Six Major Categories of Mental Disorders
As you read this section, beware of the “medical school syndrome”—the tendency to think that you have a disease (disorder in our case) when you read about its symptoms. Symptoms are behaviors or mental processes that indicate the presence of a disorder. The symptoms of many disorders often involve behavior and thinking that we all experience, which may lead us to think we have the disorders. To prevent such misdiagnoses, remember the criteria that we discussed for distinguishing abnormal behavior and thinking. For example, we all get anxious or depressed (symptoms of several different disorders) at different times in our lives for understandable reasons, such as an upcoming presentation or a death in the family. These feelings of anxiety and depression only become symptoms of a disorder when they prevent us from functioning normally. We are suffering from a disorder only if our reactions to life’s challenges become atypical, maladaptive, disturbing to ourselves or others, and irrational.
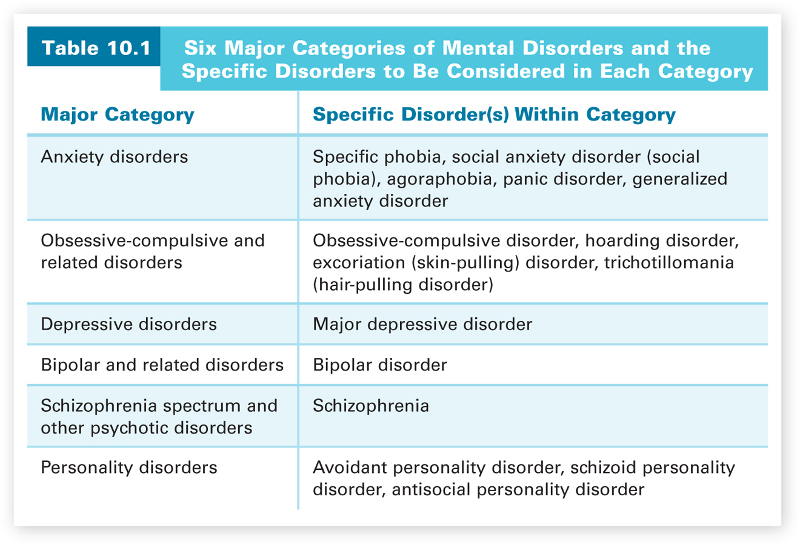
What causes such abnormal behavior and thinking? Most causal explanations for mental disorders are tied to the four major research approaches—biological, behavioral, cognitive, and sociocultural. None of these approaches has proven consistently better at explaining all of the various disorders, though particular approaches are sometimes better for specific disorders. Even in these cases, however, it appears best to formulate an explanation in terms of more than one kind of cause. This is usually referred to as the biopsychosocial approach—explaining abnormality as the result of the interaction among biological, psychological (behavioral and cognitive), and sociocultural factors. As we consider various disorders, we will provide some examples of this type of explanation. Table 10.1 outlines the six major categories of disorders, along with the specific mental disorders within each category that we will consider.
403
Anxiety Disorders
We all have experienced anxiety. Don’t you get anxious at exam times, especially at final exam time? Most students do. How do you feel when you are about to give an oral presentation? Anxiety usually presents itself again. These are normal reactions, not signs of a disorder. Anxiety disorders are disorders that share features of excessive fear and anxiety and related behavioral disturbances, such as avoidance behaviors (APA, 2013). In anxiety disorders, the anxiety and fear often occur inexplicably and are so intense that they prevent the person from functioning normally in daily life. The specific anxiety disorders differ from one another in the types of objects and situations that induce the excessive fear and anxiety. Because anxiety disorders are some of the most common disorders in the United States (Hollander & Simeon, 2011; cf. Horwitz & Wakefield, 2012), we’ll discuss several different anxiety disorders—specific phobia, social anxiety disorder (social phobia), agoraphobia, panic disorder, and generalized anxiety disorder.
Specific phobia.
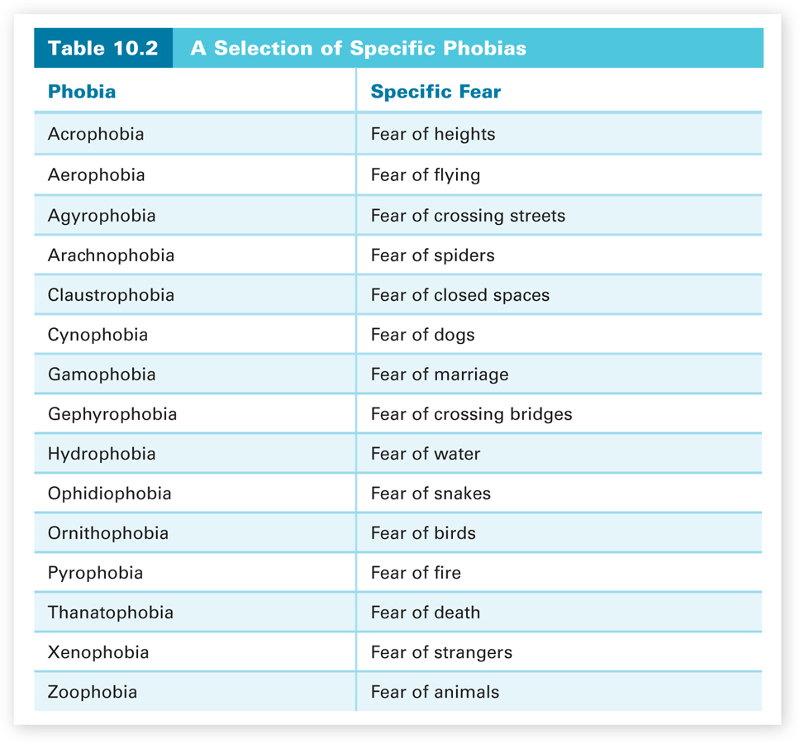
According to the DSM-5, a specific phobia is indicated by a marked and persistent fear of specific objects or situations (such as snakes or heights) that is excessive and unreasonable. In the United States, the overall prevalence rate for specific phobia ranges from 7 to 9 percent, with a higher prevalence rate in teenagers and a lower prevalence rate in older adults (APA, 2013). More than 12 percent of people in the United States develop a specific phobia at some point during their lives, and having a specific phobia is about twice as prevalent in women versus men and in African and Hispanic Americans (born in the United States) versus White Americans (Comer, 2014). A selection of specific phobias is given in Table 10.2. A person with a specific phobia realizes that the fear is excessive and unreasonable but cannot control it. Both the avoidance of the object or situation and the anxious anticipation of encountering the object or situation interfere with the person’s daily life. This is important. Many of us have fears of such things as heights, snakes, and spiders, but we do not have a disorder. The anxiety and fear are not to the degree that they interfere with normal functioning and lead us to behave in maladaptive and irrational ways.
