7.1 Prenatal Development and Infancy
What happens in the prenatal environment? What sensory abilities do we have at birth? Is our brain fully developed at birth? These are the kinds of questions that we will address in this section. We know, for instance, that the brain is not fully developed at birth. Remember, we learned in Chapter 5, on memory, that we do not have any explicit memories about this period of our life because the hippocampus isn’t fully developed until later. Thus, this next section should interest all of us, because we have no memory of our own life in the prenatal stage and infancy. Let’s get started with the beginning of all development—
Prenatal Development
zygote The fertilized egg that is formed from the union of the sperm and egg cells in human reproduction.
Human conception begins when a sperm (male reproductive cell) penetrates the membrane of an ovum, or egg (female reproductive cell). Each of these reproductive cells contains genetic instructions. When the two combine, a complete set of genetic instructions is formed, half from the father and half from the mother. The fertilized egg that is formed from the union of the sperm and egg cells is called a zygote. All other cells in the human body develop from this single cell, and each duplicate cell carries a copy of the genetic instructions of the original zygote. The zygote develops into a growing cluster as the cells duplicate.
gene The basic unit of genetic instruction.
chromosomes Molecules of DNA that hold the genetic instructions for every cell in the body.
The gene is the basic unit of genetic instruction. Genes are short segments of chromosomes, molecules of DNA (deoxyribonucleic acid) that hold the genetic instructions for every cell in our body. Except for reproductive cells (sperm and eggs), every cell of a normal human has 23 pairs of chromosomes, one of each pair coming from the mother and one from the father. Reproductive cells receive only one member of each pair, giving them only 23 chromosomes. This means that when a sperm combines with an ovum, the zygote will have the complete 46. It is the 23rd pair of chromosomes that determines a person’s sex. In a female, there are two X-
289
identical (monozygotic) twins Twins that originate from the same zygote.
fraternal (dizygotic) twins Twins that originate from the fertilization of two eggs at approximately the same time (two zygotes).
In some cases, the growing cluster of duplicated cells breaks apart early in development, resulting in two clusters with identical genes. These clusters become identical (monozygotic) twins. They are identical because they originate from the same zygote. Fraternal (dizygotic) twins originate from the fertilization of two eggs at approximately the same time. Thus, fraternal twins are nonidentical and could be of different sexes and just as different as any two children with the same parents. You may be wondering why two children with the same parents can be very different in appearance. The answer is the same reason that children with different parents vary greatly in appearance—
Prenatal development (conception until birth) is divided into three stages—
teratogens Environmental agents such as drugs and viruses, diseases, and physical conditions that impair prenatal development and lead to birth defects and sometimes death.
fetal alcohol syndrome (FAS) A syndrome affecting infants whose mothers consumed large amounts of alcohol during pregnancy, resulting in a range of severe effects including intellectual disability and facial abnormalities.
Both genetic and environmental factors impact prenatal development. The nature–
290
Other risks to newborns include prematurity and low birth weight. Those that are born prematurely, before the 37th week, have a number of problems, which increase with the degree of prematurity. Major health problems of premature infants include immaturity of the lungs and the digestive and immune systems. Premature infants also have low birth weight, although some full-
How We Develop During Infancy
Motor development and sensory-
sucking reflex An innate human reflex that leads infants to suck anything that touches their lips.
rooting reflex An innate human reflex that leads infants to turn their mouth toward anything that touches their cheeks and search for something to suck on.
Motor development. The newborn comes equipped with several motor reflexes, which are unlearned responses. Some of these reflexes, such as the breathing reflex that provides us with oxygen, have obvious survival value and are permanent, but others aren’t as necessary and disappear within the first year of life. Two examples of reflexes that disappear are the Babinski reflex, in which infants fan their toes upward when their feet are touched, and the grasping reflex, in which infants grasp any object that touches their palms. Two other motor reflexes, the sucking reflex and the rooting reflex, are concerned with getting nourishment and so are obviously related to survival. The sucking reflex leads infants to suck anything that touches their lips, and the rooting reflex leads infants to turn their mouths toward anything that touches their cheeks and search for something to suck on.

291
In this first year or so of life, infants learn to sit, stand, and walk. This is an orderly sequence; each new motor behavior builds upon previous ones. Infants learn to prop up and support their body, then to sit without support, then to crawl, then to stand while holding onto an object, then to stand without support, and finally to walk without support at somewhere around 12 months of age. It was once thought that motor development was primarily a maturational process that unfolded according to a genetic program. However, as with most achievements, the process is more complex. Learning how to walk, for instance, involves the interaction of multiple factors, such as increases in strength, body proportions, and balance (Thelen, 1995). During this first year, infants are also developing their perceptual abilities and learning to coordinate their body movements with perceptual input. In fact, the process infants go through when they learn how to move around by themselves leads to changes in depth perception (our ability to perceive the distance of objects from us). Infants who have experienced crawling develop a fear of heights and falling, whereas infants of the same age who are not yet crawling do not show this fear (Campos, Anderson, Barbu-
habituation A decrease in the physiological responding to a stimulus once it becomes familiar.
