Touch
18-4 How do we sense touch?
Touch is vital. Right from the start, touch aids our development. Infant rats deprived of their mother’s grooming produce less growth hormone and have a lower metabolic rate—a good way to keep alive until the mother returns, but a reaction that stunts growth if prolonged. Infant monkeys allowed to see, hear, and smell—but not touch—their mother become desperately unhappy; those separated by a screen with holes that allow touching are much less miserable. Premature human babies gain weight faster and go home sooner if they are stimulated by hand massage (Field et al., 2006). As adults, we still yearn to touch—to kiss, to stroke, to snuggle. This sort of touch soothes and protects. In one experiment, women felt less threatened by physical pain when holding their husband’s hand (Coan et al., 2006). Touch also helps communicate. In experiments, strangers separated by a curtain, using their hands to touch only the other’s forearms, have been able to communicate anger, fear, disgust, love, gratitude, and sympathy at levels well above chance (Hertenstein et al., 2006).

The precious sense of touch As William James wrote in his Principles of Psychology (1890), “Touch is both the alpha and omega of affection.”
© Jose Luis Pelaez, Inc./Blend Images/Corbis
Humorist Dave Barry was perhaps right to jest that your skin “keeps people from seeing the inside of your body, which is repulsive, and it prevents your organs from falling onto the ground.” But skin does much more. Touching various spots on the skin with a soft hair, a warm or cool wire, and the point of a pin reveals that some spots are especially sensitive to pressure, others to warmth, others to cold, still others to pain. Our “sense of touch” is actually a mix of these four basic and distinct skin senses, and our other skin sensations are variations of pressure, warmth, cold, and pain. Some examples:
Stroking adjacent pressure spots creates a tickle.
Repeated gentle stroking of a pain spot creates an itching sensation.
Touching adjacent cold and pressure spots triggers a sense of wetness, which you can experience by touching dry, cold metal.
Touch sensations involve more than tactile stimulation, however. A self-administered tickle produces less somatosensory cortex activation than does the same tickle from something or someone else (Blakemore et al., 1998). Likewise, a sensual leg caress evokes a different somatosensory cortex response when a heterosexual man believes it comes from an attractive woman rather than a man (Gazzola et al., 2012). Our responses to tickles and caresses reveal how quickly cognition influences our brain’s sensory response.
Pain
18-5 What biological, psychological, and social-cultural influences affect our experience of pain? How do placebos, distraction, and hypnosis help control pain?
Be thankful for occasional pain. Pain is your body’s way of telling you something has gone wrong. By drawing your attention to a burn, a break, or a sprain, pain orders you to change your behavior—“Stay off that turned ankle!” The rare people born without the ability to feel pain may experience severe injury or even death before early adulthood. Without the discomfort that makes us occasionally shift position, their joints fail from excess strain. Without the warnings of pain, the effects of unchecked infections and injuries accumulate (Neese, 1991).
More numerous are those who live with chronic pain, which is rather like an alarm that won’t shut off. The suffering of those with persistent or recurring backaches, arthritis, headaches, and cancer-related pain, prompts two questions: What is pain? How might we control it?
UNDERSTANDING PAIN Our pain experiences vary widely. Women are more sensitive to pain than men are (their senses of hearing and smell also tend to be more sensitive) (Ruau et al., 2012; Wickelgren, 2009). Our individual pain sensitivity varies, too, depending on genes, physiology, experience, attention, and surrounding culture (Gatchel et al., 2007; Reimann et al., 2010). Thus, our experience of pain reflects both bottom-up sensations and top-down cognition.
BIOLOGICAL INFLUENCES There is no one type of stimulus that triggers pain (as light triggers vision). Instead, there are different nociceptors—sensory receptors in our skin, muscles, and organs that detect harmful temperatures, pressure, or chemicals and send pain signals (FIGURE 18.6).
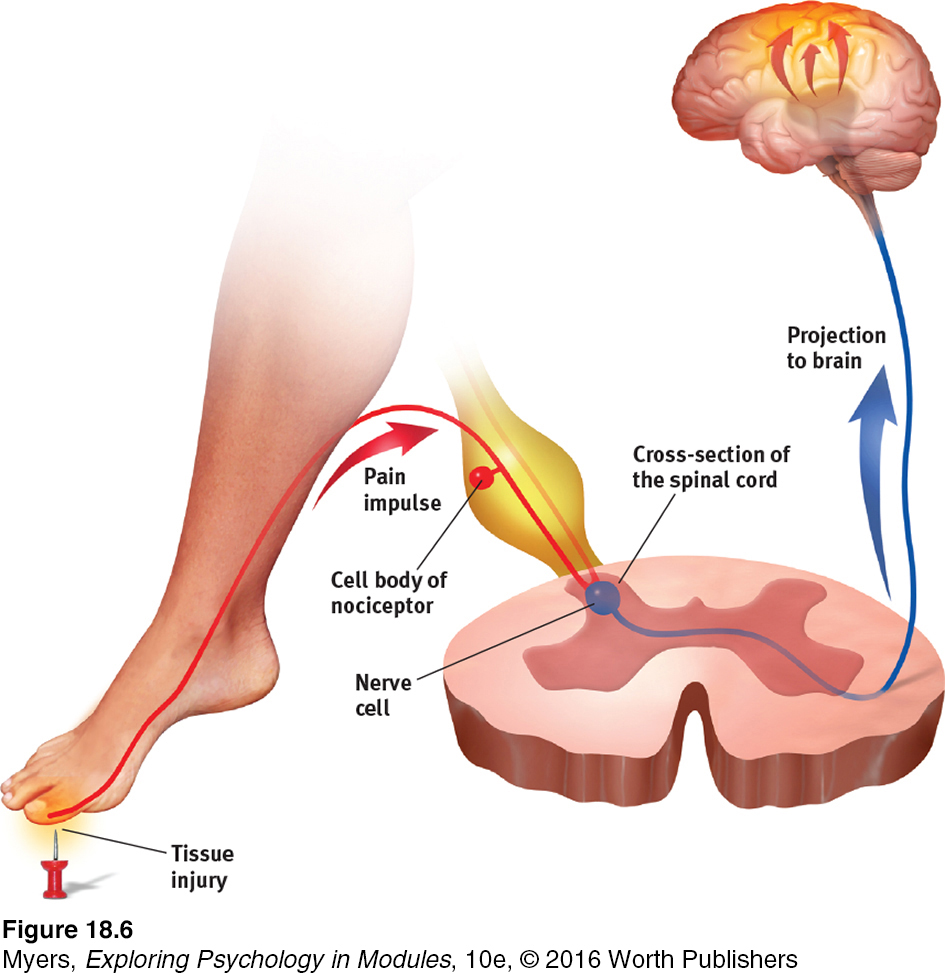
Figure 6.43: FIGURE 18.6 The pain circuit Sensory receptors (nociceptors) respond to potentially damaging stimuli by sending an impulse to the spinal cord, which passes the message to the brain, which interprets the signal as pain.
