The Brain
The brain has evolved from the brain stem structures that link the brain to the spinal cord all the way up to the cerebral cortex. As we go up the brain stem, processing gets more complex. In fact, it is the very top, the cerebral cortex, that differentiates our brains from those of all other animals. The cerebral cortex enables such complex processes as decision making, language, and perception. Even so, all of the structures below the cerebral cortex are essential for normal behavior and mental processing. This will become clearer as we discuss each structure’s role in this complex, interactive system we call the brain.
Going Up the Brain Stem
Between the spinal cord and the cortex, there are two sets of brain structures—the central core and the limbic system. The brain stem and structures near the brain stem (cerebellum, thalamus, and basal ganglia) can be thought of as the central core of the brain. Surrounding the top border of the brain stem are the limbic system structures—the hypothalamus, hippocampus, and amygdala. Our discussion will start with the central core structures going up the brain stem to the limbic system structures.
The central core.
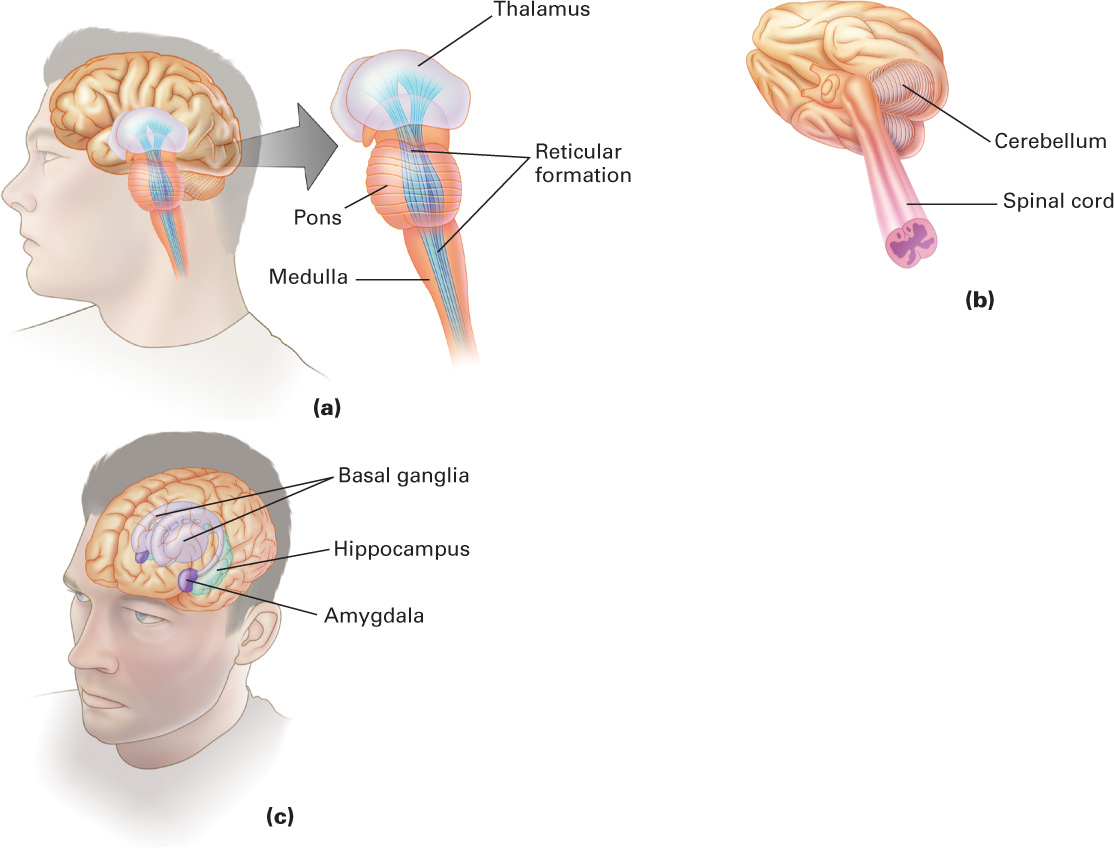
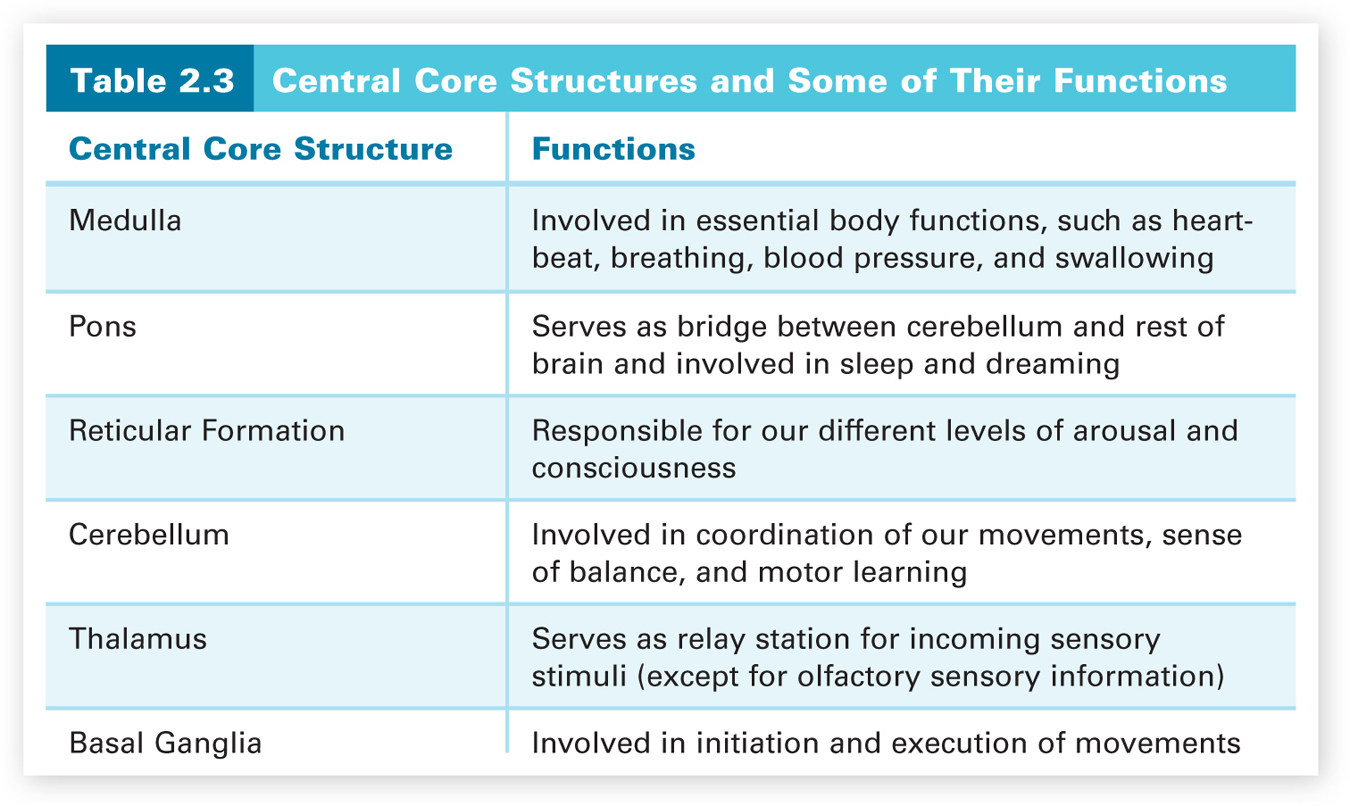
Figure 2.6 shows the central core brain structures. The brain stem spans from the spinal cord up to the thalamus. The first brain stem structure is the medulla, which links the spinal cord to the brain. The medulla is involved in regulating essential body functions such as heartbeat, breathing, blood pressure, digestion, and swallowing. This is why damage to the medulla can result in death. A drug overdose that suppresses proper functioning of the medulla can also lead to death. Just above the medulla, where the brain stem bulges, sits the pons. Along with the medulla, the pons serves as a passageway for neural signals to and from higher areas in the brain. The pons (Latin for “bridge”) functions as a bridge between the cerebellum and the rest of the brain and is involved in sleep and dreaming.
62
The reticular formation is a network of neurons running up the center of the brain stem and into the thalamus, which is involved in controlling our different levels of arousal and awareness. This function was demonstrated by Moruzzi and Magoun (1949) in research with cats. When they stimulated a sleeping cat’s reticular formation, the cat awoke and entered a very alert state. When they severed the connections of the reticular formation with higher brain structures, however, the cat went into a coma from which it could never be awakened. The reticular formation also plays a role in attention by deciding which incoming sensory information enters our conscious awareness.
The cerebellum is involved in the coordination of our movements, our sense of balance, and motor learning. Cerebellum means “little brain” in Latin, and it looks like two minihemispheres attached to the rear of the brain stem. The cerebellum has roughly the same surface area (if unfolded) as a single cerebral hemisphere does (Bower & Parsons, 2007), but it is comprised of smaller neurons so it takes up far less space. Only making up about 10 percent of the brain’s weight (Rilling & Insel, 1998), it has more neurons, an estimated 70 billion (Azevedo et al., 2009), than the rest of the brain combined. This is because the great majority of cerebellar neurons are granule neurons which are very small and can be densely packed into a smaller space. The cerebellum coordinates all of our movements, such as walking, running, and dancing. Damage to the cerebellum will lead to very unsteady, unbalanced movement. Alcohol depresses the functioning of the cerebellum, leading to the uncoordinated movements typical of someone who is drunk. This is why some of the tests for being drunk involve coordinated movement. In addition, the cerebellum is the location of motor learning, such as how to ride a bicycle or to type. There is also some emerging evidence indicating that the cerebellum not only coordinates movement but may also play a role in integrating and coordinating sensory input and in mental functions such as planning (Bower & Parsons, 2007). Lastly, recovery from cerebellar damage, and even from removal of the cerebellum at a young age, is relatively good. Why this is so remains unanswered.