404
To emphasize this difference, consider this brief description of a case of a woman with a specific phobia of birds. She became housebound because of her fear of encountering a bird. Any noises that she heard within the house she thought were birds that had somehow gotten in. Even without encountering an actual bird, the dreaded anticipation of doing so completely controlled her behavior. When she did leave her house, she would carefully back out of her driveway so that she did not hit a bird; she feared that the birds would retaliate if she did. She realized that such cognitive activity was beyond the capabilities of birds, but she could not control her fear. Her behavior and thinking were clearly abnormal.
405

What causes a specific phobia? One biopsychosocial answer involves both behavioral and biological factors. We learn phobias through classical conditioning and are biologically predisposed to learn some fears more easily than others. We are conditioned to fear a specific object or situation. Remember Watson and Rayner’s study described in Chapter 4 in which they classically conditioned Little Albert to fear white rats? Behavioral psychologists believe that the fears in specific phobias are learned the same way, but through stressful experiences in the real world, especially during early childhood. For example, a fear of birds might be due to the stressful experience of seeing Alfred Hitchcock’s movie The Birds (in which birds savagely attack humans) at a young age. You should also remember from Chapter 4 that biological preparedness constrains learning. Certain associations (such as taste and sickness) are easy to learn, while others (such as taste and electric shock) are very difficult. This biological preparedness shows up with specific phobias in that fears that seem to have more evolutionary survival value (such as fears of heights and animals) are more frequent than ones that do not (McNally, 1987). It is also more difficult to extinguish fears that have more evolutionary survival value (Davey, 1995).
Social anxiety disorder (social phobia) and agoraphobia.
Most phobias are classified as specific phobias, but the DSM-5 describes two broader types of phobias: social anxiety disorder (previously labeled social phobia in the DSM-IV) and agoraphobia. Social anxiety disorder is a marked, irrational, and persistent fear of one or more social performance situations in which embarrassment may occur and in which there is exposure to unfamiliar people or scrutiny by others. Again this is more than the normal anxiety before giving a presentation. The fear is excessive, unreasonable, and interferes with the person’s normal functioning. For example, the person may fear eating in public and will have great difficulty managing lunch at work; she will reject all lunch and dinner invitations, greatly limiting her social opportunities. The fear may be specific to one particular social situation (such as eating in public) or more general (such as functioning inadequately with respect to all behavior in front of others), leading to the avoidance of most social situations.
406

Social anxiety disorder is different from agoraphobia, the fear of being in places or situations from which escape may be difficult or embarrassing. The name of this disorder literally means fear of the market-place; in Greek, “agora” means marketplace, and “phobia” means fear. In addition to the marketplace, situations commonly feared in agoraphobia include being in a crowd, standing in a line, and traveling in a crowded bus or train or in a car in heavy traffic. To avoid these situations, people with agoraphobia usually won’t leave the security of their home. Surveys reveal that about 7 percent of people in the United States suffer from social anxiety disorder in any given year but only about 2 percent from agoraphobia (Kessler, Ruscio, Shear, & Wittchen, 2010; NIMH, 2011). Just as for specific phobias, a behavioral-evolutionary explanation seems indicated for agoraphobia. However, the leading explanation for social anxiety disorder is cognitive—people with this disorder have negative social beliefs about themselves, such as that they are socially inadequate and that their behavior in social situations will inevitably lead to disasters (e.g., Heimberg, Brozovich, & Rapee, 2010; Rosenberg, Ledley, & Heimberg, 2010). Anticipating that such disasters will occur, people with social anxiety disorder try to avoid social situations; and when they are in a social situation, they suffer increased anxiety, which leads to a negative assessment of how poorly they have acted, increasing their fear of future social situations.
Panic disorder.
Panic disorder is a condition in which a person experiences recurrent panic attacks—sudden onsets of intense fear. A panic attack includes symptoms such as trembling, sweating, heart palpitations, chest pain, shortness of breath, and feelings of choking and dizziness. The person is overrun with anxiety and fear. Some panic attacks occur when a person is faced with a dreaded situation (such as going to the dentist), but others occur without any apparent reason. Only about 2 to 3 percent of adolescents and adults suffer from panic disorder each year, and it is twice as common in women as in men (APA, 2013).