gate-control theory the theory that the spinal cord contains a neurological “gate” that blocks pain signals or allows them to pass on to the brain. The “gate” is opened by the activity of pain signals traveling up small nerve fibers and is closed by activity in larger fibers or by information coming from the brain.
Although no theory of pain explains all available findings, psychologist Ronald Melzack and biologist Patrick Wall’s (1965, 1983; Melzack & Katz, 2013) classic gate-control theory provides a useful model. The spinal cord contains small nerve fibers that conduct most pain signals, and larger fibers that conduct most other sensory signals. Melzack and Wall theorized that the spinal cord contains a neurological “gate.” When tissue is injured, the small fibers activate and open the gate, and you feel pain. Large-fiber activity closes the gate, blocking pain signals and preventing them from reaching the brain. Thus, one way to treat chronic pain is to stimulate (by massage, electric stimulation, or acupuncture) “gate-closing” activity in the large neural fibers (Wall, 2000).

“Pain is a gift.” So said a doctor studying Ashlyn Blocker, who has a rare genetic mutation that prevents her from feeling pain. At birth, she didn’t cry. As a child, she ran around for two days on a broken ankle. She has put her hands on a hot machine and burned the flesh off. And she has reached into boiling water to retrieve a dropped spoon. “Everyone in my class asks me about it, and I say, ‘I can feel pressure, but I can’t feel pain.’ Pain! I cannot feel it!”
Jeff Riedel/Contour/Getty Images
But pain is not merely a physical phenomenon of injured nerves sending impulses to a definable brain area—like pulling on a rope to ring a bell. The brain also creates pain, as it does in people’s experiences of phantom limb sensations after a limb has been amputated. Their brain may misinterpret the spontaneous central nervous system (CNS) activity that occurs in the absence of normal sensory input: As the dreamer may see with eyes closed, so 7 in 10 such people may feel pain or movement in nonexistent limbs (Melzack, 1992, 2005). (Some may also try to step off a bed onto a phantom leg or to lift a cup with a phantom hand.) Even those born without a limb sometimes perceive sensations from the absent arm or leg. The brain, Melzack (1998) has surmised, comes prepared to anticipate “that it will be getting information from a body that has limbs.”
Phantoms may haunt other senses too, as the brain, responding to the absence of sensory signals, amplifies irrelevant neural activity. People with hearing loss often experience the sound of silence: tinnitus, the phantom sound of ringing in the ears. Those who lose vision to glaucoma, cataracts, diabetes, or macular degeneration may experience phantom sights—nonthreatening hallucinations (Ramachandran & Blakeslee, 1998). Others who have nerve damage in the systems for tasting and smelling have experienced phantom tastes or smells, such as ice water that seems sickeningly sweet, or fresh air that reeks of rotten food (Goode, 1999). The point to remember: We feel, see, hear, taste, and smell with our brain, which can sense even without functioning senses.
PSYCHOLOGICAL INFLUENCES One powerful influence on our perception of pain is the attention we focus on it. Athletes, focused on winning, may play through the pain. Halfway through his lap of the 2012 Olympics 1600-meter relay, Manteo Mitchell broke one of his leg bones—and kept running.
We also seem to edit our memories of pain, which often differ from the pain we actually experienced. In experiments, and after medical procedures, people overlook a pain’s duration. Their memory snapshots instead record two factors: their pain’s peak moment (which can lead them to recall variable pain, with peaks, as worse [Stone et al., 2005]), and how much pain they felt at the end. In one experiment, researchers asked people to immerse one hand in painfully cold water for 60 seconds, and then the other hand in the same painfully cold water for 60 seconds followed by a slightly less painful 30 seconds more (Kahneman et al., 1993). Which experience would you expect to recall as most painful?
Curiously, when asked which trial they would prefer to repeat, most preferred the 90-second trial, with more net pain—but less pain at the end. Physicians have used this principle with patients undergoing colon exams—lengthening the discomfort by a minute, but lessening its intensity (Kahneman, 1999). Although the extended milder discomfort added to their net pain experience, patients experiencing this taper-down treatment later recalled the exam as less painful than did those whose pain ended abruptly. Likewise, after childbirth, women recall the total amount of pain in terms of the average of the peak and end pain, rather than the duration (Chajut, et al., 2014). (Imagine that, at the end of a painful root canal, the oral surgeon asks if you’d like to go home or to have a few more minutes of milder discomfort. If you want to remember less pain, there’s a case to be made for prolonging your hurt.)
The end of an experience can color our memory of pleasures, too. In one simple experiment, some people, on receiving a fifth and last piece of chocolate, were told it was their “next” one. Others, told it was their “last” piece, liked it better and also rated the whole experiment as being more enjoyable (O’Brien & Ellsworth, 2012). Endings matter.

