one thing, or to clear your mind of everything, ideas invade your conscious experience. The contents of your own mind can seem out of your control (Wegner, 1994).
TRY THIS!
You likely experienced difficulty controlling the contents of your conscious mind when you attempted our Try This! activity. You were asked to try not to think of a white bear. But when asked to indicate when one came to mind, you probably indicated that the bear frequently popped back into consciousness—
Can you gain greater control? People who meditate say you can. Meditation is any practice in which people focus their attention for an extended period of time (Walsh & Shapiro, 2006). Meditative methods are designed to increase people’s ability to concentrate. With practice, meditators gain greater ability to focus their minds on thoughts of their own choosing. The world’s cultures have produced numerous specific meditative techniques. Yet they can all be understood as one of two types (Goleman, 1988):
392
Concentration on a single object or event. In a meditation practice developed in the Himalayan region of South Asia, for example, meditators are instructed, during their first few months of meditative practice, to focus solely on the flow of their own breath (Rama, 1998). In other meditation traditions, practitioners may concentrate on a repeated word or phrase, known as a mantra; for example, “om” is a common mantra in South Asian meditative practice.
Clear the mind of all thoughts. A second meditative goal is to attain a state of emptiness—
a mental void. The meditator tries to attain “non- conceptual experience” (Chodron, 1990), that is, an experience stripped of the concepts learned from society.
The significance of meditation differs for different people. For many, it is a religious practice. A Hindu may meditate on the qualities of a deity to better understand the spiritual world; an Islamic Sufi meditator may seek closer spiritual connection to the Prophet Muhammad and to Allah; and Buddhists may meditate to understand, accept, and alleviate suffering (Goleman, 1988). For many clinical psychologists, meditation is a therapy method (Walsh & Shapiro, 2006). Irrespective of their religious beliefs, they judge that meditative practice can help clients become aware of their thoughts and feelings and gain greater control over their emotional life (Baer, 2003).
In this chapter, we won’t focus on either the religious or therapeutic purposes of meditation. Instead, we’ll examine a third implication of meditative practice. Meditation can inform psychological science about the full spectrum of human conscious experiences. It potentially reveals a “fourth state” of consciousness that “has nothing in common with the [other] three” (wakeful consciousness, REM sleep, and non-
Do you think prayer can be considered a form of meditation?
You may be skeptical of this claim. Meditators seem to be just sitting there, doing nothing. Have they really attained a unique conscious experience, with superior power to focus their attention and control the contents of their minds? To find out, let’s examine scientific evidence on the effects of meditation. We’ll consider evidence at two levels of analysis: the influence of meditation on (1) psychological processes of the mind, and (2) biological mechanisms in the brain.
MEDITATION AND PSYCHOLOGICAL PROCESSES. Eastern spiritual traditions have claimed, for millennia, that meditative practice enhances mental skills. It is only in recent years that scientific evidence has validated this claim (Tang & Posner, 2009).
In studying meditation, contemporary psychological scientists take two steps that were not previously taken by traditional practitioners of meditation. One involves measurement. Psychologists have devised tests to measure precisely the degree to which meditation improves people’s ability to focus their attention. The other is the experimental comparison of groups. Researchers systematically compare individuals who have and have not meditated.

In one study, researchers used an “attentional blink” task to measure people’s skill in concentrating attention (Slagter et al., 2007). Participants viewed a series of about 20 letters and numbers that appeared extremely rapidly (about 1/20 of a second) on a computer screen. On some trials, most of the stimuli were numbers, but some were letters. After these stimuli went zipping by, participants were asked to report the letters that appeared. This proved a difficult task. People’s minds tended to wander after they saw the first letter—
393
MEDITATION AND BRAIN PROCESSES. Once you learn that meditation changes psychological abilities (specifically, the ability to focus attention), a new question arises: What brain mechanisms underlie these psychological changes? The psychological findings establish facts about the mind that can be explored at a biological level of analysis.
What would be some of the advantages of an increased ability to focus your attention?
A clue to identifying the brain systems that meditation influences can be found in basic research on attention. Attention, the psychological process in which people focus their minds on an object or idea, has long been of interest to experimental psychologists (Kahneman, 1973; Triesman, 1964; see Chapter 5). Contemporary research explores attention at both psychological and biological levels of analysis and identifies parts of the brain that are particularly central to the focusing of attention (Posner & Rothbart, 2007). Here, then, is the clue: These brain systems may be the ones that change when people engage in meditative training (Lutz et al., 2008).