63
The thalamus, located at the top of the brain stem, serves as a relay station for incoming sensory information. As such, it sends each type of sensory information (visual, auditory, taste, or touch) to the appropriate location in the cerebral cortex. The only type of sensory information that does not pass through the thalamus is olfactory (smell) information. Smell information goes directly from the receptors in our nose to the cortex. The basal ganglia are on the outer sides of the thalamus and are concerned mainly with the initiation and execution of physical movements. Like the cerebellum, the basal ganglia are affected by alcohol, and so make the movements required by tests for drunken driving difficult to execute. The basal ganglia are actually a group of various interacting brain regions. As we discussed earlier in this chapter, abnormally low dopamine activity in one region of the basal ganglia results in Parkinson’s disease. Another disease that involves difficulty in controlling movements is Huntington’s chorea, which stems from problems in another region of the ganglia in which there are GABA and acetylcholine deficits.
All of the various central core structures are summarized in Table 2.3 along with some of their major functions.
The limbic system.
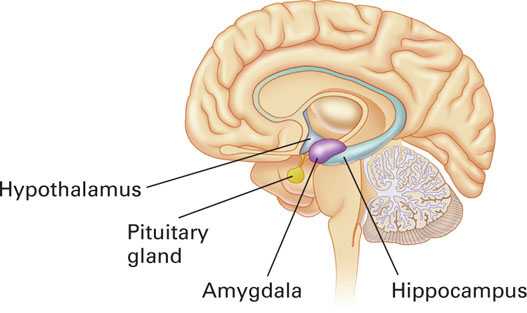
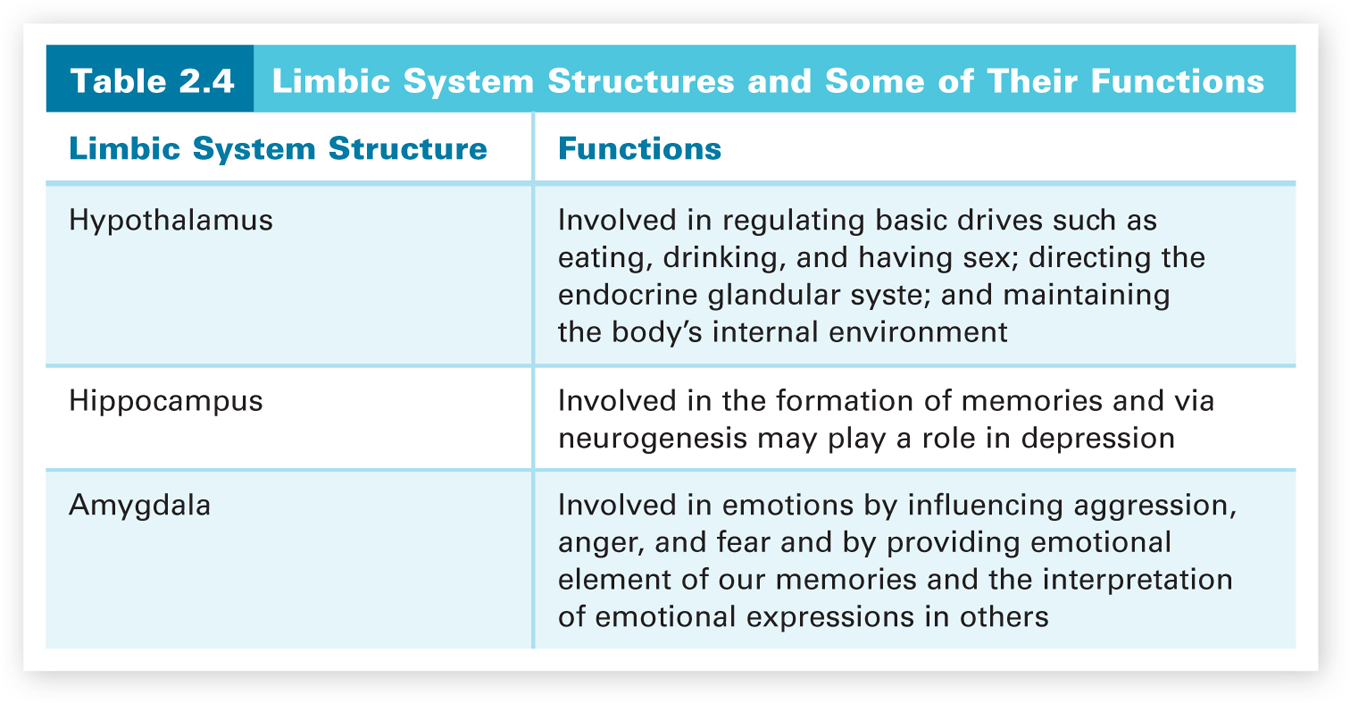
Surrounding the top border (or “limbus” in Latin) of the brain stem is the limbic system, which is made up of the hypothalamus, the amygdala, and the hippocampus. These limbic structures play an important role in our survival, memory, and emotions. Figure 2.7 shows the three parts of the limbic system. The hypothalamus is a very tiny structure, weighing about half an ounce, which is named after its location—below the thalamus (“hypo” means “below” in Greek). The hypothalamus controls the pituitary gland (and so directs activity in the endocrine glandular system) and the autonomic nervous system to maintain the body’s internal environment, such as regulating body temperature. It also plays a major role in regulating basic drives such as eating, drinking, and having sex. Thus, this tiny structure plays a huge role in both our behavior and our survival.
64
The hippocampus is involved in the formation of memories. Hippocampus may seem like a rather strange name, but like many parts of the brain, it was given a name that matched its visual appearance. The hippocampus looks somewhat like a seahorse, and “hippocampus” means “seahorse” in Greek. Recall the case study of H. M. that we discussed in Chapter 1. H. M. had his left and right hippocampal structures removed for medical reasons and as a result suffered severe memory deficits (Corkin, 1984). Subsequent research on H. M. and other people with amnesia has shown the hippocampus to be critical for the formation of certain types of new memories (Cohen & Eichenbaum, 1993), which we will discuss in Chapter 5.
The hippocampus has also been found to have the capacity to generate new neurons, a process called neurogenesis (Gage, 2003; Kempermann & Gage, 1999). The research group most responsible for demonstrating neurogenesis in humans is led by Fred Gage. Given that brain imaging techniques cannot detect neuronal growth and that ethics prohibit neurosurgery to detect such growth in humans, Gage and his colleagues developed a very clever way to demonstrate that such growth exists. BrdU is a traceable substance that has been used in cancer treatment to track how rapidly the disease is spreading. BrdU is integrated into the DNA of cells preparing to divide. Hence it becomes part of the DNA of the new cells and all future descendents of the original dividing cells. Thus, BrdU functions as a marker for new cells. Because BrdU cannot be administered to healthy people, Gage and his colleagues examined postmortem hippocampal tissue of cancer patients who had been injected with BrdU before their deaths, and new noncancerous cells with BrdU were found (Eriksson et al., 1998; van Praag et al, 2002). Although the purposes of neurogenesis in the hippocampus of humans are not yet clear, some research suggests that it may play a key role in depression (Jacobs, van Praag, & Gage, 2000a, 2000b). We will consider this hypothesis in Chapter 10 (Abnormal Psychology).
65
Located just in front of the hippocampal structures are the amygdala left and right structures. Amygdala means “almond” in Greek, and these structures look like almonds. The amygdala plays a major role in regulating our emotional experiences, especially fear, anger, and aggression. It is also responsible for generating quick emotional responses directly, without cortical involvement (LeDoux, 2000). The first evidence for the amygdala’s role in emotional behavior was done on wild, rather violent rhesus monkeys (Klüver & Bucy, 1939). The monkeys’ amygdalas were surgically removed. The surgery transformed the monkeys into calm, tame animals, clearly changing their emotional behavior. Other research has indicated that the amygdala also provides the emotional element in our memories and guides our interpretation of the emotional expressions of others (LeDoux, 1996).
All three structures in the limbic system are summarized in Table 2.4 along with some of their major functions.
66
Processing in the Cerebral Cortex
All of the brain structures that we have discussed so far are important to our behavior and survival. The most important brain structure, however, is the cerebral cortex, the control and information-processing center for the nervous system. This is where perception, language, memory, decision making, and all other higher-level cognitive processing occur. The cerebral cortex physically envelops all of the other brain structures, except for the lowest parts of the brain stem and cerebellum. It is by far the largest part of the brain, accounting for about 80 percent of its total volume (Kolb & Whishaw, 2001). The cerebral cortex consists of layers of interconnected cells that make up the “bark” or covering of the brain’s two hemispheres, which are called cerebral hemispheres. The two hemispheres are separated on top by a deep gap but joined together farther down in the middle by the corpus callosum, a bridge of neurons that allows the two hemispheres to communicate.
The cerebral cortex is very crumpled in appearance with all sorts of bulges and gaps. This allows more cortical surface area to fit inside our rather small skull. If we were to unfold the cerebral cortex to check the amount of surface area, we would find the area to be about the size of four sheets of notebook paper or one newspaper page. Think about this. You couldn’t fit four sheets of paper into your pants pocket unless you crumpled them up. This is the same principle that applies to fitting the large surface area of the cerebral cortex into the small space within the skull. It is this large amount of surface area in the cerebral cortex that not only allows our complex cognitive processing but also differentiates our brains from those of all other animals. To see where different types of processing occur in the cerebral cortex, we need to learn the geography of the two hemispheres. This geography is rather simple in that the outer surface of each hemisphere is divided into four defined parts, called lobes, which we will discuss first.
The four lobes.