Distracted from the pain After a tackle in the first half of a competitive game, BK Häcken soccer player Mohammed Ali Khan (in white) said he “had a bit of pain” but thought it was “just a bruise.” With his attention focused on the game, he played on. In the second half he was surprised to learn from an attending doctor that his leg was broken.
Reinhold Matay/AP Photo
SOCIAL-CULTURAL INFLUENCES Our perception of pain varies with our social situation and our cultural traditions. We tend to perceive more pain when others seem to be experiencing pain (Symbaluk et al., 1997). This may help explain other apparent social aspects of pain, as when pockets of Australian keyboard operators during the mid-1980s suffered outbreaks of severe pain while typing or performing other repetitive work—without any discernible physical abnormalities (Gawande, 1998). Sometimes the pain in sprain is mainly in the brain—literally. When people felt empathy for another’s pain, their own brain activity partly mirrored the activity of the actual brain in pain (Singer et al., 2004).
Thus, our perception of pain is a biopsychosocial phenomenon (Hadjistavropoulos et al., 2011). Viewing pain from many perspectives can help us better understand how to cope with it and treat it (FIGURE 18.7).
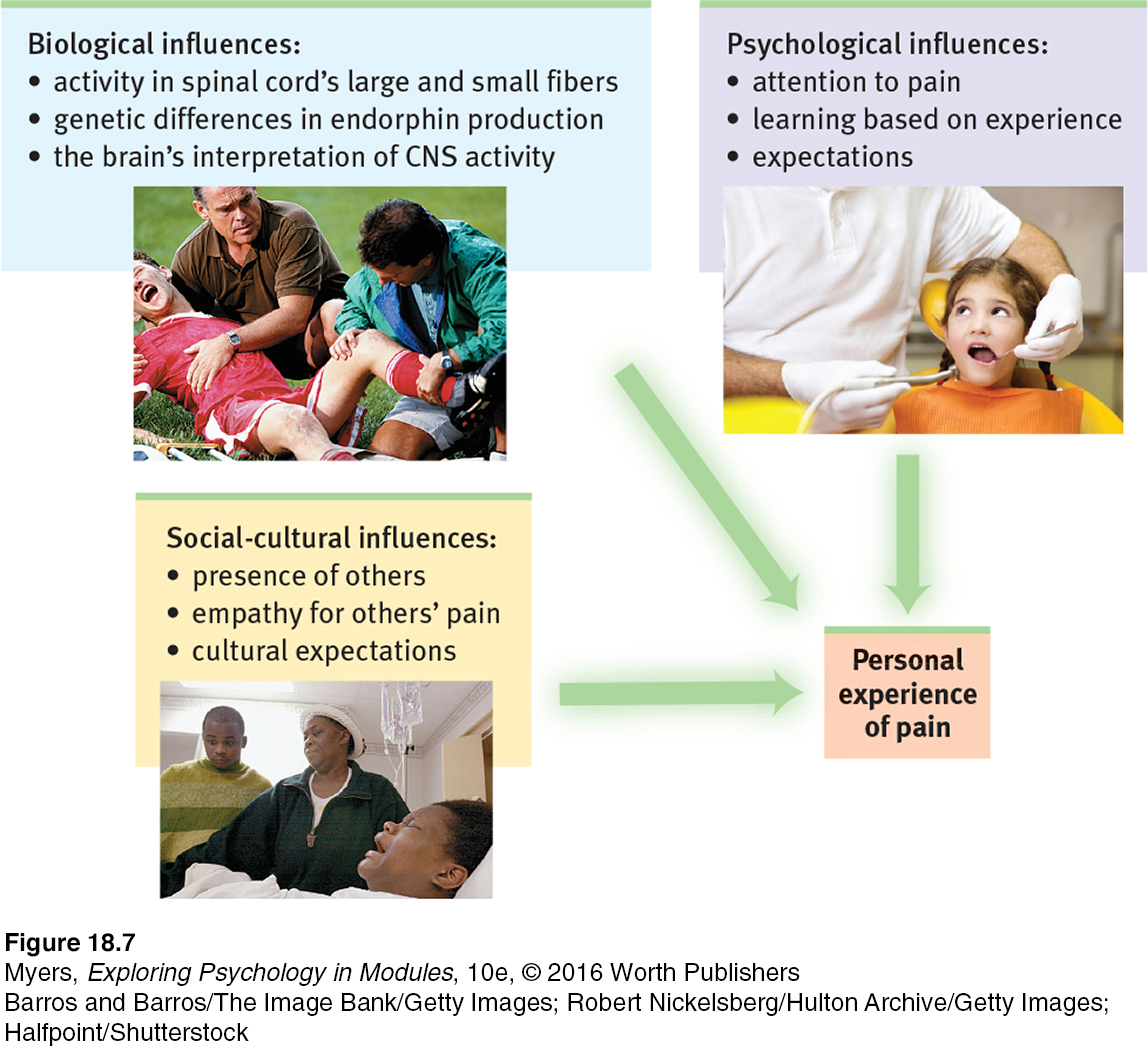
Figure 6.44: FIGURE 18.7 Biopsychosocial approach to pain Our experience of pain is much more than neural messages sent to our brain.
Barros and Barros/The Image Bank/Getty Images
Halfpoint/Shutterstock
Robert Nickelsberg/Hulton Archive/Getty Images

Acupuncture: A jab well done This acupuncturist is attempting to help this woman gain relief from back pain by using needles on points of the patient’s hand.
Gary Conner/Phototake
CONTROLLING PAIN If pain is where body meets mind—if it is both a physical and a psychological phenomenon—then it should be treatable both physically and psychologically. Depending on the patient’s symptoms, pain control clinics select one or more therapies from a list that includes drugs, surgery, acupuncture, electrical stimulation, massage, exercise, hypnosis, relaxation training, and thought distraction.