To find out, researchers conducted a brain-
As predicted, the brain activity of expert meditators differed from that of non-
Research on meditation and the brain reinforces a conclusion about how the brain works. Brain systems are “plastic” (see Chapter 3). Neural connections are not entirely determined by your genetic makeup. Instead, the brain’s inner wiring changes as a result of your experience. Meditation is an experience that can significantly change the biology of the brain, and thus the mental abilities of the person.
THINK ABOUT IT
Research shows that the minds and brains of people who meditate differ from those of others. Why? Do meditators acquire specific mental skills? Or, thanks to hours spent in a calm meditative state, might they simply be more relaxed, with their emotional relaxation affecting the mind and brain?

394
WHAT DO YOU KNOW?…
Question 23
Which of these statements about meditation are accurate?
- vfpRHu1L5R5si42mDfYAc8g1//K7moFOfCirSH2ciKKxMx9H1ovW60/BPQ2bICdjmV1lKqTedVMTz0iUF1iOKkPfgdV/qK6AXkByS3jpllaaEjdiWd7BbzrZ29Nxe7NA3D3BncVp1QEitFYWhKEYIg==
- oToxwnLXTFKTsMvnUbVhp4rbZRNkod8LIPJHbzfTbtAaI4etvoNXIZ0Tw2EL3GkdQP0yoQQb+DiXJ4QKpgAP6BYIDhkD+4K8CkOEfCVL3SYnRjzsQJK52VuoZLVKW8BHFCLAcp16f2GPbVBl7Zpe3A==
- LZGIhGJFXQIBj/Cwv3mHSireILV4KVFcEPPAyYLIWAvEMeZr0zKwmk8zyxZdxIGhLdyi/8oSl329WKVGHacAeg6Hd0AtjvFlWe6rKab0Z/EgstEjfx8qc+McoytSPsTI7i/lV3ohCUVicGhhEh1seuL5lNB/u5A4FIe9earYftPYyYt3
- 6AmJUW3fwQVl5P0BPrRZSXjxcGL0nquTlFTigBLGYzdm4p9H7wsVemY9ZDsZvkP5YuzHqaVuVjEBQKRhTZJyln7AL02Ccrp2p4LQAuRu/6wCHtSwBrJb9Fs5/g3lH1xHfk6yf3mWHr1rDenrBxL/NIq3nmxUKL5uQKI+EDeIJOlvLOzo51k9gppQ0Mq/jgQF+vD7XmL5OZxOeMsQEoG1icbJrvoVVT/+723/xVPTdBExjZB64dc56IaJmKFY/4WGXgCKgu++20bTNMMSeR70X6e/atSytF5apzwfmPw3fTxhk7x8f4Xo7ZG3vC1BmbjF4fkwFBmvxwgvw4REUHGVvg==
- 1YWCqK+83vnmw3oKMR0kS/Z/0W1yWbqs7QOGglmiLSAvXfGFAOPQzaxHzqBA/qCk/BIApsTe6+aJL28Fg9VMWMS08ztEk5zKJPeA91sWsBvYwkGEi1CTDUM0nZ41vKkmsrCtpNUnFpEXDDMxNHJVkr270EJYK7xSFFf6QMVRe1LRbLdFi6Nk4P7wLo7gPI73YQvHJWIlZnAAu+tQoaVQDP6Nb316lEqwkxAhx/oF600nAssXlfoo3C7MGak1c81m2gcgGyyL4FtdSrPziSDwKWqERnwsDQLI7GOgwA==
Hypnosis
Preview Questions
Question
Is everyone hypnotizable?
Question
How is a hypnotic state induced?
Question
How do we know hypnosis works?
Most people learn something about hypnosis well before taking a psychology class. Popular culture—
Here in a course on psychological science, you have to “unlearn” much of what popular culture has taught you. In the popular-
Research shows, however, that hypnosis does not really work this way. It is not a method of mind control (Raz & Shapiro, 2002). People who are hypnotized do not entirely lose conscious control of their thoughts and actions, although it is true that they may sometimes perform behaviors that, they report, occurred outside of their control. It also is not as mysterious as it may first appear. Recent advances suggest that hypnosis can be understood through normal methods of psychological science (Posner & Rothbart, 2011).