Biological explanations of panic disorder involve abnormal neurotransmitter activity, especially that of norepinephrine, and improper functioning of a panic brain circuit, which includes the amygdala, hypothalamus, and some other areas in the brain. Cognitive explanations involve panic-prone people who are overly sensitive to bodily sensations. Such people misinterpret these sensations as signs of a medical catastrophe, plunging them into a panic attack. Panic disorder is also often accompanied by agoraphobia. One explanation of panic disorder with agoraphobia is the fear-of-fear hypothesis: Agoraphobia is the result of the fear of having a panic attack in a public place. According to this hypothesis, agoraphobia is a case of classical conditioning in which the fear-avoidance response is a conditioned response to the initial panic attack.
407
Generalized anxiety disorder.
Panic attacks occur suddenly in panic disorder. In generalized anxiety disorder, the anxiety is chronic and lasts for months. Generalized anxiety disorder is a disorder in which a person has excessive, global anxiety that he cannot control, occurring more days than not for at least six months (APA, 2013). The person just cannot stop worrying, and the anxiety is general—it is not tied to specific objects or situations as it is in a phobic disorder. The problem is sometimes described as free-floating anxiety. About 6 percent of us will develop a generalized anxiety disorder in our lifetimes, and it is diagnosed twice as often in women than men (APA, 2013). Recent biological research has indicated that generalized anxiety disorder may be related to a biochemical dysfunction in the brain involving GABA, a neurotransmitter that we discussed in Chapter 2. Remember, GABA is the major inhibitory neurotransmitter, which means that it causes neurons to stop generating impulses. In anxiety and fear situations, more and more neurons get excited. After a while, this state of excitability in a normal person triggers the release of GABA to reduce the level of neuronal firing back to normal, which reduces the feelings of anxiety. A person with generalized anxiety disorder may have problems activating GABA, and therefore the feelings of anxiety are not reduced.
Obsessive-Compulsive and Related Disorders
This is a new major category in the DSM-5. In the DSM-IV, obsessive-compulsive disorder was classified as an anxiety disorder. In this new category, obsessive-compulsive disorder is grouped with some related disorders, such as excoriation (skin-picking) disorder and trichotillomania (hair-pulling) disorder. These disorders are related to obsessive-compulsive disorder because of the compulsive nature of the behaviors involved and the obsessive-like concerns that trigger these behaviors. We will focus our discussion on obsessive-compulsive disorder and then briefly describe a few of the related disorders. None of the disorders in this category is as prevalent as the anxiety disorders that we discussed.
408
Obsessive-compulsive disorder.
A person with obsessive-compulsive disorder experiences recurrent obsessions or compulsions that are recognized by the person as excessive or unreasonable, but consume considerable time and cause significant distress and disruption in the person’s daily life. Some people with obsessive-compulsive disorder experience only obsessions or only compulsions, but most suffer both. An obsession is a persistent intrusive thought, idea, impulse, or image that causes anxiety. A compulsion is a repetitive and rigid behavior that a person feels compelled to perform in order to reduce anxiety. The most common obsessions are concerned with contamination through germs, dirt, or other toxic substances, and the fear that something terrible, such as death or illness, is going to occur; the most frequent compulsions are excessive hand washing, bathing, and grooming (Rapoport, 1989). The 12-month prevalence of obsessive-compulsive disorder is only 1.2 percent (APA, 2013).
It is important to realize that many people experience minor obsessions (e.g., a pervasive worry about upcoming exams) or compulsions (e.g., arranging their desks in a certain way), but they do not have this disorder. People with obsessive-compulsive disorder cannot function in their daily lives, because their obsessions and compulsions consume most of the day and prevent a normal life. People who don’t have this disorder might go back to check to make sure that the stove was turned off once (or even twice), but a person with an obsessive-compulsive disorder might check 50 times and in a very ritualistic manner. This is a checking compulsion—the person checks the same thing over and over again, usually a set number of times and in a particular manner. Similarly, people who suffer from a cleaning compulsion feel compelled to keep cleaning themselves. Such people might spend their day washing their hands, taking showers, and engaging in other cleaning activities. Compulsions are usually tied to obsessions. For example, the cleaning compulsion is usually tied to a contamination obsession in which people are overly concerned with avoiding contamination. To reduce the anxiety stemming from the fear of contamination, they feel compelled to keep cleaning themselves.
409
It is not known for sure what causes obsessive-compulsive disorder, but recent research suggests that a neurotransmitter imbalance involving serotonin may be involved. Antidepressant drugs that only increase serotonin activity (SSRIs) help many patients with obsessive-compulsive disorder (Rapoport, 1991). Serotonin activity has also been linked to parts of the brain that may be related to the disorder—the orbital region of the frontal cortex (the cortical area just above the eyes), the caudate nuclei (areas in the basal ganglia), the thalamus, the amygdala, and the cingulate cortex (the communication conduit between the prefrontal lobes and the limbic system). These parts comprise a brain circuit that is involved in filtering out irrelevant information and disengaging attention, which are certainly central aspects of obsessive-compulsive disorder (Seligman, Walker, & Rosenhan, 2001). One explanation may be that serotonin works to stabilize activity in these areas. One truly bizarre case of obsessive-compulsive disorder high-lights the importance of the frontal lobe region. A man with obsessive-compulsive disorder became severely depressed and attempted suicide. He shot himself in the head, but fortunately survived and was cured of his disorder. The bullet had removed some of his orbital frontal cortex and his disorder with it.
Obsessive-compulsive related disorders.
We will briefly describe three of these disorders—hoarding disorder, excoriation (skin-picking) disorder, and trichotillomania (hair-pulling disorder). At present, explanations for these related disorders are similar to those we discussed for obsessive-compulsive disorder. It is hoped that by being grouped with obsessive-compulsive disorder in the DSM-5, these disorders will be researched more, leading to more disorder-specific explanations.