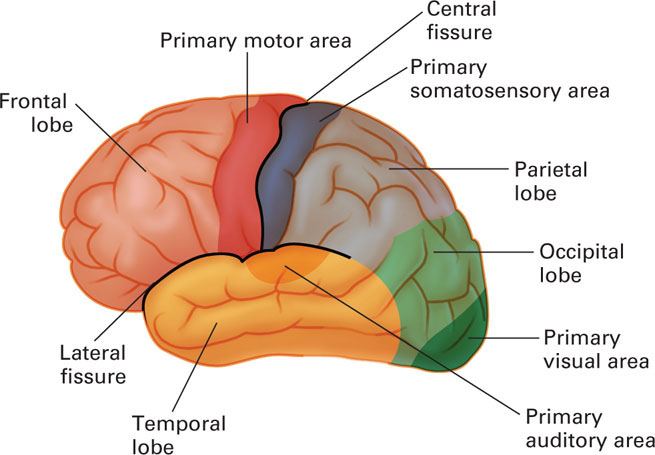
Figure 2.8 shows the four lobes in the left hemisphere. They are the same in the right hemisphere and are named after the specific bone area in the skull covering each of them. Two distinctive fissures (gaps) serve as boundary markers for three of the lobes. The central fissure (also called the fissure of Rolando) runs down the center of each hemisphere, and the lateral fissure (also called the Sylvian fissure) runs back along the side of each hemisphere. The four lobes are named for the four bones of the skull that overlie them. The frontal lobe is the area in front of the central fissure and above the lateral fissure, and the parietal lobe is the area located behind the central fissure and above the lateral fissure. The temporal lobe is located beneath the lateral fissure. The remaining lobe is the occipital lobe, which is located in the lower back of each hemisphere. Brynie (2009) explains how to find your occipital lobes. Run your hand up the back of your neck until you come to a bump and then place your palm on the bump. Your palm is squarely over the occipital lobes. The frontal lobes are the largest of the lobes. Their location is easy to remember because they are in the front of the hemispheres and directly behind our forehead. Now that we know these four areas, we can see what we have learned about what type of processing occurs in each of them. We begin with the well-defined areas for producing voluntary movement of different parts of the body, such as raising a hand or making a fist, and for processing various types of sensory input, such as touch, visual, and auditory information.
67
The motor cortex.
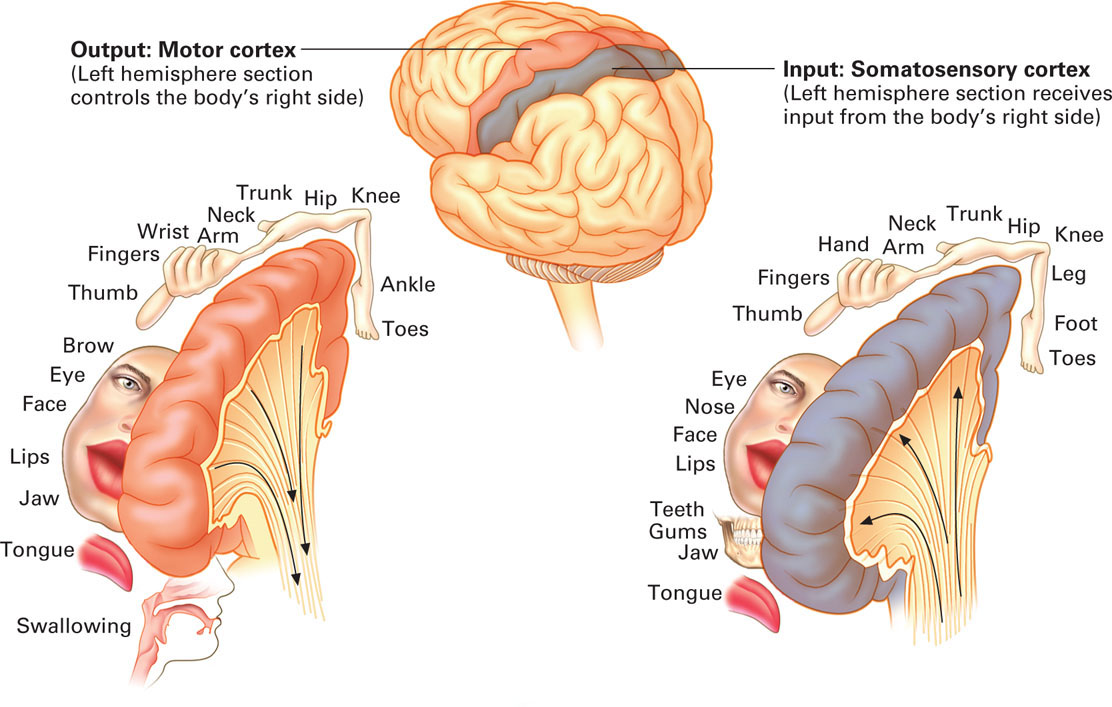
The motor cortex, the frontal lobe strip of cortex directly in front of the central fissure in each hemisphere, allows us to move different parts of our body. The two motor cortex strips are related to the body by contralateral control—each hemisphere controls the voluntary movement of the opposite side of the body. This means that the motor strip in the left hemisphere controls movement in the right side of the body, and the motor strip in the right hemisphere controls movement in the left side of the body. It is also interesting that the amount of space allocated to a specific body part in the motor cortex is not related to the actual size of the body part, but rather to the complexity and precision of movement of which that part is capable. Smaller parts that can make complex movements, such as our fingers, get a large amount of space, and larger parts, such as our torso, that cannot make complex movements do not get much space. Figure 2.9 illustrates this with what is called a homunculus (“little man” in Greek)—a body depiction with the size of each body part proportional to its amount of area in the motor cortex and not its actual size. Note that the body parts are arranged in a toe-to-head fashion spanning from the top of the motor strip to the bottom. It is as if the homunculus is hanging by its toes over the side of the hemisphere.
68
The somatosensory cortex.
The somatosensory cortex, the parietal lobe strip of cortex directly behind the central fissure in each hemisphere, is where our body sensations of pressure, temperature, limb position, and pain are processed. “Somato” is Greek for body. Somatosensory, then, refers to the body senses. In addition to information about touch, the somatosensory cortex receives input about temperature and pain and information from the muscles and joints that allow us to monitor the positions of the various parts of the body. As in the motor cortex, there are contralateral relationships between the somatosensory strips and sides of the body. The somatosensory strip in the left hemisphere interprets the body sensory information for the right side of the body, and the strip in the right hemisphere interprets this information for the left side of the body. In addition, the amount of space within these strips is not allocated by the size of the body part. In the somatosensory cortex, it is allocated in accordance with the sensitivity of the body part—the more sensitive, the more space. For example, the lips and other parts of the face are more sensitive, so they have larger processing areas than body parts, such as our torso, that are not as sensitive. The homunculus for the somatosensory strip is given in Figure 2.9. Like the motor strip, the body is arranged from toe to head, starting at the top of the strip.
69
You may be wondering how the homunculi for the motor and somatosensory strips were determined. They were the result of pre-surgical brain evaluations carried out by Canadian neurosurgeon Wilder Penfield who applied mild electrical stimulation via a single electrode to a patient’s brain before performing surgery for epilepsy (Buonomano, 2011; Seung, 2012). Because the brain itself does not have pain receptors, these surgeries could be performed in conscious patients with only local anesthesia applied to the scalp where incisions were to be made. After pulling back the scalp and opening the skull to expose the brain, Penfield applied electrical probes to different locations in the brain. By carrying out multiple stimulations and meticulously recording the patient’s response to each one, Penfield was able to identify the abnormal tissue causing the patient’s seizures and delineate those areas surrounding the tissue that he had to avoid damaging during the surgery. In using this technique to carry out pre-surgical brain evaluations of his patients, Penfield amassed a large body of stimulation data, which led to the first detailed large-scale functional map of the human cerebral cortex (Penfield & Boldrey, 1937; Penfield & Rasmussen, 1968). He found that when a particular area in the motor cortex was stimulated, a specific part of the patient’s body moved and when a particular area in the somatosensory cortex was stimulated, the patient reported feeling a sensation in a specific body part. These data were used to create the homunculi for the two strips. Using fMRI images, researchers have replicated Penfield’s functional mappings for these two strips (Seung, 2012). The researchers observed which locations in the motor strip were activated by touching parts of a subject’s body and which locations in the somatosensory strip were activated when a subject moved parts of the body.
The visual cortex and the auditory cortex.
There are two other important areas for processing sensory information in Figure 2.8 that we haven’t discussed yet. These are the primary processing areas for our two major senses, seeing and hearing. The visual cortex is located in the occipital lobes at the back of the hemispheres, and the auditory cortex is in the temporal lobes. Figure 2.8 shows where they are located in the left hemisphere. They have the same locations in the right hemisphere. The size of the primary visual cortex varies between individuals over a threefold range in surface area and volume (Dougherty et al., 2003). The reasons for this variability are not known. Interestingly, Schwartzkopf, Song, and Rees (2011) found a strong negative correlation between the magnitude of two context illusions and the surface area of the primary visual cortex. Thus, the smaller your primary visual cortex, the more dramatic some visual illusions appear. The primary visual cortex and the primary auditory cortex are only the locations of the initial processing of visual and auditory information. These primary areas pass the results of their analyses on to areas in the other lobes to complete the brain’s interpretation of the incoming visual or auditory information. These secondary cortical processing areas are part of what is termed the association cortex—all the areas of the cerebral cortex, except for those devoted to primary sensory or motor processing.