Hypnosis is an altered state of consciousness brought about through interaction between someone who makes suggestions to an individual (the “hypnotist”) and a hypnotic subject. When hypnotized, the hypnotic subject becomes highly suggestible, that is, his or her behavior is unusually responsive to suggestions from the hypnotist, rather than being driven by personal goals and intentions. Hypnosis, then, is not a method of mind control, yet it also is not mere myth. It is a genuine phenomenon with real psychological effects; as one expert summarized, “Hypnotized subjects can be oblivious to pain; they hear voices that aren’t there and fail to see objects that are clearly in their field of vision; they are unable to remember the things that happened to them while they were hypnotized; and they carry out suggestions after hypnosis has been terminated” (Kihlstrom, 2007, p. 445). Let’s look more closely at the questions of how hypnosis works and who can be hypnotized.
THE “HOW” AND “WHO” OF HYPNOSIS. Psychologists induce states of hypnosis through hypnotic induction procedures. A standard procedure, long in use, combines relaxation and focused attention (Weitzenhoffer & Hilgard, 1962). At the outset, the hypnotist informs participants that the process of hypnosis is up to them; they can achieve a hypnotic state only if they want to. (Note how this actual practice differs from the popular-
395
You might be thinking, “This would never work on me.” If so, you may be right. Not everyone is hypnotizable. People differ considerably in their susceptibility to hypnosis.
Psychologists have developed procedures to identify who is, and is not, hypnotizable. In the Stanford Hypnotic Susceptibility Scale (Weitzenhoffer & Hilgard, 1962), the hypnotic subject undergoes an induction of the sort we just described and then receives suggestions regarding a series of tasks. Some are simple, such as the suggestion that one’s eyelids are getting heavy and are closing. Others are more elaborate. For example, the psychologist places three boxes in front of the subject and suggests, “I have placed two boxes in front of you … just two boxes. Do you see them?” (Weitzenhoffer & Hilgard, 1962, p. 44). Then the participants are asked what they see. The overall degree to which the subject responds to the suggestions indicates the depth to which the person has become hypnotized (e.g., saying “I see two boxes” would indicate greater depth). Results suggest that people differ widely in their hypnotizability. Only about one in eight or nine show substantial hypnotic effects on the full range of tasks (Kihlstrom, 2007).
In summary, then, hypnotic procedures can powerfully affect people’s psychological responses. But the strongest effects are seen in only a subset of highly hypnotizable people.
Have you ever tried hypnosis? If so, how hypnotizable were you?
PSYCHOLOGICAL EVIDENCE OF HYPNOTIC EFFECTS. Why do hypnotic induction procedures affect people’s responses? There are two possibilities:
Unique hypnotic effect: Hypnotic procedures create a unique mental state in which people’s thoughts and actions are controlled, to a substantial degree, by the hypnotist’s suggestions.
Social role effect: Hypnotic procedures cause people to act as if they are experiencing a unique mental state in which their thoughts and actions are controlled by the hypnotist’s suggestions. They adopt the social role of “hypnotized person” (Sarbin, 1950; Spanos & Hewitt, 1980).
Many situations create social roles. At the doctor, you are expected to act in a manner consistent with the social role of “patient.” In class, you are expected to act according to the role of “student.” Possibility #2 suggests that, similarly, being in a hypnotic procedure causes people to act according to the role of “hypnotized person.” They adopt the role, convince themselves that they are hypnotized, and interpret their own behavior accordingly.
Which possibility do you think is correct? Before you try to answer that question, consider some research by the eminent psychologist Ernest Hilgard and his colleagues (Hilgard, Morgan, & Macdonald, 1975). They hypnotized participants and then asked them to put one of their hands in painfully cold water. Prior to this chilly experience, the hypnotist made two suggestions to participants: (1) They would not consciously experience any pain when their hand was in the water, but (2) a “hidden part” of them would be aware of the pain. The researchers then measured pain in two ways: (1) Participants reported consciously, in words, on their experiences; and, (2) in a procedure designed to tap the “hidden part” of the individual, participants typed numbers onto a keypad to indicate their level of pain.
396
Hilgard and colleagues found that the conscious and “hidden” parts of hypnotized participants provided different pain reports (Hilgard et al., 1975). Consciously, hypnotized subjects reported little pain, despite having plunged a hand in frigid water. However, when typing numbers into a keypad, many participants reported that they were in pain.