Hoarding disorder reflects a persistent difficulty in discarding or parting with possessions due to a perceived need to save the items and the distress associated with discarding them. This need to save items results in an extraordinary accumulation of clutter. Parts of the home may become inaccessible because of the stacks of clutter occupying those areas. Sofas, beds, and other pieces of furniture may be unusable, because they are filled with stacks of hoarded items. Such clutter may not only impair personal and social functioning but also result in fire hazards and unhealthy sanitary conditions. Prevalence rates for hoarding disorder are not available, but it appears to be more prevalent in older adults than younger adults (APA, 2013). About 75 percent of individuals with hoarding disorder also have an anxiety or depressive disorder, with the most common being major depressive disorder (APA, 2013). Having another disorder is important, because it may often be the main reason for consultation. Individuals with hoarding disorder seldom seek consultation for hoarding symptoms.
People with excoriation (skin-picking) disorder keep picking at their skin, leading to sores and other skin problems, as well as, in some cases, lesions. Most people with this disorder pick with their fingers and center their focus on one area of the body, most often the face. However, other areas, such as the arms and legs, are also common focal points for this disorder. The skin-picking is usually triggered and accompanied by anxiety and stress. People with excoriation disorder often spend significant amounts of time on their picking behavior, sometimes several hours per day. The lifetime prevalence for excoriation is only 1 to 2 percent, and 75 percent or more of the people with this disorder are women (APA, 2013).
410
People with trichotillomania (hair-pulling disorder) continually pull out hair from the scalp or other areas of the body. The hair-pulling typically is only focused on one body part, most often the scalp, eyebrows, or eyelids, and done one hair at a time, sometimes in a ritualistic manner. Like excoriation, trichotillomania is triggered and accompanied by anxiety or stress. The hair-pulling may occur in brief episodes throughout the day or during less frequent but more sustained periods that can continue for hours. Women are more frequently affected with trichotillomania than men, at a ratio of approximately 10 to 1 (APA, 2013).
Depressive Disorders
Depressive disorders involve the presence of sad, empty, or irritable mood, accompanied by somatic and cognitive changes that significantly affect the individual’s capacity to function. Major depressive disorder (sometimes called unipolar depression) represents the classic condition in this category, so it is the depressive disorder that we will discuss.
Major depressive disorder.
When people say that they are depressed, they usually are referring to their feelings of sadness and downward mood following a stressful life event (such as the breakup of a relationship or the loss of a job). Such mood changes are understandable and over time usually right themselves. A major depressive disorder, however, is debilitating, has an impact on every part of a person’s life, and usually doesn’t right itself. To be classified as having a major depressive disorder, a person must have experienced one or more major depressive episodes. A major depressive episode is characterized by symptoms such as feelings of intense hopelessness, low self-esteem, and worthlessness; extreme fatigue; dramatic changes in eating and sleeping behavior; inability to concentrate; and greatly diminished interest in family, friends, and activities for a period of two weeks or more. Such people are not just down in the dumps, but rather are in a snowballing downward spiral that lasts for weeks. They lose interest in everything, even their life. Suicide is strongly related to depression and can occur at any point during or after a major depressive episode. Any comments about suicide made by people suffering a major depression should be taken seriously.
The 12-month prevalence is 7 percent, but this prevalence in the 18 to 29 age group is three times greater than that in individuals age 60 years or older (APA, 2013). Major depressive disorder is also more common among poor people than wealthy people (Sareen, Afifi, McMillan, & Asmundson, 2011). About 19 percent of all adults suffer a major depressive disorder at some point in their lives. Women suffer from major depressive disorders about twice as often as men (Kessler et al., 2003), and this gender difference seems to be true worldwide (Weissman et al., 1996). Recent research suggests that this gender difference for depression may be due to biological differences (Westly, 2010). The sex hormones estrogen and testosterone have different effects on the neurotransmitters involved in mood (serotonin, norepinephrine, and dopamine), leading to a difference in both emotional reaction and symptomology in women and men. The primary emotional symptom for women is sadness; but for men, it is anger often paired with irritability. Thus, female depression will be seen as depression, but male depression may be mistakenly seen as some other emotional problem, such as general frustration, and not the serious disorder that it is. This difference, along with the fact that women are more likely than men to seek help, almost certainly contributes to the gender difference in the clinical prevalence rates for depression.
411
There is also a recent argument that the high prevalence rate for depression is spurious, in that it is due to overdiagnosis caused by insufficient diagnostic criteria (Horwitz & Wakefield, 2007). True mental disorders are usually rare, with very low prevalence rates, but depression has a high prevalence rate. According to Andrews and Thomson (2009, 2010), the fact that depression has a high prevalence rate poses an evolutionary paradox, because the pressures of evolution should have led our brains to resist such a high rate of malfunction. Andrews and Thomson propose that much of what is diagnosed as depression should not be thought of as a true mental disorder (a brain malfunction) but rather as an evolutionary mental adaptation (stress response mechanism) that focuses the mind to better solve the complex life problems that brought about the troubled state. This is an intriguing hypothesis with implications not only for the diagnostic criteria for this disorder but also for the therapeutic approaches to treat it.
Traditional explanations of major depressive disorder propose both biological and psychological factors as causes. A leading biological explanation involves neurotransmitter imbalances, primarily inadequate serotonin and norepinephrine activity. Antidepressant drugs (to be discussed later in the chapter) are the most common treatment for such imbalances. There is also evidence of a genetic predisposition for this disorder. The likelihood of one identical twin getting a disorder given that the other identical twin has the disorder is the concordance rate for identical twins for the disorder. For major depressive disorder, the concordance rate for identical twins is about 50 percent (Tsuang & Faraone, 1990), much higher than the concordance rate for fraternal twins and the base rate of occurrence in the general population.