These options reflect some striking influences on pain. When we are distracted from pain (a psychological influence) and soothed by the release of our naturally painkilling endorphins (a biological influence), our experience of pain diminishes. Sports injuries may go unnoticed until the after-game shower. People who carry a gene that boosts the availability of endorphins are less bothered by pain, and their brain is less responsive to pain (Zubieta et al., 2003). Others, who carry a mutated gene that disrupts pain circuit neurotransmission, may be unable to experience pain (Cox et al., 2006). Such discoveries could point the way toward new pain medications that mimic these genetic effects.
PLACEBOS Even an inert placebo can help, by dampening the central nervous system’s attention and responses to painful experiences—mimicking painkilling drugs (Eippert et al., 2009; Wager & Atlas, 2013). After being injected in the jaw with a stinging saltwater solution, men in one experiment received a placebo said to relieve pain, and they immediately felt better. Sometimes “nothing works.” Being given fake painkilling chemicals caused the brain to dispense real ones, as indicated by activity in an area that releases natural painkilling opiates (Scott et al., 2007; Zubieta et al., 2005). “Believing becomes reality,” noted one commentator (Thernstrom, 2006), as “the mind unites with the body.”
“Pain is increased by attending to it.”
Charles Darwin, The Expression of the Emotions in Man and Animals, 1872
DISTRACTION Distracting people with pleasant images (“Think of a warm, comfortable environment”) or drawing their attention away from painful stimulation (“Count backward by 3’s”) is an effective way to activate pain-inhibiting circuits and to increase pain tolerance (Edwards et al., 2009). A well-trained nurse may chat with needle-shy patients and ask them to look away when inserting the needle. Burn victims receiving excruciating wound care can benefit from an even more effective distraction: immersion in a computer-generated 3-D world, like the snow scene in FIGURE 18.8. Functional MRI (fMRI) scans have revealed that playing in the virtual reality reduces the brain’s pain-related activity (Hoffman, 2004). Because pain is in the brain, diverting the brain’s attention may bring relief. Better yet, research suggests, maximize pain relief by combining a placebo with distraction (Buhle et al., 2012), and amplify their effects with hypnosis. Hypnosis can also divert attention (see Thinking Critically About: Hypnosis and Pain Relief).
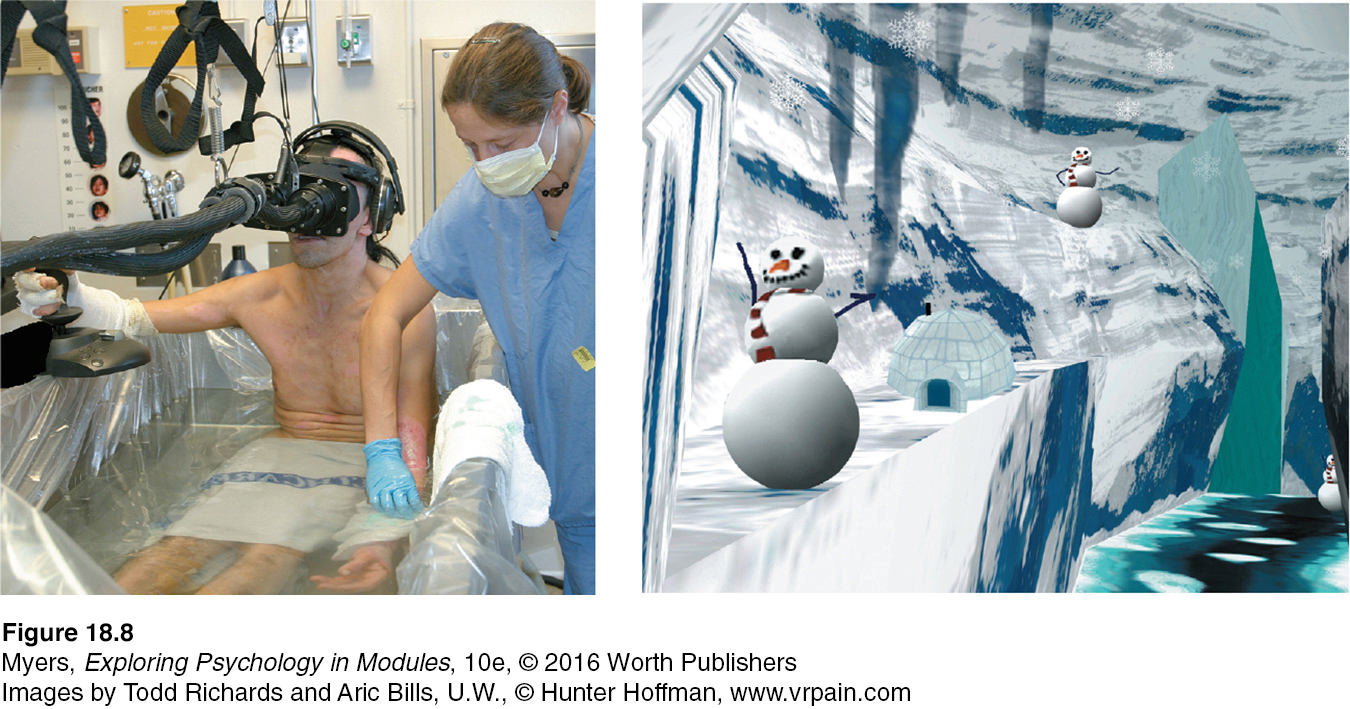
FIGURE 18.8 Virtual-reality pain control For burn victims undergoing painful skin repair, an escape into virtual reality can powerfully distract attention, thus reducing pain and the brain’s response to painful stimulation. fMRI scans have illustrated a lowered pain response when the patient is distracted.