Sensory-
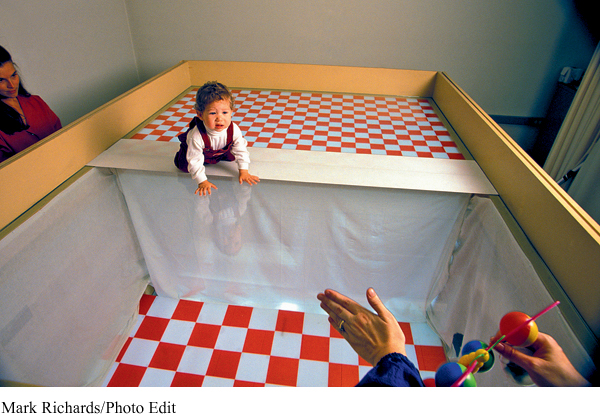
Through these ingenious techniques we have learned that our five senses are functional at birth (though not fully developed). Vision, our dominant sense, is the least developed at birth. Newborns cannot see very clearly. Their visual acuity (resolution of visual detail) is estimated to be about 20/400 to 20/800 (Kellman & Banks, 1998). This means that the visual detail that a person with normal 20/20 vision can see at 400 to 800 feet is what the infant sees at 20 feet. This lack of resolution is due to inadequate connections between the infant’s eyes and the brain, but these connections develop quickly. Hence, acuity develops quickly and reaches 20/20 within the first year of life. Color vision develops even sooner, by two to three months, when it becomes comparable to that of adults (Kellman & Arterberry, 1998). We also know that depth perception develops rather quickly (Gibson & Walk, 1960). Demonstrations of this have used an apparatus called the visual cliff, a table with a glass top that gives the illusion of a very steep (cliff-
292
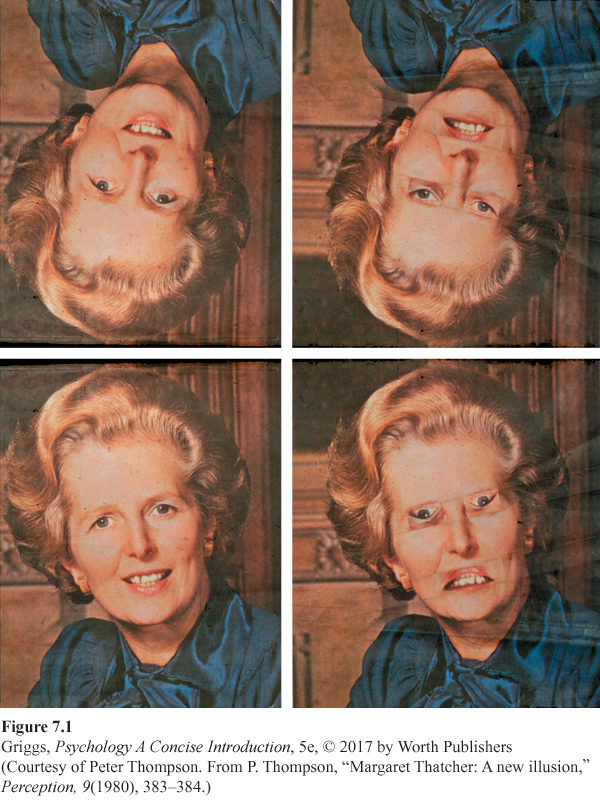
We also know that infants have a visual preference for faces, especially their mother’s face, and other complex stimuli (Field, Cohen, Garcia, & Greenberg, 1984; Valenza, Simion, Cassia, & Umiltà, 1996). Infants’ preference for such visual complexity may be due to the fact that such stimulation is necessary for proper development of the visual pathways and cortex during infancy (Greenough, Black, & Wallace, 1987). In addition to their visual preference for faces, recent research indicates that the ability to process configural information in upright faces (i.e., the structural relationships between the individual features on the face) may already be present at birth (Leo & Simion, 2009). The manner in which Leo and Simion demonstrated this is interesting because it involves what is called Thatcherization, an illusion created by Peter Thompson (1980) involving images of former Prime Minister Margaret Thatcher. Thatcherization is created by rotating the eyes and mouth 180° within the image of a face, causing the face to appear grotesque. See Figure 7.1. The top row looks like two upside-
293
Adults readily detect changes in face patterns brought about by Thatcherization when the faces are viewed upright but not when they are viewed upside down (Thompson, 1980). This inability to quickly discriminate a Thatcherized face from an unaltered face when viewed upside down is thought to be caused by the disruption of configural processing, so that the structural changes from Thatcherization are no longer apparent (Bartlett & Searcy, 1993). Leo and Simion wanted to know if newborns would respond like adults to such faces. Using the habituation paradigm, they tested newborns’ ability to discriminate a normal face and a Thatcherized face when presented upright and also upside down. Newborns could do so when the faces were upright (as in the bottom row of Figure 7.1) but not when the faces were upside down (as in the top row), the same inversion effect observed in adults. Hence, Leo and Simion concluded that newborns were sensitive to configural information in faces.