The researchers interpreted this finding as evidence that hypnotized participants’ minds contain two parts that, through hypnosis, become disconnected. The conscious part truly experiences no pain, as a result of hypnosis. The “hidden part,” however, is aware of the pain.
Other research similarly shows the action of different parts of the mind. Hypnotized people have been shown information (e.g., a list of words) and then given a hypnotic suggestion for amnesia, that is, the suggestion that they will lose their memory of the material. Later, they are given tests of both explicit and implicit memory (Chapter 6). After the hypnotic suggestion, people lack explicit memory; they don’t consciously remember the material. Yet they do have implicit memory; when performing a task that requires them to think of a word, they tend to think of one that was on the previous word list (Kihlstrom, 2007). The results thus suggest that the mind contains at least two different memory systems.
This conclusion—
What about the social role hypothesis? Some psychologists think that the findings of Hilgard and colleagues can be explained in terms of social roles (Spanos & Hewitt, 1980). Others, however, doubt this. They think it unlikely that the social role hypothesis can explain complex phenomena such as a participant’s different levels of performance on tests of implicit and explicit memory. In general, then, research suggests that—
BIOLOGICAL EVIDENCE OF HYPNOTIC EFFECTS. You still might be skeptical about hypnosis. It’s not impossible that the psychological evidence we just reviewed can be explained in terms of social roles. Biological evidence would be even more convincing. Since people generally cannot voluntarily control the activation of regions of their brains, any effects of hypnosis on brain functioning could not be explained by saying that people voluntarily adopted the social role of “hypnotized person.”
Researchers have, in fact, obtained such evidence. Using a research procedure similar to that of Hilgard and colleagues, researchers examined the effects of hypnosis on the experience of pain (Vanhaudenhuyse et al., 2009). They added a procedure unavailable to Hilgard decades earlier: fMRI, which enabled them to study brain activity during a painful task.