Images by Todd Richards and Aric Bills, U.W., ©Hunter Hoffman, www.vrpain.com
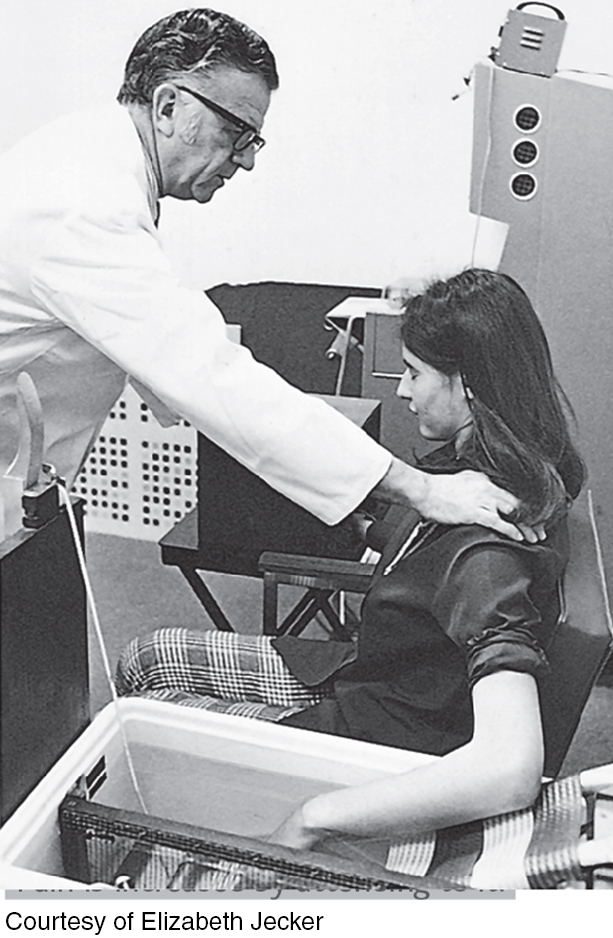
Dissociation or social influence? This hypnotized woman being tested by famous researcher Ernest Hilgard showed no pain when her arm was placed in an ice bath. But asked to press a key if some part of her felt the pain, she did so. To Hilgard (1986, 1992), this was evidence of dissociation, or divided consciousness. The social influence perspective, however, maintains that people responding this way are caught up in playing the role of “good subject.”
Courtesy of Elizabeth Jecker
THINKING CRITICALLY ABOUT
Imagine you are about to be hypnotized. The hypnotist invites you to sit back, fix your gaze on a spot high on the wall, and relax. In a quiet, low voice the hypnotist suggests, “Your eyes are growing tired… . Your eyelids are becoming heavy … now heavier and heavier… . They are beginning to close… . You are becoming more deeply relaxed… . Your breathing is now deep and regular… . Your muscles are becoming more and more relaxed… . Your whole body is beginning to feel like lead.”
hypnosis a social interaction in which one person (the hypnotist) suggests to another (the subject) that certain perceptions, feelings, thoughts, or behaviors will spontaneously occur.
After a few minutes of this hypnotic induction, you may experience hypnosis. Hypnotists have no magical mind-control power; they merely focus people on certain images or behaviors. To some extent, we are all open to suggestion. But highly hypnotizable people—such as the 20 percent who can carry out a suggestion not to smell or react to an open bottle of ammonia held under their nose—are especially suggestible and imaginative (Barnier & McConkey, 2004; Silva & Kirsch, 1992).
Can hypnosis relieve pain? Yes. When unhypnotized people put their arms in an ice bath, they felt intense pain within 25 seconds (Elkins et al., 2012; Jensen, 2008). When hypnotized people did the same after being given suggestions to feel no pain, they indeed reported feeling little pain. As some dentists know, light hypnosis can reduce fear, thus reducing hypersensitivity to pain. Hypnosis also lessens some forms of chronic pain (Adachi et al., 2014).
Hypnosis inhibits pain-related brain activity. In surgical experiments, hypnotized patients have required less medication, recovered sooner, and left the hospital earlier than unhypnotized control patients (Askay & Patterson, 2007; Hammond, 2008; Spiegel, 2007). Nearly 10 percent of us can become so deeply hypnotized that even major surgery can be performed without anesthesia. Half of us can gain at least some pain relief from hypnosis. The surgical use of hypnosis has flourished in Europe, where one Belgian medical team has performed more than 5000 surgeries with a combination of hypnosis, local anesthesia, and a mild sedative (Song, 2006).
Psychologists have proposed two explanations for how hypnosis works. One theory proposes that hypnosis is a form of normal social influence (Lynn et al., 1990, 2015; Spanos & Coe, 1992). In this view, hypnosis is a by-product of normal social and mental processes. Like actors caught up in their roles, people begin to feel and behave in ways appropriate for “good hypnotic subjects.” They may allow the hypnotist to direct their attention and fantasies away from pain.
dissociation a split in consciousness, which allows some thoughts and behaviors to occur simultaneously with others.
posthypnotic suggestion a suggestion, made during a hypnosis session, to be carried out after the subject is no longer hypnotized; used by some clinicians to help control undesired symptoms and behaviors.
Another theory views hypnosis as a special dual-processing state of dissociation—a split between different levels of consciousness. Dissociation theory offers an explanation for why people hypnotized for pain relief may show brain activity in areas that receive sensory information, but not in areas that normally process pain-related information. It also seeks to explain why, when no one is watching, hypnotized people may carry out posthypnotic suggestions (which are made during hypnosis but carried out after the person is no longer hypnotized) (Perugini et al., 1998).