If the disorder were totally genetic in origin, however, this rate would be 100 percent. Because it isn’t, nongenetic factors are also seen as causes in major depressive disorder. Cognitive factors have been found to be important. The person’s perceptual and cognitive processes are assumed to be faulty, causing the depression. We discussed an example of such faulty cognitive processing in Chapter 8. Remember the pessimistic explanatory style in which a person explains negative events in terms of internal (her own fault), stable (here to stay), and global (applies to all aspects of her life) causes. Such a style, paired with a series of negative events in a person’s life, will lead to learned helplessness and depression. Thus, the cause of the person’s depression is her own thinking, in this case how she makes attributions. Cognitive therapies, which we will discuss later in this chapter, attempt to replace such maladaptive thinking with more adaptive thinking that will not lead to depression. These therapies have been shown to be just as effective as drug therapy in treating depression (DeRubeis et al., 2005).
412
Bipolar and Related Disorders
Major depressive disorder is often referred to as unipolar depression or a unipolar disorder to contrast it with bipolar disorder, another disorder in which the person’s mood takes dramatic mood swings between depression and mania. Such disorders used to be called “manic-depressive” disorders. Experiencing a mania is not just having an “up” day. A manic episode is a period of at least a week of abnormally elevated mood in which the person experiences such symptoms as inflated self-esteem with grandiose delusions, a decreased need for sleep, constant talking, distractibility, restlessness, and poor judgment. The person’s behavior becomes maladaptive and interferes with daily functioning.

Consider the following behavior of a person experiencing a manic episode. A postal worker stayed up all night and then went off normally to work in the morning. He returned later that morning, however, having quit his job, withdrawn all of the family savings, and spent it on fish and aquariums. He told his wife that, the night before, he had discovered a way to keep fish alive forever. He then ran off to canvass the neighborhood for possible sales. This person showed poor judgment and a decreased need for sleep, and his behavior disrupted his normal functioning (he quit his job). In the beginning, milder stages of a manic episode, some people become not only more energetic but also more creative, until the episode accelerates and their behavior deteriorates.
There is no diagnosis for mania alone. It is part of a bipolar disorder in which recurrent cycles of depressive and manic episodes occur. A bipolar disorder is an emotional roller coaster, with the person’s mood swinging from manic highs to depressive lows. There are two types of bipolar disorder. In Bipolar I disorder, the person has both major manic and depressive episodes. In Bipolar II disorder, the person has full-blown depressive episodes, but the manic episodes are milder. Bipolar I disorder is more common than Bipolar II disorder, but both disorders are rare and only affect less than 1 percent of the population (APA, 2013; Kessler et al., 1994).
413
Because the concordance rate for identical twins for bipolar disorder is so strong, 70 percent (Tsuang & Faraone, 1990), biological causal explanations are the most common. In fact, researchers are presently working on identifying the specific genes that make a person vulnerable to bipolar disorder. As with major depressive disorder, the biological predisposition shows up as neurotransmitter imbalances. In this case, the imbalances swing between inadequate activity (depression) and too much activity (mania). The most common treatment is drug therapy, and the specific drugs used will be discussed later in the chapter.
Schizophrenia Spectrum and Other Psychotic Disorders
We will only be discussing schizophrenia from this category. It is the disorder that people are usually thinking of when they use words such as “insane” and “deranged.” More people are institutionalized with schizophrenia than with any other disorder, and schizophrenia is much more difficult to successfully treat than other mental disorders. Thankfully, only about 1 percent of the population suffers from this disorder (Gottesman, 1991). The onset of schizophrenia is usually in late adolescence or early adulthood. Men and women are equally likely to develop schizophrenia, but it tends to strike men earlier and more severely (Lindenmayer & Khan, 2012). Schizophrenia is more common in the lower socioeconomic classes than in the higher ones, and also for those who are single, separated, or divorced (Sareen, Afifi, McMillan, & Asmundson, 2011). In addition, people with schizophrenia have an increased risk of suicide with an estimated 25 percent attempting suicide (Kasckow, Felmet, & Zisook, 2011).
Schizophrenia is referred to as a psychotic disorder, because it is characterized by a loss of contact with reality. The word “schizophrenia” is Greek in origin and literally means “split mind.” This is not a bad description; in a person with schizophrenia, mental functions become split from each other and the person becomes detached from reality. The person has trouble distinguishing reality from his own distorted view of the world. This splitting of mental functions, however, has led to the confusion of schizophrenia with “split personality” or multiple personality disorder (now called dissociative identity disorder in the DSM-5), but these are very different disorders. In schizophrenia, the split is between the mental functions and their contact with reality; in multiple personality disorder, one’s personality is split into two or more distinct personalities.
The symptoms of schizophrenia.
The symptoms of schizophrenia vary greatly, but they are typically divided into three categories—positive, negative, and disorganized. This use of the terms “positive” and “negative” is consistent with their use in Chapter 4, on learning. Positive means that something has been added, and negative means that something has been removed.