294
Hearing in the newborn is even more fully developed than vision. In fact, newborns can distinguish their mother’s voice from those of others (DeCasper & Fifer, 1980). Research indicates this ability and several auditory preferences develop in the womb before birth (Dirix, Nijhuis, Jongsma, & Hornstra, 2009). Let’s briefly consider one of the most famous studies indicating the effects of prenatal learning on auditory preferences after birth (DeCasper & Spence, 1986). During the final 16 weeks of pregnancy, mothers read Dr. Seuss’s The Cat in the Hat aloud twice a day. Following birth, the researchers had the babies suck on an artificial nipple that, depending upon the infant’s sucking pattern, would activate a tape of their mother reading the Dr. Seuss story or another story that the mother had never read aloud. Most of the infants sucked to hear The Cat in the Hat. The infants preferred the familiar story that their mothers had read to them while they were still in the womb. Then, Spence and Freeman (1996) carried out a similar experiment but used a low-
phonemes The smallest distinctive speech sounds in a language.
One of the most remarkable hearing abilities that infants possess involves speech perception. Phonemes are the smallest distinctive speech sounds in a language. They allow us to distinguish between different words. For example, the difference between the words pat and bat is the difference in the pa and ba phonemes. In order to learn a language, infants must be able to detect these subtle differences between phonemes, and they are able to do so soon after birth. Different languages do not use all the same phonemes, and adults who are not native speakers of a particular language have difficulty detecting the speech sounds of that language. Japanese adults, for example, have trouble with the English r and l sounds. Infants, in contrast, can detect all phonemes whether or not they have been exposed to them. By 12 months of age, however, they no longer can easily detect speech sounds not in their native language (Kuhl, 2004). Interestingly though, a brief amount of exposure given through live social interaction is sufficient to maintain the ability to detect nonnative phonemes (Kuhl, Tsao, & Liu, 2003). It seems as though infants come into the world prepared to learn whatever language they happen to find themselves exposed to, and experience fine-
295
The senses of smell, taste, and touch are also fairly well developed at birth. For example, infants can differentiate the smell of their mother from the smells of other people. Researchers discovered this by placing a nursing pad worn by the mother on one side of an infant and a pad worn by another woman on the other side, then measured how long the baby was turned toward each side. The infants spent more time turned toward their mother’s pad (MacFarlane, 1975).
Some recent studies have indicated that infants’ understanding of the physical world and their cognitive abilities may be much better than was previously thought. Researchers have demonstrated that very young infants may have an innate conceptual understanding of object movement—
Development of an infant’s cognitive and perceptual abilities depends upon brain development. The brain contains about 100 billion neurons at birth, but the infant’s brain is rather immature, and connections between neurons (neural networks) need to be formed. During the first few months of life, there is a large growth spurt for these connections between neurons, especially those in the cortex that control perception and cognition. Thousands of new connections are established for these neurons. The connections between the retina and the brain are a good example. Without visual experiences, these visual pathways do not develop, and vision will be permanently lost (Kalat, 2007). This is why a baby born with cataracts that prevent vision needs to have them removed as early as possible, so that normal vision will develop. During infancy, the networks of neurons that are used become stronger, and those that are not used disappear (Thompson, 2000).
Section Summary
Our prenatal development starts with conception, the fertilization of an egg by a sperm to form a zygote, and proceeds through the germinal stage (first two weeks), the embryonic stage (two weeks to two months), and the fetal stage (two months to birth). Prenatal development is guided by the zygote’s genetic code (nature), but teratogens (environmental agents such as drugs or viruses, diseases, and malnutrition) can impact the prenatal environment (nurture) and result in birth defects and even death. Other factors that affect prenatal development include fetal alcohol syndrome and the age of the mother. Prematurity and low birth weight are also risks to newborns. The newborn comes equipped with several motor reflexes, some critical for survival, such as the rooting and sucking reflexes that lead to nourishment, and some not so critical, such as the grasping reflex, which disappear within the first year of life. Within this first year, the infant learns to sit, stand, and walk in a very orderly sequence; each new motor behavior builds upon previous ones. They also learn to coordinate their body movements with perceptual input.
Although not fully developed, our five senses are functional at birth, with vision being the least developed. To study early sensory-
296
1
Question 7.1
.
Explain how the effects of teratogens are due to nurture and not nature.
Teratogens are agents such as drugs, viruses, and diseases and conditions such as malnutrition that impair prenatal development and lead to birth defects or even death. Thus, they are not due to heredity (nature). They are prenatal environmental factors, and therefore their effects are due to nurture.
Question 7.2
.
Explain how habituation is used to study infant sensory-
Habituation, a decrease in physiological responding to a stimulus once it becomes familiar, is used to determine what stimuli an infant can perceptually discriminate. The inference is that if an infant looks longer at a new stimulus than an old one, then the infant must be able to perceive the difference. In addition to looking, researchers use other measures such as changes in the rates of sucking on a pacifier and the infant’s heart rate.