Another form of dual processing—selective attention—may also play a role in hypnotic pain relief. Brain scans show that hypnosis increases activity in frontal lobe attention systems (Oakley & Halligan, 2013). And it reduces brain activity in a region that processes painful stimuli, but not in the somatosensory cortex, which receives the raw sensory input (Rainville et al., 1997). So, hypnosis does not block sensory input, but it may block our attention to those stimuli. This helps explain why an injured athlete, caught up in the competition, may feel little or no pain until the game ends.
RETRIEVE IT
Question
2Nz7guHN57Qn5E37mFoVtnbig4Ap6CtLqo3ORydohYsnSG8HfTfyQDM5BxMOns1So6saDaeHCAexZa2HVeqGxaTpVz8oPXVyAkou20YjEs40Py095h/ql1OEmLEY4lA83qIwUF5tv7GHvm0TzmjTop0TyUGYfUmsxIjFuWZ5IwN4oTrM
Taste
18-6 In what ways are our senses of taste and smell similar, and how do they differ?
Like touch, our sense of taste involves several basic sensations. Taste’s sensations were once thought to be sweet, sour, salty, and bitter, with all others stemming from mixtures of these four (McBurney & Gent, 1979). Then, as investigators searched for specialized nerve fibers for the four taste sensations, they encountered a receptor for what we now know is a fifth—the savory meaty taste of umami, best experienced as the flavor enhancer monosodium glutamate (MSG).
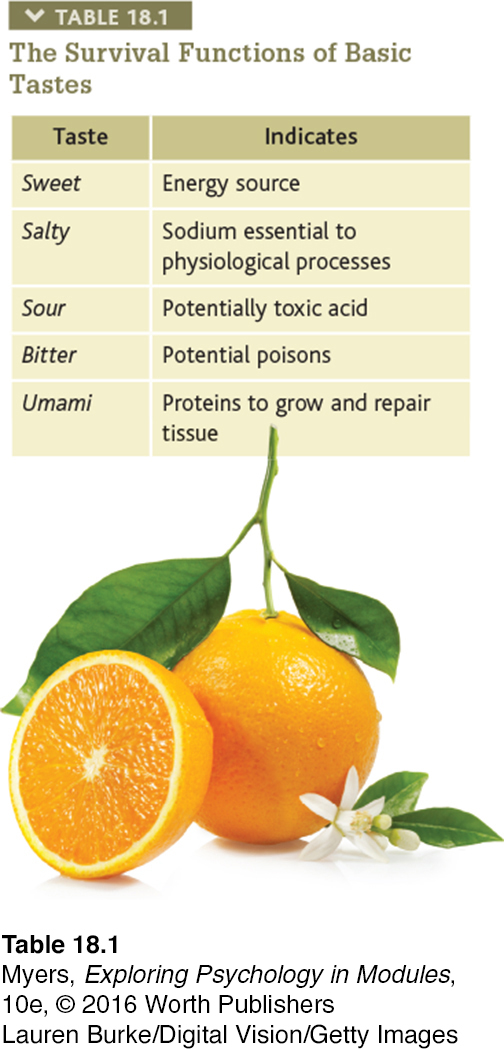
Tastes exist for more than our pleasure (see TABLE 18.1). Pleasureful tastes attracted our ancestors to energy- or protein-rich foods that enabled their survival. Aversive tastes deterred them from new foods that might be toxic. We see the inheritance of this biological wisdom in today’s 2- to 6-year-olds, who are typically fussy eaters, especially when offered new meats or bitter-tasting vegetables, such as spinach and brussels sprouts (Cooke et al., 2003). Meat and plant toxins were both potentially dangerous sources of food poisoning for our ancestors, especially for children. Given repeated small tastes of disliked new foods, however, children begin to accept them (Wardle et al., 2003). We come to like what we eat. Compared with breast-fed babies, German babies bottle-fed vanilla-flavored milk grew up to be adults with a striking preference for vanilla flavoring (Haller et al., 1999).
Taste is a chemical sense. Inside each little bump on the top and sides of your tongue are 200 or more taste buds, each containing a pore that catches food chemicals. Into each taste bud pore, 50 to 100 taste receptor cells project antenna-like hairs that sense food molecules. Some receptors respond mostly to sweet-tasting molecules, others to salty-, sour-, umami-, or bitter-tasting ones, and each has a matching partner cell in the brain (Barretto et al., 2015). It doesn’t take much to trigger a response that alerts your brain’s temporal lobe. If a stream of water is pumped across your tongue, the addition of a concentrated salty or sweet taste for but one-tenth of a second will get your attention (Kelling & Halpern, 1983). When a friend asks for “just a taste” of your soft drink, you can squeeze off the straw after a mere instant.
Taste receptors reproduce themselves every week or two, so if you burn your tongue with hot food it hardly matters. However, as you grow older, the number of taste buds decreases, as does taste sensitivity (Cowart, 1981). (No wonder adults enjoy strong-tasting foods that children resist.) Smoking and alcohol use accelerate these declines. Those who have lost their sense of taste have reported that food tastes like “straw” and is hard to swallow (Cowart, 2005).
“Life is not measured by the number of breaths we take, but by the moments that take our breath away.”
Essential as taste buds are, there’s more to taste than meets the tongue. Expectations can influence taste. When told a sausage roll was “vegetarian,” people in one experiment found it decidedly inferior to its identical partner labeled “meat” (Allen et al., 2008). In another experiment, being told that a wine cost $90 rather than its real $10 price made it taste better and triggered more activity in a brain area that responds to pleasant experiences (Plassmann et al., 2008).
Smell
Life begins with an inhale and ends with an exhale. Between birth and death, we will, on average, inhale and exhale 500 million breaths of life-sustaining air, bathing our nostrils in a stream of scent-laden molecules. The resulting experiences of smell (olfaction) are strikingly intimate: You inhale something of whatever or whoever it is you smell.
Impress your friends with your new word for the day: People unable to see are said to experience blindness. People unable to hear experience deafness. People unable to smell experience anosmia. The 1 in 7500 people born with anosmia not only have trouble cooking and eating, but also are somewhat more prone to depression, accidents, and relationship insecurity (Croy et al., 2012, 2013).