70
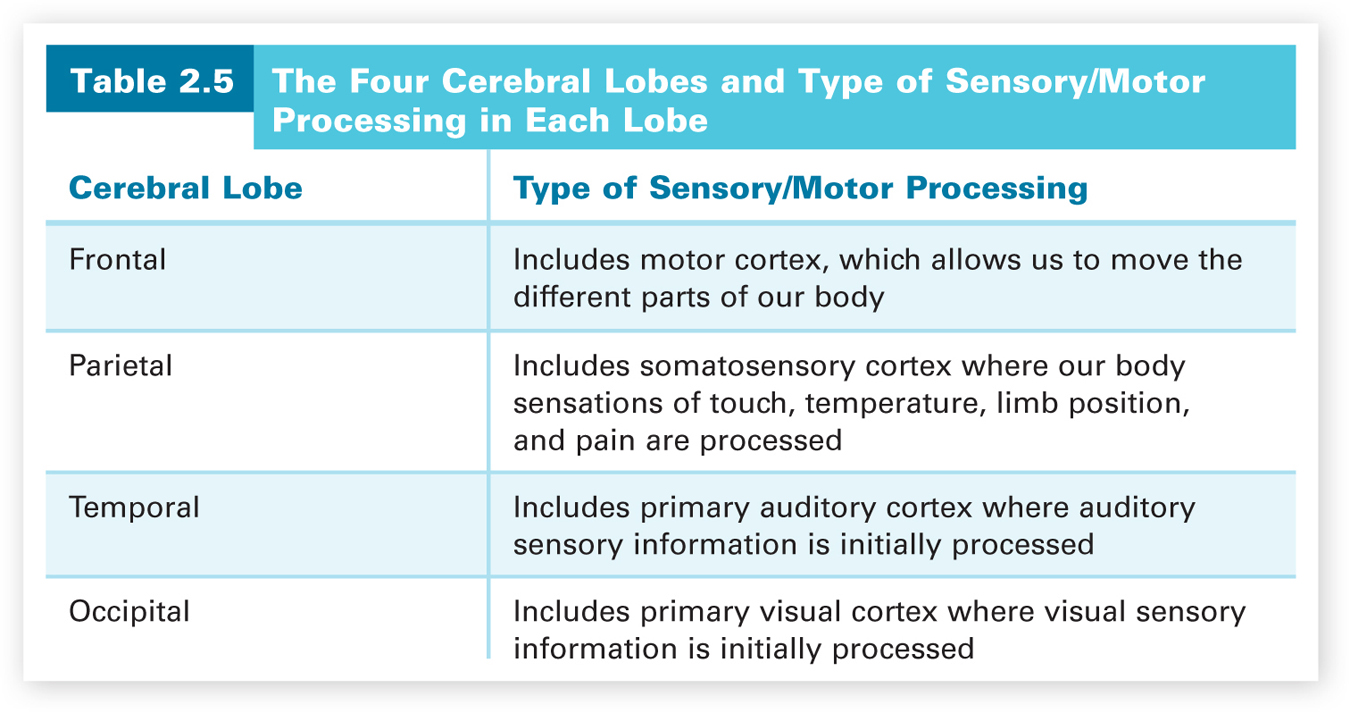
The four cerebral lobes and the type of sensory/motor processing that occurs in each lobe are summarized in Table 2.5.
Given the different locations of the visual cortex and the auditory cortex, you may think that seeing and hearing function entirely separately from each other. The reality, however, is that there is plenty of crosstalk between them. A good example of this interaction is the McGurk effect, which demonstrates that the brain integrates visual and auditory information when processing spoken language (McGurk & MacDonald, 1976). The McGurk effect arises out of conflicting auditory and visual information. A person’s lip movements influence what we hear. For example, if you listen to an audio track of a syllable (“ba”) spoken repeatedly while you watch a video clip of a person making the lip movements as if repeatedly saying another syllable (“ga”), you actually hear a third syllable “da,” the brain’s best guess after merging the information from the two senses. You will have a much better understanding of the McGurk effect if you experience it, and you can find several Web sites that allow you to do so just by doing an online search for the McGurk effect. The McGurk effect is a good example of how visual information can exert a strong influence on what we hear, but it is just one example of how our senses interact. There are many others, such as the smell of food influencing its taste. In interpreting the world, the brain blends the input from all of our senses.
71
It is important not to confuse sensory interaction in general and the McGurk effect, which all of us with normal sensory capabilities can experience, with synesthesia, a rare neurological condition in which otherwise normal people have cross-sensory experiences in which stimulation in one modality leads to automatic, involuntary experiences in another modality. For example, in synesthesia, sounds may evoke tastes, and colors may evoke smells. In addition, perception of a form (e.g., a number) may induce an unusual perception in the same modality (e.g., a color). Although grapheme-color synesthesia (seeing letters, words, and numbers in colors) and sound-color synesthesia (seeing sounds as colors) are the most common types of synesthesia (Brang & Ramachandran, 2011), there are many other types. The exact number is not known. Some people with synesthesia appear to use this union of the senses to inspire their art (Ramachandran & Blakeslee, 1998). For example, Russian artist Wassily Kandinsky said that when he saw colors, he also heard music, leading him to develop his style of abstract painting (Blakeslee & Blakeslee, 2008). It was as if he was capturing music on canvas. Synesthesia affects only 2–4 percent of the population and is believed to stem from some type of cross-wiring in the brain in which normally separate areas of the brain elicit activity in each other (Brang & Ramachandran, 2011). Although familial linkage analyses have shown a strong genetic component, the precise genes involved in synesthesia have not been identified, and why this sensory anomaly has remained in our gene pool remains a mystery. As Eagleman (2011, p. 80) points out in discussing the tiny genetic changes that cause synesthesia, “microscopic changes in brain wiring can lead to different realities,” demonstrating once again that reality is more subjective than most people realize.
The association cortex.
Most of the cortex (about 70 percent) is association cortex. This is where all the higher-level processing such as decision making, reasoning, perception, speech, and language occurs. These areas were named the association cortex because higher-level processing requires the association (integration) of various types of information. Scientists have studied the association cortex for over a century, but they are only beginning to understand the functions of some of the association areas (helped greatly by the recently developed scanning technologies, such as PET scans and fMRI). For example, Sergent, Ohta, and MacDonald (1992) and Kanwisher, McDermott, and Chun (1997) used PET scans and fMRI, respectively, and found a small region on the underside of the temporal lobe near the intersection of the temporal and occipital lobes that responded most strongly to faces. Kanwisher and her colleagues named it the fusiform face area (FFA). Subsequent fMRI studies have confirmed the engagement of the FFA during a range of facial perception tasks (Tong, Nakayama, Moscovitch, Weinrib, and Kanwisher, 2000). The asymmetry of the FFA (it is much larger in the right hemisphere) leads to a right-hemisphere specialization for face recognition (Kanwisher, 2006; Kanwisher & Yovel, 2009). Hence, it is the right hemisphere that is mainly at work when we process faces.
72
Damage to the FFA has also been found to play a role in prosopagnosia (sometimes called face blindness), a condition that impacts a person’s ability to recognize faces including relatives, friends, and acquaintances or even themselves in a mirror (Greuter, 2007; Hadjikhani & de Gelder, 2002). Although a person with prosopagnosia cannot consciously recognize faces, some part of their brain does unconsciously distinguish familiar faces from unfamiliar ones because they show a higher skin conductance response to familiar faces (Tranel & Damasio, 1985). Sadly, prosopagnosia cannot be cured, but people with prosopagnosia learn other ways of recognizing people, such as memorizing a person’s speech patterns, their gait, how they wear their hair, and so on. Surprisingly, prosopagnosia also occurs among people without brain damage and is highly heritable (Wilmer et al., 2010).
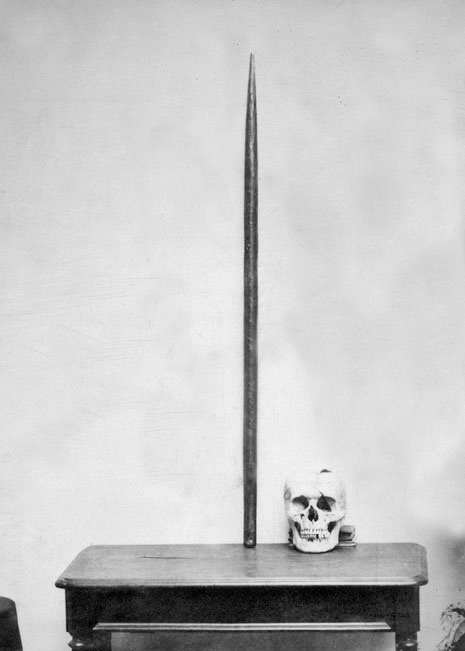
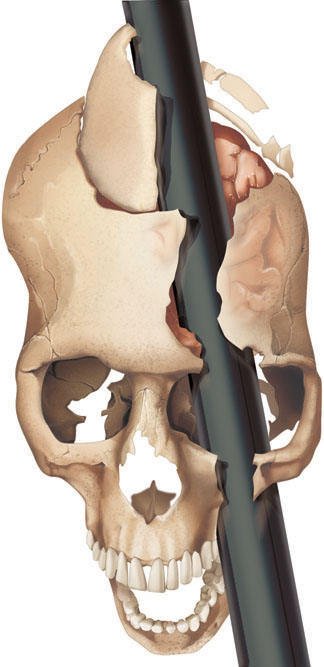
During the nineteenth century and most of the twentieth century, however, brain scans obviously weren’t available, so scientists had to learn about the association areas by other methods. One major method was to study the behavior of people who had suffered brain damage in accidents and strokes, or had brain surgery for medical reasons. Their behavioral and mental processing deficits were then related to the particular cortical areas where damage or surgery had occurred. A railroad worker’s tragic accident in 1848 gave us some hints as to what type of processing occurs in our frontal lobes (Macmillan, 2000). Phineas Gage was taking a break from tamping some blasting powder into a rock with a metal tamping iron. He was distracted and the tamping iron slipped, generating some sparks that caused the powder to explode. The explosion caused the metal tamping iron, which was 3 feet 7 inches long, 1¼ inches in diameter, and 13½ pounds in weight, to fly through his left cheek and head, exiting through his left frontal lobe (Ratiu, Talos, Haker, Lieberman, & Everett, 2004; Van Horn et al., 2012). Before Ratiu et al.’s study, most researchers believed that both frontal lobes were damaged, but Ratiu et al. showed that the cerebral injury was limited to the left frontal lobe. Their computerized tomography scan of Gage’s skull clearly shows this, and Van Horn et al. verified the damage was localized to the left frontal lobe.
73
Gage survived, but his personality was greatly changed. As his doctor and friends pointed out, Gage was “no longer Gage” (Macmillan, 2000). He became very irresponsible, impulsive, and disorderly; had great difficulty making decisions and reasoning; and cursed regularly. This led neuroscientists to hypothesize that the frontal lobes played a major role in such behaviors. Subsequent collaborative evidence from similar cases and from studies using other techniques such as brain scans confirmed that this is the case (Klein & Kihlstrom, 1998). The frontal lobes play a major role in our planning, decision making, judgment, impulse control, and personality, especially its emotional aspects. Actually, the cortical area destroyed in Gage’s left frontal lobe (the prefrontal cortex just behind the forehead and in front of the primary motor cortex) was essentially the left portion of the cortex that was disconnected from the rest of the brain in the infamous lobotomies performed on hundreds of patients in mental hospitals in the middle part of the twentieth century. The frontal lobes may also be partially responsible for the bad decisions and risky behavior of teenagers, because frontal lobe development is not complete until the late teens and possibly even the early 20s (Sabbagh, 2006).