Highly hypnotizable participants took part in research procedures on two different days, during which they either were or were not hypnotized. The painful stimuli on both days were brief pulses of a laser directed to the back of the left hand. (The laser stimulated pain receptors, thereby producing a sensation of pain.) Researchers recorded brain activity and also asked participants to rate the severity of the pain they experienced.
397
As in prior research, hypnosis reduced conscious pain. Participants reported less pain on the day they were hypnotized. In addition, hypnosis influenced brain activation. When participants were not hypnotized, the laser pulses caused activation in a wide variety of brain regions. However, when they were hypnotized, these same stimuli remarkably “failed to elicit any cerebral activation” (Vanhaudenhuyse et al., 2009, p. 1050; Figure 9.7). Hypnosis apparently caused high-
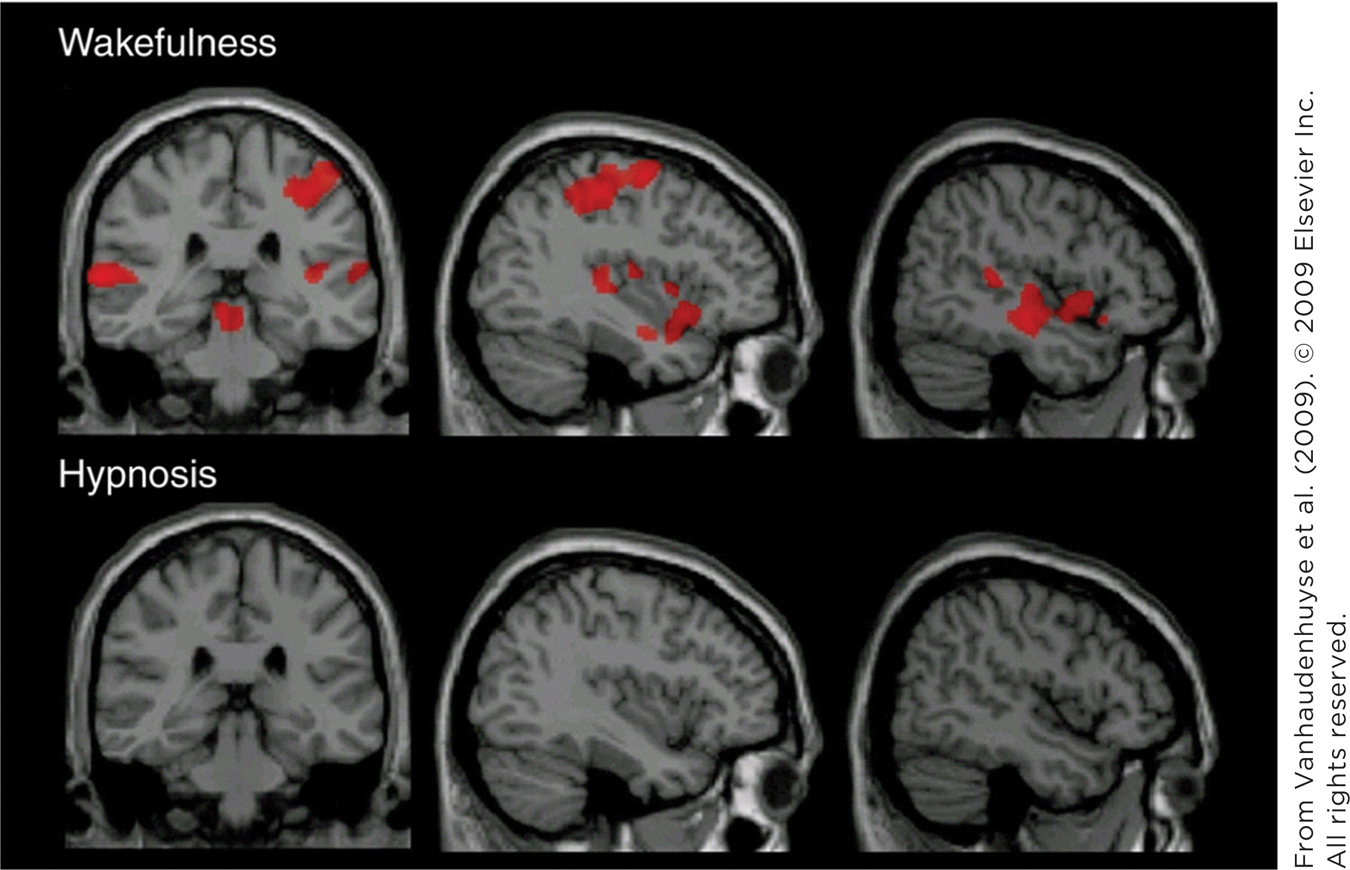
The key finding, then, is that identical stimuli had different effects on neural activity when participants were hypnotized. This should be enough to convince even the skeptic that hypnosis is a real phenomenon that influences both mind and brain.
WHAT DO YOU KNOW?…
Question 24
A standard hypnotic b4p5Doz8GpSarsVZeHWHCQ== procedure involves relaxation and focused attention. Once hypnotized, people are highly MXVzKjPPBuf4YhgaBqxp0Q==; they are willing to be guided by the instructions of a hypnotist. Only about one in eight or nine people are able to be 2Zotrc0/nGTAzjG1qDyvrQ==. Hilgard’s research indicated that people’s minds have two parts that become disconnected during hypnosis and that they map onto explicit and dU7oeVLigOsooOD/BszTWw== memory. Experimental research suggests that hypnosis alters both the mind and DFWnZgt9nnTSLKGc.
Psychoactive Drugs
Preview Question
Question
What are the effects of hallucinogens, opioids, stimulants, and depressants and how do they work?