Like taste, smell is a chemical sense. We smell something when molecules of a substance carried in the air reach a tiny cluster of 20 million receptor cells at the top of each nasal cavity (FIGURE 18.9). These olfactory receptor cells, waving like sea anemones on a reef, respond selectively—to the aroma of a cake baking, to a wisp of smoke, to a friend’s fragrance. Instantly, they alert the brain through their axon fibers. Being part of an old, primitive sense, olfactory neurons bypass the brain’s sensory control center, the thalamus.
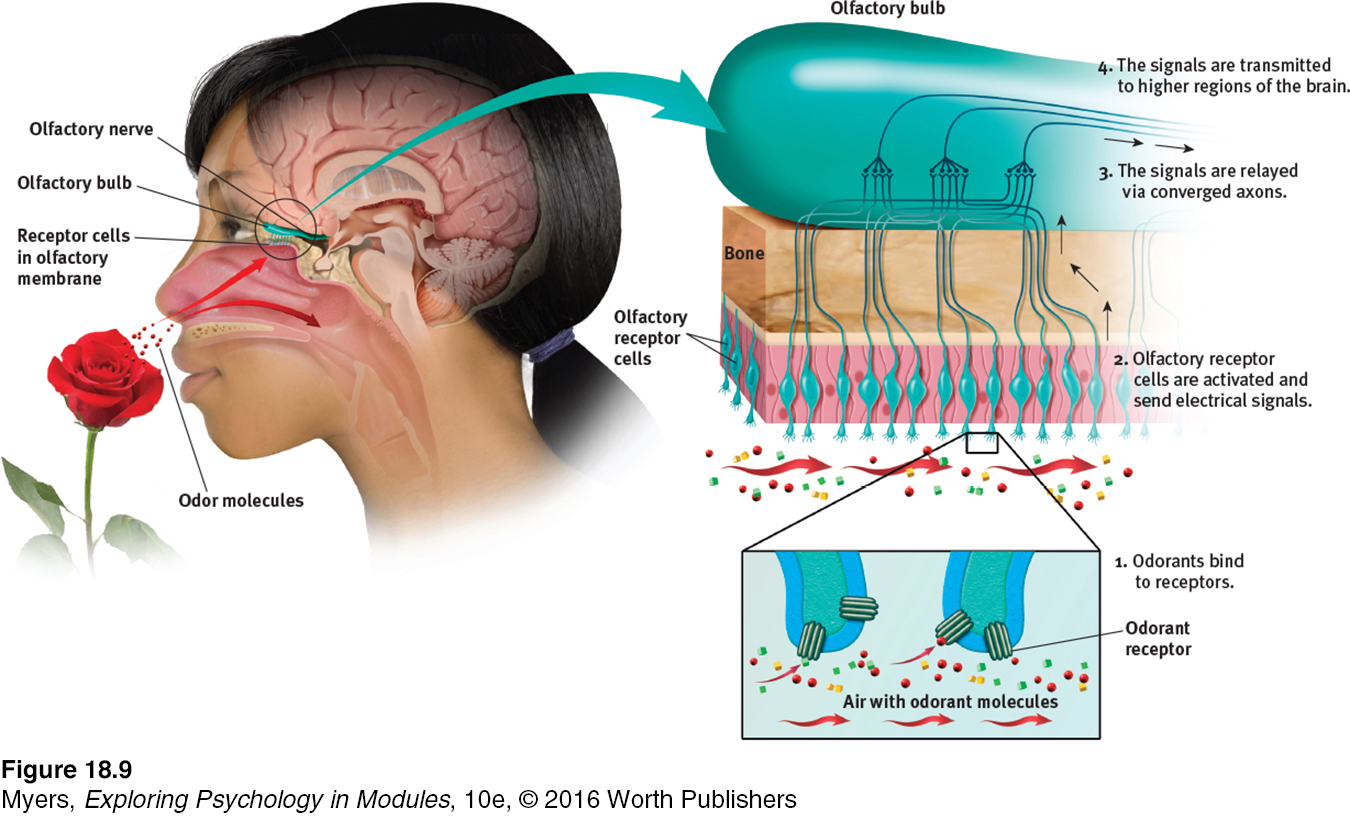
Figure 6.45: FIGURE 18.9 The sense of smell If you are to smell a flower, airborne molecules of its fragrance must reach receptors at the top of your nose. Sniffing swirls air up to the receptors, enhancing the aroma. The receptor cells send messages to the brain’s olfactory bulb, and then onward to the temporal lobe’s primary smell cortex and to the parts of the limbic system involved in memory and emotion.
 For an animated explanation of how we smell, visit LaunchPad’s Concept Practice: Sense of Smell.
For an animated explanation of how we smell, visit LaunchPad’s Concept Practice: Sense of Smell.
Even nursing infants and their mothers have a literal chemistry to their relationship. They quickly learn to recognize each other’s scents (McCarthy, 1986). Aided by smell, a mother fur seal returning to a beach crowded with pups will find her own. Our human sense of smell is less acute than our senses of seeing and hearing. Looking out across a garden, we see its forms and colors in exquisite detail and hear a variety of birds singing, yet we smell little of it without sticking our nose into the blossoms.
Odor molecules come in many shapes and sizes—so many, in fact, that it takes many different receptors to detect them. A large family of genes designs the 350 or so receptor proteins that recognize particular odor molecules (Miller, 2004). Linda Buck and Richard Axel (1991) discovered (in work for which they received a 2004 Nobel Prize) that these receptor proteins are embedded on the surface of nasal cavity neurons. As a key slips into a lock, so odor molecules slip into these receptors. Yet we don’t seem to have a distinct receptor for each detectable odor. Odors trigger combinations of receptors, in patterns that are interpreted by the olfactory cortex. As the English alphabet’s 26 letters can combine to form many words, so odor molecules bind to different receptor arrays, producing at least 1 trillion odors that we could potentially discriminate (Bushdid et al., 2014). It is the combinations of olfactory receptors, which activate different neuron patterns, that allow us to distinguish between the aromas of fresh-brewed and hours-old coffee (Zou et al., 2005).