What happened to Phineas Gage? While it has proved very difficult to fill in the exact details of Gage’s subsequent life, Fleischman (2002) provides a general account. Following his recovery, Phineas tried to return to his job as railroad foreman, but because of the “new” Gage’s vulgar, unreliable behavior, the railroad let him go. It appears that for a brief period of time he traveled around New England exhibiting himself along with the tamping iron, possibly ending up in P. T. Barnum’s American Museum sideshow in New York City. After this, because he got along very well with horses, he worked for awhile in a livery stable in New Hampshire near his hometown. In 1852 he traveled, taking the tamping iron with him, to South America to care for horses and be a stagecoach driver in Chile. His work as a stagecoach driver and the fact that he supported himself throughout his post-accident life seem to indicate that he at least partially adapted to his injury (Macmillan & Lena, 2010). Because of health issues he returned in 1859 to California where his family had moved; and after recovering, he found work as a farmhand. In 1860 he began suffering epileptic seizures (likely due to slow changes in his brain tissue damaged in the railroad accident), and at that time, physicians could not control such seizures. These seizures killed him, 11½ years after the accident. The immediate cause of death was probably hypothermia created by the seizures (during which the body cannot control its internal temperature). If you want to find out more about Phineas Gage, go to www.uakron.edu/gage, a Web site created by Malcolm Macmillan, the world’s leading authority on Gage.
74

In 2012, an accident similar to that of Phineas Gage happened in Rio de Janeiro, Brazil. A 24-year old construction worker, Eduardo Leite, survived after a 6-foot metal bar fell from the fifth floor of a building under construction and went through his hard hat, entering his skull and partially exiting between his eyes. Although the bar stayed in Leite’s head, he remained conscious; and the bar was successfully removed by doctors in a 5-hour surgery. Remarkably, Leite was lucid and showed no negative behavioral consequences after the operation. The hospital’s head of neurosurgery said that Leite escaped by just a few centimeters from losing his right eye and becoming paralyzed on the left side of his body. The computerized tomography scan of Leite’s skull pierced by the bar shows that the bar entered in front of the motor cortex in the right hemisphere and exited the right frontal lobe just above the right eye. The doctors concluded that the bar went through “non-eloquent” areas of the brain, areas that have no discernible cognitive, motor, or sensory functions. Phineas Gage was not so fortunate. By using connectograms (circular diagrams depicting the brain’s major white matter connective tracts in the brain), Van Horn et al. (2012) found that Gage’s accident damaged some of the major white matter tracts that connect the frontal lobe with the other three lobes and the limbic system, leading to Gage’s dramatic behavioral changes. In Leite’s case, his brain damage may not have disrupted his brain’s connective networks as Gage’s damage did, possibly accounting for the difference in the behavioral consequences observed.
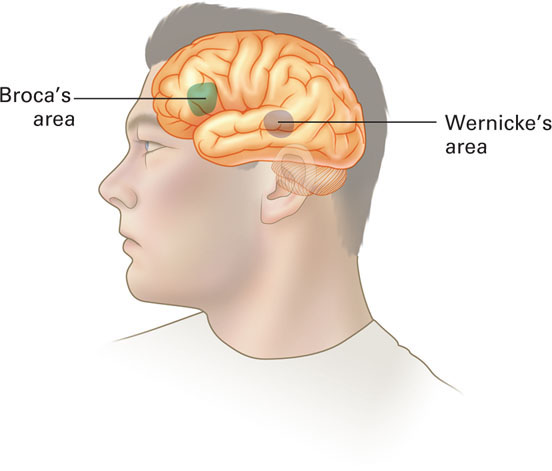
Early brain researchers also analyzed the brains of deceased people, relating a person’s brain analysis to their behavior while living. Using this technique, two nineteenth-century researchers, Paul Broca and Karl Wernicke, studied people with aphasias—speech and language dysfunctions—and made some major discoveries about where speech and language abilities occur in the brain. By examining the brains of deceased persons who had lost their ability to speak fluently while alive, Paul Broca, a French brain researcher, identified an area in the left frontal lobe that is named after him, Broca's area, which is responsible for fluent speech production (see Figure 2.10). Damage to Broca’s area leads to Broca’s aphasia—the inability to generate fluent speech while maintaining the ability to understand speech and read silently.
75
Broca’s area is only in the left hemisphere in the majority of people, both right-handed and left-handed (unlike the sensory and motor processing areas that are in each hemisphere). This means that speech production seems to be a specialization of the left hemisphere (the comparable area in the right hemisphere is usually not used for speech production). So, what is this area in the right hemisphere used for? One possible answer that has been offered is singing and music. People with Broca’s area damage often retain these abilities (Besson, Faita, Peretz, Bonnel, & Requin, 1998). This means that singing and speaking seem to originate from different areas of the brain. What about Broca’s area in deaf people who use sign language? Will damage to Broca’s area impact their ability to use sign language? The answer is yes. Broca’s area seems important for both the production of speech and its complement in the deaf, sign language (Corina, 1998).
People with damage to Broca’s area do not have a problem understanding the speech of other people or reading silently, which means these skills must involve other areas. One of these areas is in the left temporal lobe and is named after its discoverer, Karl Wernicke, a German researcher. Wernicke's area is responsible for the comprehension of speech and reading. Figure 2.10 shows exactly where this area is located. Damage to this area leads to Wernicke’s aphasia—incoherent speech and the inability to understand the speech of others and to read. Wernicke’s area functions as the understanding center for incoming speech and text.
Like Broca’s area, Wernicke’s area is only in the left temporal lobe of the majority of people (regardless of handedness). Many people have the misconception that these speech and language centers normally reside in the hemisphere opposite to a person’s handedness. This is only the case for a very small number of right-handers and some left-handers, however. Speech and language centers are located in the left hemisphere for about 95 percent of right-handers and 70 percent of left-handers (Springer & Deutsch, 1998).
Broca and Wernicke examined the brains of deceased people who had speech and language dysfunctions in order to identify the speech and language centers in the brain. So perhaps this cortical localization technique could be used with highly intelligent people to identify the keys to their genius, the neural basis of intellect? What about the brain of acclaimed genius, Albert Einstein? Was it studied after his death in 1955? The answer is a much qualified yes, because his brain was not studied in the careful, systematic manner that you would think it would be. The journey that Einstein’s brain took was indeed a bizarre odyssey (Abraham, 2001). With the exception of his brain and eyes, his body was cremated on the day of his death; but to this day no one seems to know where the ashes are (Lepore, 2001). The examining pathologist at Princeton Hospital where Einstein died, Dr. Thomas Harvey, removed the brain and took dozens of photographs of the whole and partially dissected brain before having it partitioned into 240 blocks of tissue, preparing a roadmap of the locations in the brain that yielded the dissected blocks, and sectioning and staining histological slides from the blocks.
76

Despite Harvey’s meticulous preservation of Einstein’s brain and the distribution of some brain sections to a few researchers, nothing had yet been published 23 years later when Harvey was interviewed in 1978 (Lepore, 2001). During this time period, Harvey kept most of the brain hidden away for his own personal research. He stored these remaining dissected and labeled brain pieces in glass jars of formaldehyde in a cider box in his office. Einstein’s brain usually accompanied him when he traveled. In fact, Dr. Harvey made a trip across America to visit Einstein’s granddaughter with some of the photographs and slides and some pieces of the brain floating in formaldehyde in a Tupperware bowl in a duffel bag in the trunk of a car (Paterniti, 2000).
Starting in the 1980s Harvey did dole out some more of the slides and photographs to researchers. This led to six peer-reviewed publications and a few speculative differences between Einstein’s brain and those of people with normal intelligence (Falk, Lepore, & Noe, 2012). For example, Diamond, Scheibel, Murphy, and Harvey (1985) found a higher glia to neuron ratio in the left parietal lobe, and Witelson, Kigar, and Harvey (1999) found that the gross anatomy of Einstein’s brain seemed within normal limits with the exception of his parietal lobes. These findings led to the hypothesis that Einstein’s unusual parietal lobes might have provided the neural basis for his visuospatial and mathematical skills. In 2007 Harvey died, but fortunately Dr. Harvey’s Estate donated 14 of Harvey’s photographs of Einstein’s whole brain (last seen in 1955) along with some of the histological slides and the roadmap that identifies the brain locations that yielded the slides to the National Museum of Health and Medicine (Falk, Lepore, & Noe, 2012).
Granted access to these materials, Falk et al. (2012) were able to describe the external gross neuroanatomy of Einstein’s entire cerebral cortex in comparison to 85 normal human brains. Many of the photographs show structures that were not visible in the photographs previously analyzed. Falk et al. found that Einstein’s brain was of unexceptional size but had very unusual morphology. The complexity and pattern of convolutions and folds in the prefrontal lobe, parietal lobe, visual cortex, and primary motor and somatosensory cortices gave these parts a much larger surface area than in normal brains. Falk et al. also speculated on the meaning of their findings. For example, the expanded prefrontal cortex may have contributed to the neurological substrates for some of Einstein’s remarkable abilities, and the unusual parietal lobes are consistent with the earlier hypothesis that they may have provided the neurological underpinnings for his visuospatial and mathematical abilities. But the long, strange journey for Einstein’s brain hasn’t ended. In 2012, digital preservations of some of the slides of Einstein’s brain became available to the general public as an iPad application. You have to wonder whether Einstein would have wanted images of his remains sold to nonscientists for $9.99.
77
Specializations of the Left and Right Hemispheres
Next, we will consider the question of whether there are any hemispheric specializations other than speech, language, and face perception. To try to answer this question, researchers have examined patients who have had their corpus callosum, the cortical bridge between the two hemispheres, severed as a medical treatment for severe cases of epilepsy. William Van Wagenen performed the first split-brain surgery in 1940 (Gazzaniga, 2008). Not many people have had this surgery, and because of improved medications and other modes of treatment for epilepsy, it is done even more rarely now. The rationale behind this surgery was that the epileptic seizures would be lessened in severity if they were confined to only one hemisphere. Indeed, the surgery did provide this benefit. However, it also created a group of people (usually referred to as “split-brain” patients) in which the two hemispheres of the brain could not communicate, comprising an ideal group for studying the question of hemispheric specialization. According to Gazzaniga (2008), there have only been 10 split-brain patients who have been well tested. First, we will discuss the general experimental procedure that has been used to study the hemispheric specialization question with these patients.