414
Positive symptoms are the more active symptoms that reflect an excess or distortion of normal thinking or behavior, including hallucinations (false sensory perceptions) and delusions (false beliefs). Hallucinations are usually auditory, hearing voices that aren’t really there. Remember, the fake patients in Rosenhan’s study said that they heard voices and were admitted and diagnosed as having a schizophrenic disorder. Delusions fall into several categories, such as delusions of persecution (for example, believing that one is the victim of conspiracies) or delusions of grandeur (for example, believing that one is a person of great importance, such as Jesus Christ or Napoleon). Hallucinations and delusions are referred to as positive symptoms because they refer to things that have been added. Negative symptoms refer to things that have been removed. These are deficits or losses in emotion, speech, energy level, social activity, and even basic drives such as hunger and thirst. For example, many people with schizophrenia suffer a flat affect in which there is a marked lack of emotional expressiveness. Their faces show no expression, and they speak in a monotone. Similarly, there may be a serious reduction in their quantity and quality of speech. People suffering from schizophrenia may also lose their energy and become extremely apathetic—not able to start a task, much less finish one.
Disorganized symptoms include nonsensical speech and behavior and inappropriate emotion. Disorganized speech sounds like a “word salad,” with unconnected words incoherently spoken together and a shifting from one topic to another without any apparent connections. One thought does not follow the other. Those who show inappropriate emotion may smile when given terrible news. Their emotional reactions seem unsuited to the situation.
Behavior may also be catatonic—physical actions that do not appear to be goal-directed, such as assuming and maintaining postures and remaining motionless for a long period of time. Catatonic behavior takes extreme forms ranging from immobility to hyperactivity (such as rocking constantly).
According to the DSM-5, schizophrenia is the presence, most of the time during at least a one-month period, of at least two of the following symptoms—hallucinations, delusions, disorganized speech, grossly abnormal psychomotor activity (including catatonic behavior), or any negative symptom (such as loss of emotion). In addition, functioning in daily life is markedly below that prior to the onset of the symptoms, and the signs of this disturbance must occur for at least six months, including the period of at least one month when at least two of the symptoms are present.
Clinicians have used the various types of symptoms of schizophrenia and their course of development to make distinctions between types of schizophrenia. One such distinction between chronic and acute schizophrenia deals with how quickly the symptoms developed. In chronic schizophrenia, there is a long period of development, over years, and the decline in the person’s behavior and thinking occurs gradually. In acute schizophrenia, there is a sudden onset of symptoms that usually can be attributed to a crisis in the person’s life, and the person functioned normally before the crisis with no clinical signs of the disorder. Acute schizophrenia is more of a reactive disorder, and recovery is much more likely.
415
Another distinction is between Type I and II schizophrenia (Crow, 1985). Type I is characterized by positive symptoms, and Type II by negative symptoms. Type I is similar to acute schizophrenia: The person has usually functioned relatively normally before the disorder strikes, and there is a higher likelihood of recovery. People with Type I schizophrenia respond better to drug therapy than do those with Type II. This difference may be because the positive symptoms of Type I result from neurotransmitter imbalances, which are affected by drugs, whereas the more permanent structural abnormalities in the brain that produce the negative symptoms of Type II are not as affected by drugs.
The causes of schizophrenia.
Schizophrenia seems to have many different causes, and we do not have a very good understanding of any of them. Hypothesized causes inevitably involve a genetic or biological predisposition factor. There definitely appears to be a genetic predisposition to some schizophrenia; it seems to run in families, with the concordance rate for identical twins similar to that for a major depression, about 50 percent (DeLisi, 1997; Gottesman, 1991). This is significantly greater than the 17 percent concordance rate for fraternal twins. No particular genes have yet been identified, but it is possible that different genes might be involved in the different types of schizophrenia or that schizophrenia is a polygenic disorder caused by a combination of gene defects (e.g., Sanders, Duan, & Gejman, 2012).
The concordance rate for identical twins could also be partially due to prenatal factors (Brown, 2006). One hypothesis involves prenatal viral infections. Research has found that people are at increased risk for schizophrenia if there was a flu epidemic during the middle of their fetal development (Takei, Van Os, & Murray, 1995; Wright, Takei, Rifkin, & Murray, 1995). There is even a birth month effect for schizophrenia. People born in the winter/spring months (January to April) following the fall/winter flu season are more likely to develop schizophrenia, because it is more likely that they were exposed to a flu virus during fetal development (Torrey, Miller, Rawlings, & Yolken, 1997). According to the viral hypothesis, the invading virus impairs fetal brain development, making people more susceptible to developing schizophrenia later in life. The viral hypothesis is further supported by the finding that the 50 percent concordance rate in identical twins is the result of a 60 percent chance for identical twins that share the same placenta (about two-thirds of identical twins), but only a 10 percent chance for identical twins with separate placentas (Davis & Phelps, 1995). It is certainly more likely that a viral infection would affect both twins in the same placenta rather than twins in separate placentas.
Prenatal or early postnatal exposure to several other viruses (e.g., herpes simplex virus) has also been associated with the later development of schizophrenia (Yolken & Torrey, 1995). Even exposure to house cats has been proposed as a risk factor for the development of schizophrenia (Torrey, Rawlings, & Yolken, 2000; Torrey & Yolken, 1995; Yolken, Dickerson, & Torrey, 2009). Infectious parasites hosted by cats, Toxoplasma gondii (T. gondii), are transmitted through ingestion or inhalation of the parasite’s eggs that are shed with the infected cat’s feces into litter boxes and elsewhere. For example, this could occur through hand-to-mouth contact following gardening or cleaning a cat’s litter box. According to this viral zoonosis hypothesis, the T. gondii invade the brain and upset its chemistry, creating the psychotic behaviors recognized as schizophrenia. This may sound far-fetched to you, but many significant correlational findings supporting this hypothesis have been observed. For example, individuals with schizophrenia have an increased prevalence of antibodies to T. gondii in their blood (Torrey, Bartko, Lun, & Yolken, 2007; Torrey, Bartko, & Yolken, 2012; Torrey & Yolken, 2003). This increased prevalence has been observed for both prenatal and early postnatal exposure to T. gondii (Mortensen et al., 2007). Should cat owners panic? Probably not, but keeping basic hygienic precautions in mind is highly recommended.