A while back, some residents of the Caribbean wanted to alter their conscious states. They did so the quick way: They took out their paraphernalia—
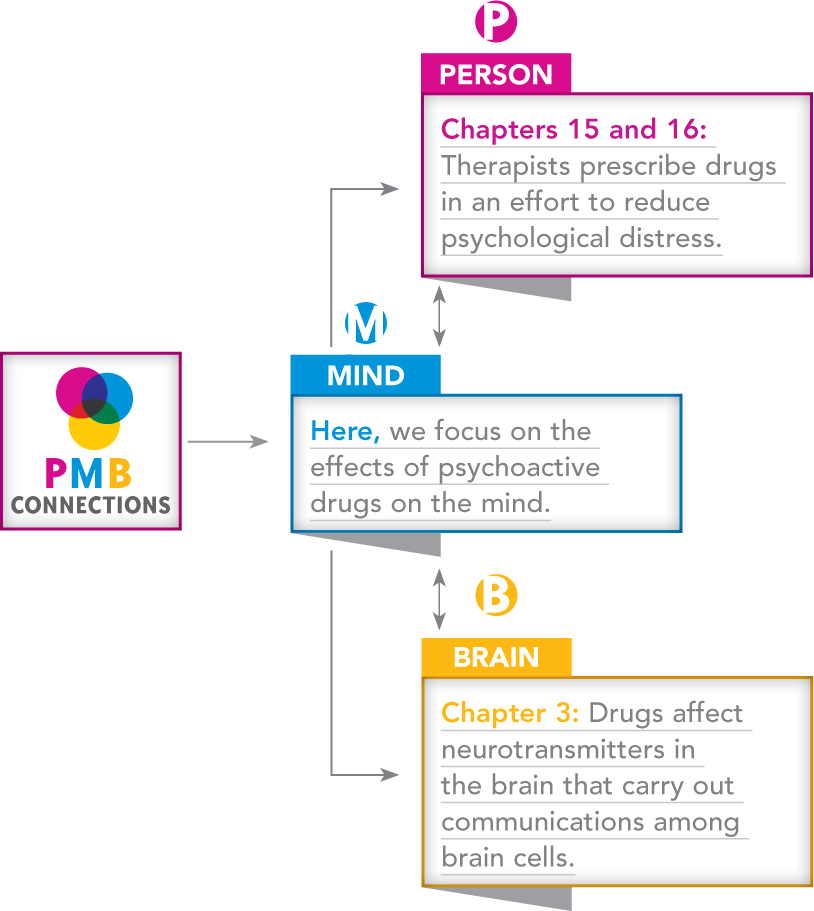
Humans, then, have long used psychoactive drugs. A psychoactive drug is any chemical substance that affects the nervous system in a manner that alters conscious experience. Psychoactive drugs exert these effects by changing communications among cells in the nervous system.
Once people begin abusing drugs, it can be difficult for them to stop—
Why are psychoactive drugs so addicting? It’s primarily because they activate a reward center in the brain (Tan, Rudolph, & Lüscher, 2011). The brain’s reward center normally produces pleasurable feelings when organisms engage in activities that are naturally rewarding, such as eating or sex. Drugs artificially activate this reward system and thereby directly create such feelings of pleasure. This makes them highly addicting. (Chapter 11 discusses motivational processes and brain mechanisms that can cause people to become addicted to stimulant drugs.)
398
There are different types of psychoactive drugs. We’ll examine four: hallucinogens, opioids, stimulants, and depressants.
HALLUCINOGENS. Hallucinogens are substances that profoundly alter consciousness, causing people to experience phenomena such as hallucinations and a loss of contact with reality. Hallucinogenic effects have long been experienced across the globe. Traditional cultures in Central America, South America, and South Asia have used hallucinogens in religious ceremonies for centuries (Nichols, 2004).
Traditional cultures discovered the effects of hallucinogenic substances that occur naturally. “Magic” mushrooms found in Mexico and South America, for example, produce hallucinogenic effects because they contain psilocybin, a chemical substance that powerfully alters mental experiences.
More recently, people have produced hallucinogens synthetically, that is, by combining chemicals in a laboratory. The first to do so was Albert Hoffman, a Swiss chemist working on drugs for migraine headaches. In 1943 he reported an unusual experience: “a not unpleasant intoxicated-
Everything in my field of vision wavered and was distorted as if seen in a curved mirror…. Everything in the room spun around, and the familiar objects and pieces of furniture assumed grotesque, threatening forms…. I was seized by the dreadful fear of going insane.
—Hoffman (1979, pp. 48–
CONNECTING TO NEUROTRANSMITTER SYSTEMS AND THERAPIES FOR PSYCHOLOGICAL DISORDERS
Hoffman had experienced the first LSD “trip.”
For two decades after Hoffman’s discovery, few people in the United States experienced LSD trips. But the drug gained popularity in the 1960s, due largely to the efforts of two psychologists at Harvard University, Timothy Leary and Richard Alpert (Lattin, 2010). They first experienced hallucinogens when sampling magic mushrooms in Mexico. They then experimented with LSD and became convinced that it was beneficial, awakening users to new, enlightening conscious experiences. Leary and Alpert gave the drug to colleagues, writers, artists, and even their students. They launched a campaign to get people, as Leary put it, to “turn on, tune in, and drop out” of mainstream society by exploring LSD’s mind-
Their campaign was remarkably successful. Hallucinogens became a staple of the 1960s counterculture. Popular music and art reflected, and contributed to, growth in the use of these drugs.