Studying the two hemispheres.
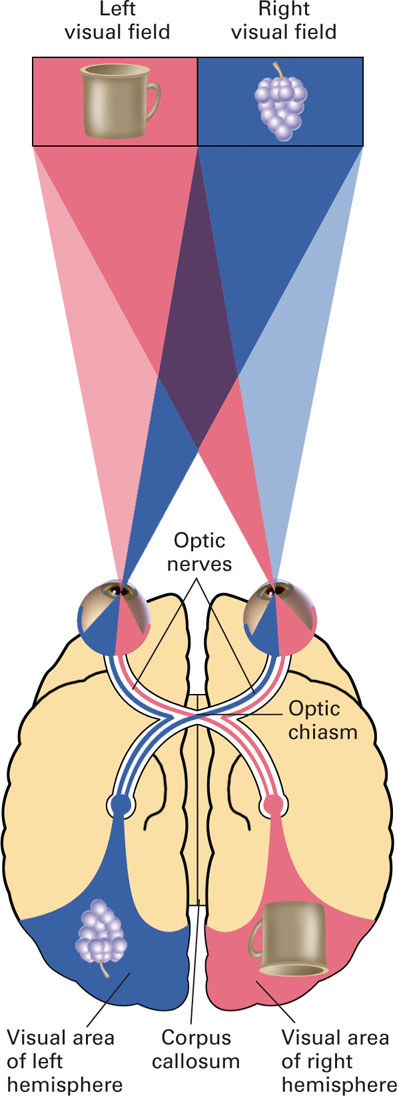
To understand the experimental procedure for studying the two hemispheres, we first need to understand how the visual fields, the eyes, and the cerebral hemispheres are related. These relationships are shown in Figure 2.11. Our field of vision has two halves—the left visual field (what is to the left of center in our field of vision) and the right visual field (what is to the right of center in our field of vision). Light waves from the left visual field go to the right half of each eye, and those from the right visual field go the left half of each eye. Each visual field is processed by half of each eye. The right half of each eye connects with the right hemisphere, and the left half of each eye with the left hemisphere. This means that the eyes and the hemispheres, with respect to processing incoming visual information, are not contralaterally related. Rather, the visual information in half of each eye goes to each hemisphere. The visual information in the right halves goes to the right hemisphere, and the visual information in the left halves goes to the left hemisphere. Thus, information in the left visual field goes only to the right hemisphere, and information in the right visual field goes only to the left hemisphere. The following diagram should help you remember this processing sequence:
78
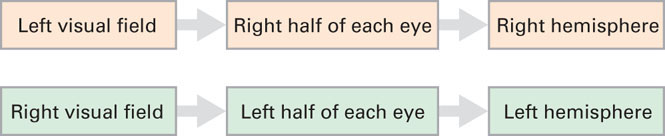
This relationship between the visual fields and the hemispheres is important because it allows information that is presented briefly in one visual field to go to only one hemisphere. With split-brain patients, the information cannot be transferred to the other hemisphere because the corpus callosum connecting their two hemispheres has been severed. By examining how split-brain patients can identify the presented information (orally, visually, or by touch), researchers can study the hemispheric specialization question.
Recall that the speech and language centers (Broca’s and Wernicke’s areas) are only in the left hemisphere of the vast majority of people. This would mean that a split-brain patient should only be able to identify information orally when it is presented briefly in the right visual field (it is this field that feeds information to the left hemisphere). In fact, this is what has been found with split-brain patients. For example, if a picture of a spoon were flashed briefly in the left visual field, a split-brain patient would not be able to say that it was a spoon. But if we blindfolded the split-brain patient and asked her to identify the flashed object from a group of objects by touch with the left hand, the split-brain patient can do this (Gazzaniga, 1992). Remember that the somatosensory strip in the right hemisphere is connected to the left hand. However, even after identifying the spoon as the object presented, a split-brain patient would not be able to identify it orally if asked what was in her left hand. What would happen if the blindfolded split-brain patient were asked to move the object from her left hand to her right hand? She would now say that she was holding a spoon. The information that it was a spoon would be gathered through touch by her right hand and sent to the somatosensory strip in her left hemisphere, allowing her to transfer this information to the speech centers in the left hemisphere.
79
Split-brain patients are also sometimes asked to identify the presented information by pointing with the appropriate hand (left hand for right hemisphere, right hand for left hemisphere). A clever use of this methodology involves simultaneously presenting different objects to each hemisphere. For example, an orange might be shown in the right visual field so it goes to the left hemisphere, and an apple in the left visual field so it goes to the right hemisphere. If then asked to use the left hand to identify what was presented, the split-brain patient would point to the apple; but if she had been asked to use the right hand, she would have pointed to the orange. In each case, the nonresponding hemisphere would be baffled by the other hemisphere’s response.
What we know about the left and right hemispheres.
The two most prominent researchers on split-brain questions have been Roger Sperry and Michael Gazzaniga. Sperry led most of the early split-brain research and in 1981 won the Nobel Prize in Physiology or Medicine for his discoveries concerning the functional specializations of the cerebral hemispheres. Sperry’s student, Michael Gazzaniga, who conducted the first studies with human split-brain participants in the early 1960s at the California Institute of Technology under the guidance of Sperry and neurosurgeon Joseph Bogen (Gazzaniga, Bogen, & Sperry, 1962), has continued this line of inquiry for the past five decades (Gazzaniga, 2005, 2008). Now let’s see what these studies with split-brain participants have told us about hemispheric specialization.
We know that the speech and language centers are specialties of the left hemisphere. This is why the left hemisphere is sometimes referred to as the verbal hemisphere. This does not mean, however, that the right hemisphere has no verbal ability. It can’t produce speech, but it can understand simple verbal material. In addition, the left hemisphere is better at mathematical skills and logic, while the right is better at spatial perception, solving spatial problems (block design), and drawing. The right hemisphere is also better at face recognition. Due to the asymmetry in the fusiform face area, recognition of faces is faster when faces are presented in the left- than the right-visual field of both split-brain patients (Stone, Nisenson, Eliassen, & Gazzaniga, 1996) and normal people (Yovel, Tambini, & Brandman, 2008). In general, the left hemisphere is more analytic, analyzing wholes into their elements or pieces; the right hemisphere processes information in a more holistic fashion, combining pieces into wholes (Reuter-Lorenz & Miller, 1998). The right gets the big picture (the “forest”); the left focuses on the smaller details (the “trees”). This information-processing style difference between the two hemispheres is sometimes referred to as global versus local processing.
80
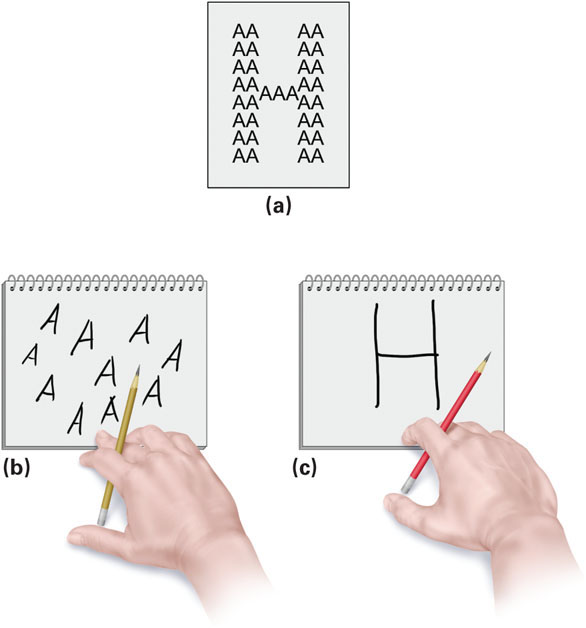
Support for this general processing style difference between the hemispheres has been corroborated by research with brain-damaged patients using hierarchical stimuli developed by David Navon (1977). These hierarchical stimuli consist of a large letter (the global, holistic level) that is composed of smaller versions of another letter (the local or analytic level). See the example in Figure 2.12a in which the large letter H is composed of smaller As. Delis, Robertson, and Efron (1986) used such stimuli to study perceptual encoding in brain-damaged patients. The patients were asked to study the hierarchical stimulus and then redraw it from memory after a brief period of distraction. The patients with right hemisphere damage who were dependent on their left hemisphere often drew As unsystematically scattered about the page (see Figure 2.12b). They remembered the constituent elements of the original stimulus but not the overall pattern. In contrast, the patients with left hemisphere damage who were dependent on their right hemisphere often drew a large capital H but with no As (see Figure 2.12c). They remembered the global pattern but not the constituent elements. Thus, the right hemisphere specializes in synthesizing global, holistic patterns, whereas the left hemisphere specializes in analyzing the details of a stimulus. Fink et al. (1996) have also observed this hemispheric processing style difference in PET scan data when normal participants were attending to either the global or local level of Navon hierarchical figures.
This processing difference along with all of the other specialization differences that have been observed in split-brain patients have led to the expressions “left-brained” and “right-brained” to refer to people who seem to excel at the skills normally attributed to left and right hemispheres, respectively. We must remember, however, that these differences in hemispheric performance are for people whose two hemispheres can no longer communicate. When normal people are performing a task, the two hemispheres are constantly interacting and sharing information. There is no forced separation of labor as in the split-brain patient. It may be the case that one hemisphere tends to play a larger role in some tasks, but both hemispheres are involved (Corballis, 2007; Hellige, 1993). This is why it is not very accurate to say someone is “left-brained” or “right-brained.” It is best not to make the distinction. Nearly all of us are “whole-brained.”