416
Given these possible genetic, prenatal, and postnatal factors, what might be the organic problems that the person is predisposed to develop? There are two good answers—neurotransmitter imbalances and brain abnormalities. People with schizophrenia have elevated levels of dopamine activity in certain areas in the brain (Davis, Kahn, Ko, & Davidson, 1991). Autopsy and brain scan research indicate that the brains of people with schizophrenia have an excess of dopamine receptors. In addition, drugs that decrease dopamine activity reduce schizophrenic symptoms, and drugs that increase dopamine activity seem to heighten the symptoms of people with schizophrenia and produce schizophrenic symptoms in people who do not have schizophrenia. Such findings led to the development of antipsychotic drugs that are dopamine antagonists (reduce the level of dopamine activity) and help control the symptoms in many people with schizophrenia, especially those with Type I. We will discuss these antipsychotic drugs later in the chapter.
Two psychedelic drugs, phencyclidine (PCP) and ketamine, have also provided some insight into the neurochemistry of schizophrenia (Julien, 2011). These two drugs produce schizophrenia-type symptoms, such as a general motor slowing and reduced speech and other cognitive deficits. The underlying neurochemical action for these drugs is antagonistic, the blocking of glutamate receptors, especially one type of receptor that plays a critical role in brain development and neural processing in general (Javitt & Coyle, 2007). Remember from Chapter 2, glutamate is the major excitatory neurotransmitter in our nervous system. The ability of PCP and ketamine to induce schizophrenia-type symptoms suggests that the actions of these drugs replicate disturbances in the brains of people with schizophrenia. Thus, a glutamate dysfunction has been proposed as a contributor to the development of schizophrenia, especially the negative symptoms and cognitive impairments that are observed (Goff & Coyle, 2001). According to this hypothesis, excessive release of glutamate destroys neurons, especially in the frontal lobes, leading to cortical damage and triggering the mental deterioration observed in schizophrenia. Hence, glutamate neurotransmission has become a promising target for antipsychotic drug development, and antipsychotic drugs that impact glutamate activity levels are presently undergoing clinical trials (Stone, 2011).
417
Various structural brain abnormalities have also been found in people with schizophrenia, especially those suffering from Type II and chronic schizophrenia (Buchanan & Carpenter, 1997; Weyandt, 2006). I’ll mention a few. For example, brain scans of people with schizophrenia often indicate shrunken cerebral tissue and enlarged fluid-filled areas. Some brain areas (the thalamus) seem to be smaller than normal, and the frontal lobes less active. Because structural brain abnormalities have not been observed in the nonpsychotic siblings of people with schizophrenia using multiple imaging methods, these abnormalities for the most part must be due to nongenetic factors (Boos et al., 2012). Prenatal factors, such as the viral infections we discussed, and postnatal factors, such as oxygen deprivation arising from birth complications, likely play a major role in the development of these brain abnormalities (Cannon, 1997; Wright, Takei, Rifkin, & Murray, 1995).
Even given all of this biological evidence, biopsychosocial explanations are necessary to explain all of the evidence accumulated about schizophrenia. A popular biopsychosocial explanation is the vulnerability-stress model—genetic, prenatal, and postnatal biological factors render a person vulnerable to schizophrenia, but environmental stress determines whether it develops or not (Gottesman, 1991). According to the vulnerability–stress model, we vary in our vulnerability to schizophrenia. A person’s level of vulnerability interacts with the stressful social-cognitive events in his life to determine the likelihood of schizophrenia. Remember that schizophrenia typically strikes in late adolescence/early adulthood, periods of unusually high stress levels. There is also some evidence that dysfunctional family environments may be a contributing stress factor (Fowles, 1992).
In summary, there has been much research on the causes of schizophrenia, but we still do not have many clear answers. The only certainty is that schizophrenia is a disabling disorder with many causes. As pointed out in the DSM-5, schizophrenia is a heterogeneous mental disorder and people with schizophrenia will vary substantially in their symptomology. Explanations inevitably involve a biological component, making drug therapy the predominant treatment for schizophrenia. Given the person’s loss of contact with reality, psychotherapies are usually difficult, if not impossible, to institute.
Personality Disorders
A personality disorder is characterized by inflexible, long-standing personality traits that lead to behavior that deviates from cultural norms and results in distress or impairment. The DSM-5 identifies 10 personality disorders divided into three clusters based on their symptoms (APA, 2013). One cluster of three disorders (the avoidant, dependent, and obsessive-compulsive personality disorders) involves highly anxious or fearful behavior patterns. For example, a person with an avoidant personality disorder is so overwhelmed by feelings of inadequacy and rejection that social situations are avoided. A second cluster of three (the paranoid, schizoid, and the schizotypal personality disorders) involves eccentric or odd behavior patterns. For example, a person with a schizoid personality disorder totally avoids social relationships and contact. The last cluster of four disorders (the antisocial, borderline, histrionic, and narcissistic personality disorders) involves excessively dramatic, emotional, or erratic behavior patterns. For example, a person with an antisocial personality disorder shows total disregard for the rights of others and the moral rules of the culture. A person with antisocial personality disorder used to be referred to as a psychopath or sociopath. If you would like to learn more about these disorders, Millon, Millon, Meagher, and Grossman (2004) provide detailed coverage of all 10 personality disorders and their development.