Today, hallucinogen use persists. About 1% of teens and 7% of young adults in the United States have tried LSD at least once (Substance Abuse and Mental Health Services Administration [SAMHSA], 2010). It persists despite legal sanctions: Possession of hallucinogens is illegal. It persists despite health risks: Hallucinogens can impair health through multiple routes. For example, some users feel that they have superhuman powers and attempt bizarre, dangerous activities such as trying to fly (Nichols, 2004). Another risk is psychological. Among people who are predisposed to psychological distress, the disturbing alterations of consciousness that hallucinogens create can trigger depression or psychosis, that is, a loss of the normal ability to understand the world of reality (Nichols, 2004).
399
Some readers of this text may be seeking an expansion of conscious experience. If so, compare pills to skills. As you learned above, the skills of meditation enhance conscious awareness—
What biological processes explain LSD’s psychological effects? The drug affects the actions of the neurotransmitter serotonin (Aghajanian & Marek, 1999; Nichols, 2004). When people take LSD, brain cells that are activated by serotonin—
Evidence indicates that hallucinogens may have additional biological effects (Fantegrossi, Murnane, & Reissig, 2008). Both LSD and the psilocybin found in magic mushrooms uniquely influence the inner workings of brain cells in the cortex (González-

OPIOIDS. Opioids are chemical substances whose primary psychoactive effect is the reduction of pain. They reduce pain by attaching themselves to nervous system cells that are involved in generating pain and related emotions (Holden, Jeong, & Forrest, 2005). Through such action, the drug morphine, for example, lessens the transmission of pain signals from the body to the brain, thereby lowering the conscious experience of pain.
Pain reduction is not the opioids’ only psychoactive effect. Opioids can also produce powerful feelings of euphoria and ecstasy (van Ree, Gerrits, & Vanderschuren, 1999). This makes opioid drugs highly addictive. People crave the positive feelings they create and seek to avoid the withdrawal symptoms—
You don’t need to take drugs to experience the pain-
400

STIMULANTS. Stimulants are psychoactive drugs that increase nervous system activity and thus enhance alertness and energy. Stimulants also can enhance people’s sense of psychological well-
You might be in easy reach of the most commonly ingested stimulant drug right now: caffeine, a chemical compound found in coffee, tea, energy drinks, sodas, and chocolate. Caffeine increases alertness by interfering with naturally occurring biochemical processes that decrease brain activity (e.g., when you’re sleepy; Ribeiro & Sebastião, 2010). Although caffeine’s psychoactive effects are milder than those of some other stimulants, it still can be addicting. If regular users suddenly quit taking caffeine, they experience withdrawal symptoms such as headache and fatigue that are caused by changes in cerebral blood flow (Sigmon et al., 2009).
Another stimulant, nicotine, is found in tobacco products. Nicotine triggers the release of neurotransmitters that increase alertness, as well as a neurotransmitter, dopamine, that enhances feelings of pleasure and emotional well-
Ritalin is a stimulant drug that is sometimes prescribed to treat attention-
Amphetamines are powerful stimulants that increase alertness and produce euphoric feelings by affecting multiple neurotransmitters, including dopamine (Berman et al., 2009). Amphetamines have practical medical uses. However, both amphetamines and methamphetamines (a chemically similar stimulant) are used illegally as recreational drugs. More than half a million Americans at any given time use these drugs for the rush of energy and positive emotions they produce (SAMHSA, 2009). Cocaine, another simulant, has similar effects on conscious experience and thus is also highly addictive. Cocaine’s effects are particularly powerful when the drug is processed into a form that can be smoked, known as crack cocaine (Schifano & Corkery, 2008).
A drug that has gained in popularity in recent years is ecstasy, which is both a stimulant and a hallucinogen. Ecstasy can reduce anxiety and create feelings of intimacy and euphoria—
DEPRESSANTS. Depressants are psychoactive drugs that reduce arousal in the central nervous system. In so doing, they can lower conscious experiences of excitability and anxiety. Depressants achieve these effects in part by increasing the effects of inhibitory neurotransmitters, that is, neurotransmitters that reduce activity in the brain (Julien, 2005).
One class of widely used depressants is benzodiazepines, psychoactive drugs that reduce feelings of anxiety while also inducing muscular relaxation and sleepiness (Tan et al., 2011). Because of these effects, benzodiazepines such as Valium, Xanax, and Ativan are prescribed frequently to treat anxiety disorders (see Chapter 15). In addition to reducing anxiety, benzodiazepines activate the brain’s reward center and thus produce pleasurable feelings. This makes them particularly addicting.