The nose knows Humans have some 20 million olfactory receptors. A bloodhound has 220 million (Herz, 2007).
Layne Bailey/The Charlotte Observer/AP Photo
For humans, the attractiveness of smells depends on learned associations (Herz, 2001). As babies nurse, their preference for the smell of their mother’s breast builds. So, too, with other associations. As good experiences are linked with a particular scent, people come to like that scent. This helps explain why people in the United States tend to like the smell of wintergreen (which they associate with candy and gum) more than do those in Great Britain (where it often is associated with medicine). In another example of odors evoking unpleasant emotions, researchers frustrated Brown University students with a rigged computer game in a scented room (Herz et al., 2004). Later, if exposed to the same odor while working on a verbal task, the students’ frustration was rekindled and they gave up sooner than others exposed to a different odor or no odor.
Our sensory experiences also interact with other aspects of our psychology. Our brain’s circuitry helps explain an odor’s power to evoke feelings and memories (FIGURE 18.10). A hotline runs between the brain area receiving information from the nose and the brain’s ancient limbic centers associated with memory and emotion. Thus, when put in a foul-smelling room, people expressed harsher judgments of immoral acts (such as lying or keeping a found wallet) and more negative attitudes toward gay men (Inbar et al., 2011; Schnall et al., 2008). Exposed to a fishy smell during a trust game, people became more suspicious (Lee & Schwarz, 2012). And when exposed to a sweet taste, people became sweeter on their romantic partners and sweeter to others by acting more helpful (Meier et al., 2012; Ren et al., 2015).
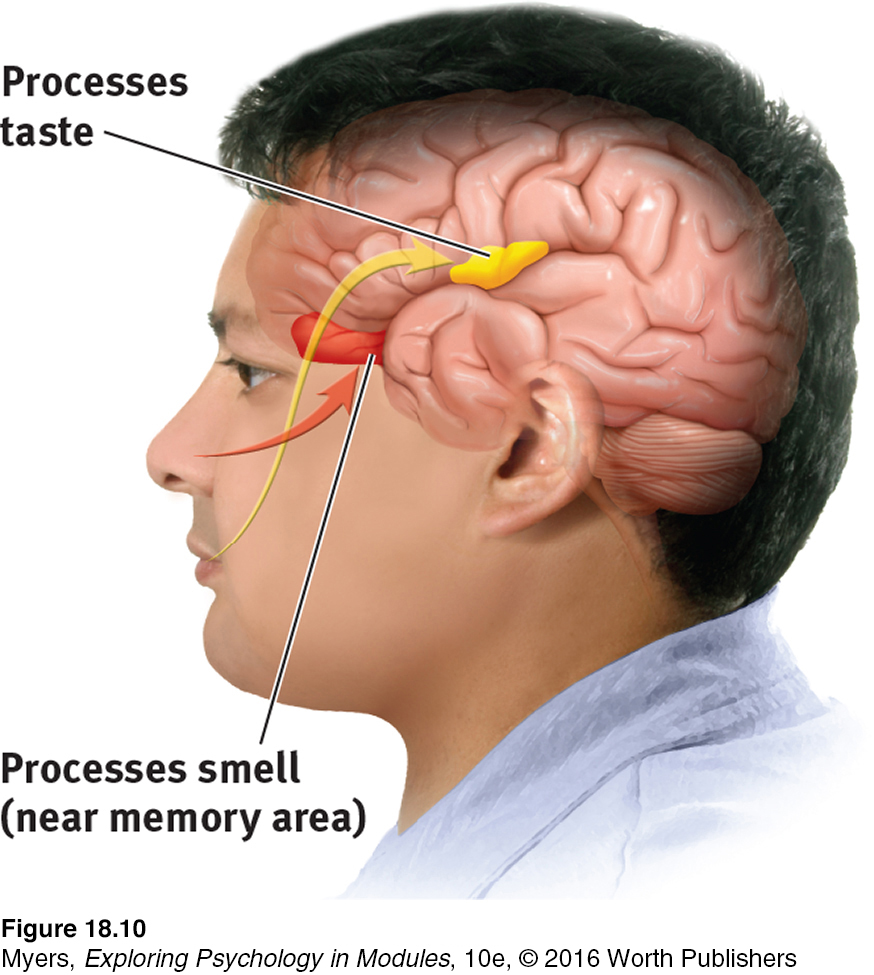
Figure 6.46: FIGURE 18.10 Taste, smell, and memory Information from the taste buds (yellow arrow) travels to an area between the frontal and temporal lobes of the brain. It registers in an area not far from where the brain receives information from our sense of smell, which interacts with taste. The brain’s circuitry for smell (red area) also connects with areas involved in memory storage, which helps explain why a smell can trigger a memory.
Though it’s difficult to recall odors by name, we can easily recognize long-forgotten odors and their associated memories (Engen, 1987; Schab, 1991).
RETRIEVE IT
Question
OXlfLvcSr0YwuqRvm3IVnVr4Tiw/bB/LMHizIYadipRS/QQupBOe6ryUKTdN2iL+bRCnsaeGTRxHG1PYtSFY8+T7v/BqtJC12wf8QzhqjjXAiZ0eT8JNWy4Y6au71E1z
ANSWER: We have four basic touch senses and five basic taste sensations. But we have no specific smell receptors. Instead, different combinations of odor receptors send messages to the brain, enabling us to recognize some 1 trillion different smells.