418
Personality disorders usually begin in childhood or adolescence and persist in a stable form throughout adulthood. It has been estimated that 9 to 13 percent of adults in the United States have a personality disorder (Comer, 2014). Personality disorders are fairly resistant to treatment and change. They need to be diagnosed, however, because they give the clinician a more complete understanding of the patient’s behavior and may complicate the treatment for a patient with another mental disorder. In addition, because the symptoms of the 10 personality disorders overlap so much, clinicians sometimes diagnose a person to have more than one personality disorder. This symptom overlap also leads clinicians to disagree about which personality disorder is the correct diagnosis, questioning the reliability of the DSM-5 definitions of these disorders.
Section Summary
In this section, we discussed six major categories of mental disorders—anxiety disorders, obsessive-compulsive and related disorders, depressive disorders, bipolar and related disorders, schizophrenia spectrum and other psychotic disorders, and personality disorders. Anxiety disorders involve excessive fear and anxiety. For each of the anxiety disorders, anxiety is involved in a different way. Panic attacks (being overwhelmed by anxiety and fear) occur suddenly in panic disorder, but the anxiety is chronic and global in generalized anxiety disorder. In specific phobia disorder, there is a marked and persistent fear of specific objects or situations that is excessive and unreasonable. There are two broader types of phobias, however—social anxiety disorder and agoraphobia. Social anxiety disorder involves a fear of social performance situations in which there is exposure to unfamiliar people or scrutiny by others. Causal explanations of anxiety disorders typically involve both behavioral and biological factors.
In obsessive-compulsive disorder, the person experiences recurrent obsessions (persistent thoughts that cause anxiety) and compulsions (repetitive and rigid behaviors that have to be performed to alleviate anxiety). It is not known what causes obsessive-compulsive disorder, but recent research indicates a biochemical lack of serotonin activity in several parts of the brain. Obsessive-compulsive related disorders include hoarding disorder, excoriation (skin-picking) disorder, and trichotillomania (hair-pulling) disorder.
419
Depressive disorders involve the presence of sad, empty, or irritable mood that impacts the individual’s capacity to function. The changes in the person’s emotional mood are excessive and unwarranted. The most common depressive disorder is major depressive disorder, which involves at least one major depressive episode. It is twice as frequent in women as in men. Sometimes this disorder is referred to as unipolar depression in order to contrast it with bipolar disorder, in which the person has recurrent cycles of depressive and manic (elevated mood) episodes. The concordance rate (the likelihood that one identical twin will get the disorder if the other twin has it) is substantial for both disorders, about 50 percent for depression and 70 percent for bipolar disorder. Neurotransmitter imbalances seem to be involved in both disorders, and cognitive factors are involved in major depressive disorder.
Schizophrenia is the most serious disorder discussed in this chapter. It is a psychotic disorder, which means that the person loses contact with reality. Clinicians divide schizophrenic symptoms into three categories—positive, negative, and disorganized. Schizophrenia seems to be a very heterogeneous disorder with many possible causes. Biological abnormalities in people with schizophrenia range from elevated dopamine activity levels to shrunken cerebral tissue, and there is also evidence that prenatal viral infections and birth complications may be involved. A popular biopsychosocial explanation of schizophrenia is the vulnerability–stress model, which proposes that genetic, prenatal, and postnatal biological factors render a person vulnerable to schizophrenia, but environmental stress determines whether it develops or not.
Personality disorders are characterized by inflexible, long-standing personality traits that lead to behavior that impairs social functioning and deviates from cultural norms. The DSM-5 identifies 10 personality disorders. They fall into three clusters, each characterized by a group of problematic personality symptoms. One cluster of disorders involves highly anxious or fearful behavior patterns, one involves eccentric or odd behavior patterns, and the third involves excessively dramatic, emotional, or erratic behavior patterns. Personality disorders are fairly resistant to treatment and change.
ConceptCheck | 2
 Explain what is meant by the biopsychosocial approach and then describe a biopsychosocial explanation for specific phobic disorders.
Explain what is meant by the biopsychosocial approach and then describe a biopsychosocial explanation for specific phobic disorders.A biopsychosocial explanation of a disorder entails explaining the problem as the result of the interaction of biological, psychological (behavioral and cognitive), and sociocultural factors. A good example is the explanation of specific phobia disorders in terms of a behavioral factor (classical conditioning) along with a biological predisposition to learn certain fears more easily. Thus, a psychological factor is involved in the learning of the fear but a biological factor determines which fears are easier to learn. Another good example is the vulnerability–stress model explanation of schizophrenia in which one’s level of vulnerability to schizophrenia is determined by biological factors, but how much stress one experiences and how one copes psychologically with the stress determines whether or not one suffers from the disorder.
-
Explain how the two anxiety disorders, specific phobia and generalized anxiety disorder, are different.
The anxiety and fear in the specific phobia disorder are exactly as the label indicates. They are specific to a certain class of objects or situations. However, the anxiety and fear in generalized anxiety disorder are not specific, but rather global. The person has excessive anxiety and worries most of the time, and the anxiety is not tied to anything in particular.
-
Explain how the concordance rates for identical twins for a major depressive disorder and for schizophrenia indicate that more than biological causes are responsible for these disorders.
The concordance rates for identical twins for major depressive disorder and schizophrenia are only about 1 in 2 (50 percent). If only biological genetic factors were responsible for these disorders, these concordance rates would be 100 percent. Thus, psychological and sociocultural factors must play a role in causing these disorders.
-
Explain the difference between schizophrenia and “split personality.”
Schizophrenia is a psychotic disorder. This means the person loses contact with reality. Thus, the split is between the person’s mental functions (perception, beliefs, and speech) and reality. In “split personality,” which used to be called multiple personality disorder and is now called dissociative identity disorder in the DSM-5, one’s personality is split into two or more distinct personalities.
420