81
Consciousness and the Sleeping Brain
There are many questions left for neuroscientists to answer about the brain and its many functions, but the most intriguing questions concern human consciousness—What is consciousness and what underlies it? Probably the best way to think about consciousness is as a person’s subjective awareness of his inner thinking and feeling as well as his immediate surroundings. Thus, consciousness is both internal (one’s thoughts and feelings) and external (what’s going on in one’s environment).
Most brain (and bodily) functioning goes on without our conscious awareness. For example, you are presently recognizing the letters and words in this paragraph, but you are not consciously aware of the actual processing required to accomplish this recognition. You are only consciously aware of the results of the recognition process (the meaningful collection of words). Even if you wanted to, you couldn’t become consciously aware of this processing by the brain. Think about the billions of neurons communicating with each other within your brain and nervous system at this very moment. You cannot become aware of activity at this neuronal level of processing. Our consciousness is privy to only some of the results of this processing.
We can describe waking consciousness as our tuning in to both our internal and external worlds, but questions about exactly what underlies it (how it is generated) or why it evolved remain open for debate. Similarly, we are still pondering the question of why we experience sleep—a natural, altered state of consciousness. We do, however, have some better answers to questions about what the brain is doing during sleep. Electrical recordings of brain activity during sleep allow us to measure different stages of sleep and to tell us when we are dreaming. So first we’ll examine the stages of sleep and how they are related to dreaming. Then, we will briefly discuss theories that have been proposed to explain why we sleep and why we dream.
The five stages of sleep.
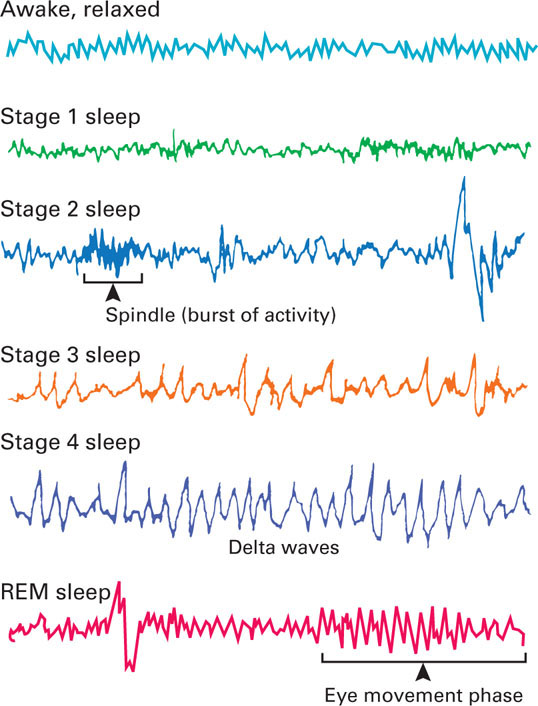
The various stages of sleep have been determined by monitoring the electrical activity in the brain using an electroencephalograph (EEG). Small electrodes are attached to the scalp and connected to recording equipment that produces a real-time graph of electrical activity in the cortex of the brain. In Figure 2.13 on the following page, a sample EEG for the awake, relaxed state is shown along with sample EEGs for the five stages of sleep. As we slip into sleep and pass through the first four stages, our brain waves change, in general becoming progressively slower, larger, and more irregular, especially in Stages 3 and 4. Stage 1 sleep, which lasts about 5 minutes, is followed by about 20 minutes of Stage 2 sleep, which is characterized by periodic bursts of rapid activity called sleep spindles. Some researchers believe these spindles represent the activity of a mechanism that lessens the brain’s sensitivity to sensory input and thus keeps the person asleep. The fact that older people’s sleep contains fewer spindles and is interrupted by more awakenings during the night is consistent with this explanation.
82
Next are the two stages comprising slow-wave sleep—the brief, transitional sleep of Stage 3 and then the deep sleep of Stage 4. These two stages, especially Stage 4, are characterized by delta waves—large, slow brain waves. You are now completely asleep and this initial period of slow-wave sleep lasts for about 30 minutes. In deep sleep, the parasympathetic nervous system dominates. So, muscles relax, heart rate slows, blood pressure declines, and digestion is stimulated. Mysteriously, the brain is still monitoring environmental information, though it is outside our conscious awareness. If a sensory stimulus is important, such as a baby’s cry, or very strong, such as a slamming door or a breaking glass, it will break through the perceptual barrier created by sleep and awaken us.
Near the end of your first period of deep sleep (about an hour after falling asleep), you return through Stages 3 and 2 and enter REM (rapid eye movement) sleep, the most fascinating stage of sleep. REM sleep is characterized by very rapid waves somewhat like those of Stage 1 sleep. However, you are still sound asleep. REM sleep is sometimes referred to as paradoxical sleep because the muscles are relaxed, but other body systems and the brain are active, following a waking pattern. Heart rate rises, breathing is more rapid, eyes move back and forth rapidly under closed eyelids, and one’s genitals become aroused. The brain is also highly active; both oxygen consumption and cerebral blood flow increase. Strangely, given all of this internal activity, the muscles are relaxed, leaving the body essentially paralyzed except for occasional muscle twitching.
83
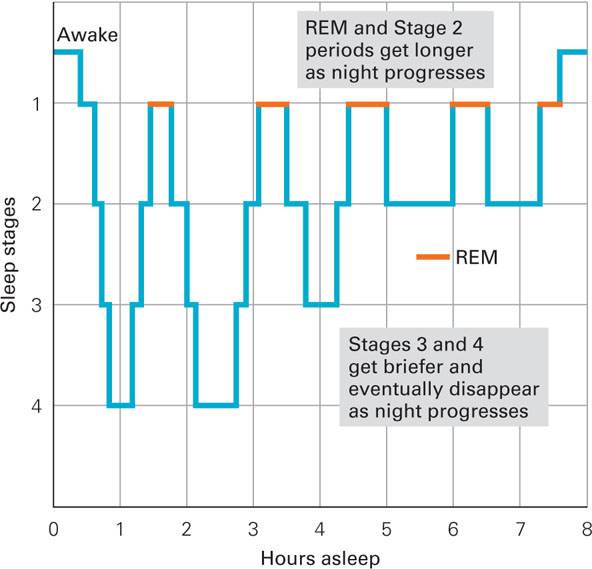
REM sleep indicates the beginning of dreaming; it is the stage during which most dreaming occurs. How do we know this? If people are awakened during Stages 1 through 4, they only occasionally report dreaming; but if awakened during REM sleep, people usually recall dreams that they were having. This is as true for people who say they dream as for those who say they rarely do so, which means that we all dream whether we realize it or not. This first bout of REM sleep typically lasts about 10 minutes and completes the first sleep cycle of the night. The cycle of stages, in which we move out of and back into REM sleep, repeats itself about every 90 minutes throughout the night. Deep sleep (Stages 3 and 4) gets briefer and eventually disappears, as Stage 2 and REM sleep periods get longer with each sleep cycle. Over the course of the night, you have four or five REM sleep periods, amounting to about 20 to 25 percent of your sleep time (Figure 2.14).
We spend on average about 2 hours a night dreaming, which works out to about 6 years of dreaming across our lifetime, given current life expectancies. We don’t remember many of our dreams, though. The dreams we do remember are usually from our last phase of REM sleep, right before we wake up. Many dreams are highly emotional and unpleasant. For example, people often dream of being attacked or pursued. This may be due to the fact that the frontal lobes (responsible for rational thought) are shut down during REM sleep, but the amygdala and the hippocampus, the limbic system structures responsible for emotion and memory, are active, creating the irrational imagery and emotional experiences of our dream world. Given the strong visual nature of dreams, what are the dreams of blind people like? Research indicates that people born blind or who go blind very early in life do not have visual dreams. Their dreams are just as emotional, but involve other sensations, especially sounds.
Why do we sleep and dream?
We do not know why we sleep, but we know that we need sleep. You cannot cheat sleep; it will always overcome you. Inadequate sleep has a high cost. Sleep-deprived people have impaired concentration and a general bodily feeling of weakness and discomfort, and they may even hallucinate. Sleep deprivation also suppresses your immune system, lessening your ability to fight off infection and disease. Sleep-deprived people are also more vulnerable to accidents. For example, traffic accidents increase following the shortened sleep accompanying the 1-hour time change in the spring (Coren, 1993). All of this may help explain why people who typically sleep 7 or 8 hours outlive those who are chronically sleep deprived (Dement, 1999). College students are notorious for being sleep deprived, with as many as four out of five not getting adequate sleep. Beware of sleep deprivation and its negative effects. Sleep deprivation makes it more difficult to concentrate, study, and take exams. So, creating a large sleep debt will, in simple terms, “make you stupid” (Dement, 1999, p. 231).
84
We clearly need sleep. How much, however, varies greatly with individuals. On the average, though, we spend about a third of our lives sleeping. Why? Three possible answers have been proposed, and the actual answer probably involves all three. First, sleep seems to serve a restorative function by allowing the brain and body time to rest and recuperate from the daily wear and tear of our existence. Sleep is necessary for optimal functioning. Second, sleep helps us process what we learn. It allows the brain the opportunity to consolidate our day’s experiences into our memory banks for later retrieval and use. Indeed, there is research evidence that memory is often strengthened and enhanced following a period of sleep (Stickgold & Ellenbogen, 2009). REM sleep is especially important in relation to memory. Disruption of REM sleep (by being constantly awakened during this stage) following learning impairs our memory for this learning (DuJardin, Guerrien, & LeConte, 1990). Disruption of other sleep stages does not impair memory similarly. Third, sleep may have evolved as an adaptive process. It served a protective function for our ancestors, increasing their survival by keeping them safe from predators during the night and from the dangers of wandering around cliffs in the dark. Those who stayed in their caves and slept had a better chance of surviving and passing on their genes.