401
The most commonly used depressant of all is alcohol, a chemical compound found in beer, wine, and spirits. Beverages containing alcohol, which enhances the action of inhibitory neurotransmitters in the brain and reduces the action of excitatory neurotransmitters (Valenzuela, 1997), have been part of human societies for millennia. Various 7000-
How does alcohol affect behavior? It depends. Sometimes, a few drinks can make people warm and outgoing. At other times, drinking may cause those same individuals to become hostile and belligerent. Understanding these differences requires multiple levels of analysis: not just a brain level of analysis (the effects of alcohol on neural communication) but a mind level (analysis of the specific thinking processes that alcohol affects) and person level (in particular, consideration of the social setting in which the person is drinking).
At the level of the mind, alcohol has two notable effects: (1) reducing the amount of information in a situation that people can pay attention to and (2) impairing individuals’ ability to think deeply about that information (Steele & Josephs, 1990). In short, drinking impairs thinking. This impact of alcohol on mental processes, in turn, helps to explain the impact of drinking on people’s social behavior.
People who have been drinking are strongly affected by social cues. They are particularly influenced (before their attention is heavily impaired) by cues that happen to grab their attention. If they notice others who are pleasant, alcohol may increase their warmth and pleasantness. If they notice someone who they think is insulting them, alcohol may increase their belligerence. This is why the effects of alcohol on behavior “depend.” They depend on cues in a person’s immediate social environment.
Finally, let’s conclude our discussion of psychoactive substances with the most frequently used illicit drug, marijuana (NIDA, 2014). Marijuana is a difficult drug to classify, for two reasons. First, it produces a wide range of effects; marijuana can influence both conscious feelings and thinking abilities. Second, its effects vary; the exact influence of the drug on any given occasion depends on the amount of marijuana consumed, as well as on individual differences in people’s reaction to the drug (Ameri, 1999).
Despite these variations, there is a pattern of effects that occurs commonly. Users tend to experience feelings of euphoria accompanied by a relaxed, tranquil state (Ameri, 1999). These effects are caused by a chemical substance in marijuana, tetrahy-
In the past, public health officials sometimes exaggerated the negative effects of marijuana use. Today, by contrast, users may enjoy the drug’s psychological effects while giving little thought to its potential long-
Table 9.1 summarizes the psychoactive drugs we have reviewed, plus selected additional drugs whose use is relatively widespread.
| Psychoactive Drugs | ||
|---|---|---|
|
Drug |
Classification |
Common Short- |
|
Alcohol |
Depressant |
Relaxation, tension reduction, elevated mood |
|
Amphetamine |
Stimulant |
Increased alertness, euphoric feelings |
|
Benzodiazepine |
Depressant |
Reduced anxiety, relaxation, sleepiness |
|
Caffeine |
Stimulant |
Enhanced alertness, arousal, attention |
|
Cocaine |
Stimulant |
Euphoria, enhanced energy, alertness |
|
Ecstasy |
Hallucinogen, stimulant |
Reduced anxiety, euphoria, visual hallucinations |
|
Heroin |
Opioid |
Euphoric rush, “clouded” thinking, pain reduction |
|
LSD |
Hallucinogen |
Distorted sensory and perceptual experiences, intense positive and negative emotions |
|
Marijuana |
Depressant, hallucinogen |
Euphoria, calmness, distorted perception and impaired thinking, paranoia |
|
Nicotine |
Stimulant |
Elevated mood, relaxation, improved concentration, appetite reduction |
|
Psilocybin |
Hallucinogen |
Hallucinations, altered perception of time, intense emotional states |
|
Ritalin |
Stimulant |
Increased attention and concentration, reduced distractibility |
*The short-
402
WHAT DO YOU KNOW?…
Question 25
Hallucinogens such as lysergic acid diethylamide, or gRWLGCJqkz0=, cause people to hallucinate and to lose touch with reality. Opioids, such as the drug 11NHSz6jxuI6piXh9saYDA==, reduce the transmission of pain signals from the body to the brain. Nicotine, a nNqRjRlJ3HEP0Ui7Sfm8mQ==, triggers the release of the neurotransmitter IYCeJjg1eg+Q5dqWo8is5Q==, which enhances feelings of well-