So, sleep has clear advantages. But why do we dream? One answer is the critical role of REM sleep in learning—providing the opportunity for memory consolidation of new information (Stickgold, Hobson, Fosse, & Fosse, 2001). Other answers to the question of why we dream have also been proposed. About a hundred years ago, Sigmund Freud proposed that dreams were disguised outlets for the inner conflicts of our unconscious (Freud 1900/1953a). But given its lack of scientific support, the Freudian view has been rejected by most contemporary sleep researchers. There are many contemporary theories of why we dream, but all have their critics. One explanation, however, that has received much attention is the activation-synthesis theory (Hobson, 2003; Hobson & McCarley, 1977; Hobson, Pace-Scott, & Stickgold, 2000). This physiological theory proposes that neurons in the pons fire spontaneously during REM sleep, sending random signals to various areas in the cortex and the emotional areas in the limbic system. The signals are random, but the brain tries to make sense of them and produce a meaningful interpretation. Thus, a dream is the brain’s synthesis of these signals. However, because the signals evoke random memories and visual images, the brain has a difficult time weaving a coherent story, often resulting in the bizarre and confusing nature of our dreams. This relates to a major criticism of the theory: dream content is more coherent, consistent over time, and concerned with waking problems and anxieties than the activation-synthesis theory would predict (Domhoff, 2003). Criticisms aside, this theory has led to a wide body of research on the neurological stuff that dreams are made of and thus greatly increased our knowledge of the physiological basis of dreaming.
85
In contrast to the activation-synthesis theory of dreaming, the neurocognitive theory of dreaming emphasizes the parallels between waking cognition and dreaming (Domhoff, 2011). Neurocognitive theory argues that explaining dreams as our subjective interpretations of random neural firing is too simple and that dreams are meaningful products of our cognitive abilities, with continuity between waking and dreaming cognition. Most dreams are about people and activities that are well-known to the dreamer and reflect our waking concerns, personality, emotions, and interests (Domhoff, 1996; Nir & Tononi, 2010). According to neurocognitive theory, the dreams of children younger than 9- or 10-years-old are simpler and less emotional and bizarre than adult dreams. Why? Children’s dream development parallels the gradual development of advanced cognitive abilities, such as visual imagination. Once their cognitive abilities are more advanced, their dreams become more complex. In brief, dreams are a product of our normal cognitive processes, but they use self-generated sensory data during sleep rather than external sensory input as they do when we are awake.
Although sleep researchers do not agree about why we dream, they do agree that REM sleep is essential. This is clearly demonstrated by the REM sleep rebound effect—a significant increase in the amount of REM sleep following deprivation of REM sleep. The fact that REM sleep and the rebound effect are observed in other mammals implies a definite biological need for this type of sleep. Exactly what that need is, however, remains an open question.
Section Summary
In this section, we discussed many of the major structures in the brain. Between the spinal cord and the cerebral hemispheres, there are two sets of brain structures—the central core and limbic system. The central core is made up of the medulla, pons, and reticular formation (parts of the brain stem) and the cerebellum, thalamus, and basal ganglia (structures near the brain stem). The medulla regulates essential body functions, such as breathing and blood pressure, and the pons serves as a bridge between the cerebellum and the rest of the brain. The reticular formation is involved in controlling different levels of arousal and awareness. The cerebellum is involved in the coordination of movement and motor learning, the thalamus serves as a relay station for incoming sensory information, and the basal ganglia are involved in the initiation and execution of physical movements. Surrounding the top of the brain, the limbic system structures (hypothalamus, hippocampus, and amygdala) play important roles in our survival, memory, and emotions.
86
As we move up the brain stem to the cerebral hemispheres, the functioning gets more complex. It is the top cortical layer that gives us all of our complex abilities (such as language, perception, and decision making) and makes us “human.” Each cerebral hemisphere is divided into four lobes—frontal, parietal, temporal, and occipital. The motor cortex in the frontal lobes allows us to move different parts of our body. The somatosensory cortex in the parietal lobes is where our body sensations of touch, temperature, limb position, and pain are processed. Both the motor cortex and the somatosensory cortex are related to the two sides of our body in a contralateral fashion—the left hemisphere controls the movement of, and processes body sensations from, the right side of the body, and the right hemisphere does so for the left side of the body. The primary visual cortex is in the occipital lobes, and the primary auditory cortex is in the temporal lobes. The remaining area in the two hemispheres, about 70 percent of the cortex, is called the association cortex. All of the higher-level cognitive processing, including perception and decision making, occurs in the association cortex. Such processing requires the association of various types of information.
Research has shown that the frontal lobes play a major role in our planning, reasoning, impulse control, and personality—especially its emotional aspects. We have also learned that the speech and language areas are only in the left hemisphere in the majority of people, regardless of handedness. Broca’s area in the left frontal lobe is responsible for speech production, and Wernicke’s area in the left temporal lobe is responsible for the comprehension of speech and text. In addition, research on split-brain patients (whose hemispheres cannot communicate because they have had their corpus callosum surgically severed) has shown that there are processing differences between the two hemispheres. For example, the left specializes in speech, language, mathematical skills, and logic; the right specializes in spatial perception, face recognition, and drawing. In addition, the right hemisphere specializes in processing stimuli at the holistic, global level, whereas the left hemisphere analyzes stimuli into their elements or pieces. We must remember, however, that in normal people, the two hemispheres are constantly interacting. One hemisphere may play a more major role in some tasks, but both hemispheres are involved.
Neuroscientists have much more to learn not only about the brain but also about consciousness, a person’s awareness of his inner thinking and feeling and his external environment. We have learned much about sleep, a natural altered state of consciousness, through the use of EEG recordings of the brain’s electrical activity while sleeping. Such recordings indicate the occurrence of five different stages of sleep, with the REM (rapid eye movement) sleep stage as the one during which most dreaming occurs. We can’t yet explain definitively why we sleep or why we dream, but both are clearly essential. Sleep-deprived people suffer many consequences ranging from impaired concentration to weakened immune systems. A rebound effect for REM sleep (a significant increase in REM sleep) follows REM sleep deprivation.
87
ConceptCheck | 3
 Explain where in the cerebral cortex (which hemisphere, lobe, area in the lobe, and part of that area) is active when you feel a slap on the left cheek of your face.
Explain where in the cerebral cortex (which hemisphere, lobe, area in the lobe, and part of that area) is active when you feel a slap on the left cheek of your face.
To feel a slap on the left cheek of your face, the area devoted to the cheek in the lower half of the somatosensory cortical strip in the parietal lobe in the right hemisphere would be activated. Refer to Figure 2.9 to see the exact location of the cheek in the somatosensory homunculus and thus the activation. Remember that the activation would be at this location in the right hemisphere because your left cheek was slapped.
-
Explain which areas in the cerebral cortex are involved and how they are involved when you shadow (repeat aloud) someone’s speech.
When you shadow someone’s speech, the auditory sensory input from the person’s speech goes first to the primary auditory cortex in the temporal lobes, next to Wernicke’s area to be understood, and then to Broca’s area to produce the appropriate motor programs, which are then sent to the motor cortex, which then executes the programs to activate your speech muscles to produce the speech.
-
Explain what types of behavioral deficits would be observed in a person who suffered damage to her cerebellum.
A person who suffered damage to her cerebellum would have problems in motor coordination and balance. Her movements would be jerky and uncoordinated, and she would have great difficulty maintaining her balance.
-
Explain how you could demonstrate that a split-brain patient knows what was briefly flashed in his left visual field, even though he cannot say what was flashed.
You would ask him to identify the object by the sense of touch with his left hand. He could identify it by matching the tactile input (the information gathered from touching the object) with his knowledge of what had been presented, both in the right hemisphere.
-
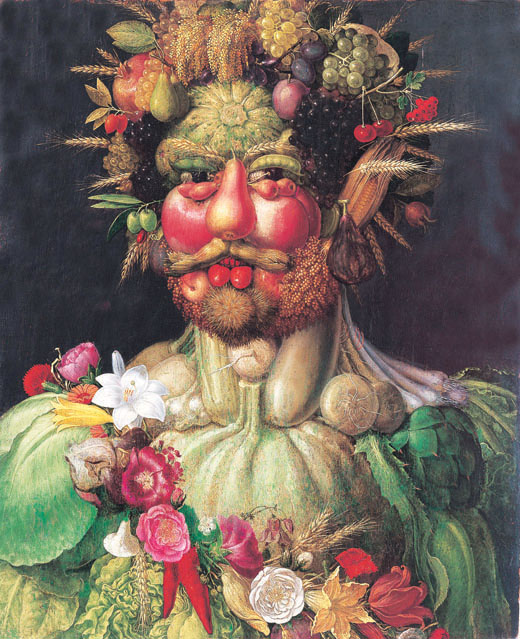
This 400-year-old painting, Vertumnus, was done by Giuseppe Arcimboldo, a sixteenth-century Italian painter who is best known for creating imaginative portraits from such objects as fruits, vegetables, flowers, books, and other objects. Vertumnus is a portrait of Rudolf II of Prague made from fruits, flowers, and vegetables. Let’s use this portrait to test your understanding of both the processing differences between the two hemispheres and the relationship between the visual fields and the hemispheres. Suppose Vertumnus is flashed briefly in the left visual field of a split-brain patient and he is instructed to point with the appropriate hand to what he saw given the choice of the two words “face” and “fruits.” Which hand would he use and which word would he point to? Why? Now suppose the painting had been flashed briefly in his right visual field. Which hand would he use and which word would he point to? Why?
 The Art Archive at Art Resource, NY
The Art Archive at Art Resource, NYIf Vertumnus were flashed briefly in a split-brain person’s left visual field, it would be processed in his right hemisphere. Hence he would use his left hand to respond because the right hemisphere’s motor cortex controls that hand. Because the right hemisphere specializes in face recognition and engages in visual, holistic processing, he would point to “face” because the overall global impression of the painting is a face. However, if the painting had been flashed briefly in his right visual field, he would use his right hand because the painting would be processed in the left hemisphere, which controls that hand. Because the left hemisphere engages in analytic processing of the elements of a stimulus, the painting would be analyzed into its component elements (fruits, flowers, and vegetables) so he would point to “fruits,” one of the main elements of the face. Gazzaniga has actually conducted some experimental trials using some of Arcimboldo’s paintings with a split-brain participant and found these predicted results.
-
Explain why REM sleep is sometimes referred to as paradoxical sleep.
REM sleep is sometimes referred to as paradoxical sleep because your bodily muscles are relaxed and immobilized, but many parts of your brain are active with both oxygen consumption and cerebral blood flow increasing. The brain appears to be awake, but you are behaviorally asleep.
88