12-4 Neuroanatomy of Motivated and Emotional Behavior
The neural circuits that control behavior encompass regions at all levels of the brain, but the critical neural structures in emotional and motivated behavior are the hypothalamus and associated pituitary gland, the limbic system, and the frontal lobes. The expression of emotions includes physiological changes: in heart rate, blood pressure, and hormone secretions. It also includes motor responses, especially movements of the muscles that produce facial expressions (see Figure 12-9). So much of human life revolves around emotions that understanding them is central to understanding our humanness.
But emotions are not restricted to people. A horse that is expecting alfalfa for dinner will turn its nose up at grass hay and may stomp its front feet and toss its head. Two dogs that are in competition for attention may snap at one another. Charles Darwin interpreted such behaviors as emotions in his classic book The Expression of the Emotions in Man and Animals, published in 1872. We now know that emotional expression in all mammals is related to activity in the limbic system and frontal lobes.
411
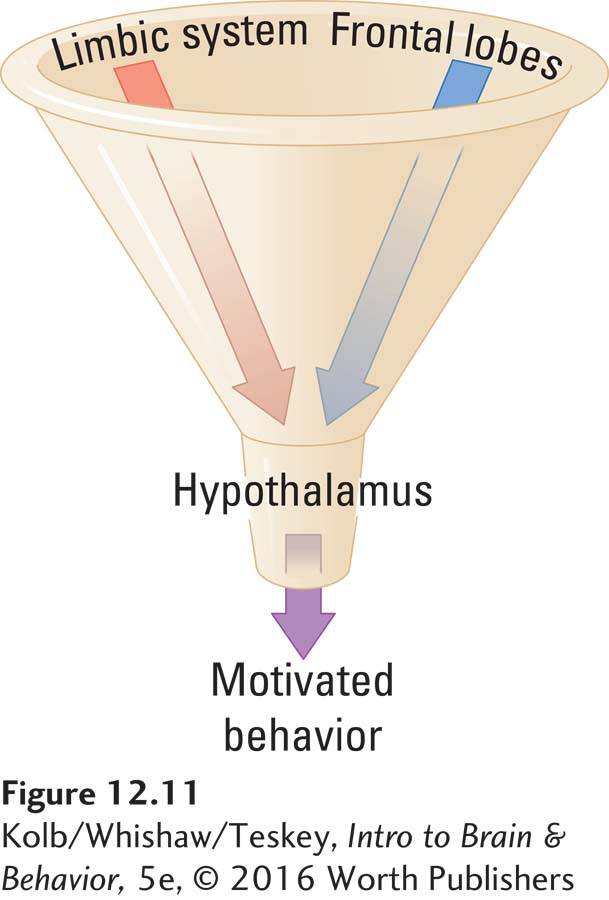
Although the hypothalamus plays a central role in controlling motivated behavior, it takes its instructions from the limbic system and the frontal lobes. The limbic and frontal regions project to the hypothalamus, which houses many basic neural circuits for controlling behavior and for autonomic processes that maintain critical body functions within a narrow, fixed range—
Section 6-5 explores hormonal regulation of homeostatic mechanisms.
In Figure 12-11, the neck of a funnel represents the hypothalamus, and the limbic system and frontal lobes form the funnel’s rim. To produce behavior, the hypothalamus sends axons to other brainstem circuits. But not all behavior is controlled via the funnel to the hypothalamus. Many other routes to the brainstem and spinal cord bypass the hypothalamus, among them projections from the motor cortex to the brainstem and spinal cord. Thus it is primarily motivated behaviors that require hypothalamic involvement.
Regulatory and Nonregulatory Behavior
We seek mates, food, or sensory stimulation because of brain activity, but we talk about such behavior as being motivated. Motivated behaviors are not something in the brain that we can point to, however. Rather, motivations are inferences we make about why someone, ourselves included, engages in a particular behavior. The two general classes of motivated behaviors are regulatory and nonregulatory. In this section we explore both categories before exploring the neuroanatomy of motivation and emotion.
Regulatory Behaviors
Regulatory behaviors—behaviors motivated by an organism’s survival—
Human body temperature is controlled in a somewhat similar manner by a thermostat in the hypothalamus that holds internal temperature at about 37°C, a temperature referred to as a set point. Even slight variations cause us to engage in various behaviors to regain the set point. For example, when body temperature drops slightly, neural circuits that increase body temperature turn on. These neural circuits might induce an involuntary response such as shivering or a seemingly voluntary behavior such as moving closer to a heat source. Conversely, if body temperature rises slightly, we sweat or move to a cooler place.
Similar mechanisms control many other homeostatic processes, including the amount of water in the body, the balance of dietary nutrients, and the blood sugar level. Control of many such homeostatic systems is quite complex, requiring both neural and hormonal mechanisms. In some way, however, all of the body’s homeostatic systems involve hypothalamic activity.
Imagine that specific cells are especially sensitive to temperature. When they are cool, they become very active; when they are warm, they become less active. These cells could function as a thermostat, telling the body when it is too cool or too warm. A similar set of cells could serve as a glucostat, controlling the level of sugar in the blood, or as a hydrostat, controlling the amount of water in the body. In fact, the body’s real homeostatic mechanisms are slightly more complex than this imagined one, but they work on the same general principle.
Mechanisms to hold conditions such as temperature constant have evolved because the body, including the brain, is a chemical soup in which thousands of reactions are taking place all the time. Maintaining constant temperature is critical. When temperature changes, even by 2°C, the rates at which chemical reactions take place change.
Such changes might be tolerable, within certain limits, if all the reaction times changed to the same extent. But they do not. Consequently, an increase of 2°C might increase one reaction by 10 percent and another by only 2 percent. Such uneven changes would wreak havoc with finely tuned body processes such as metabolism and the workings of neurons.
412
A similar logic applies to maintaining homeostasis in other body systems. For instance, cells require certain concentrations of water, salt, and glucose to function properly. Wild fluctuations in the concentrations cause a gross disturbance of metabolic balance and eventually biological disaster.
Nonregulatory Behaviors
Unlike regulatory behaviors, such as eating or drinking, nonregulatory behaviors are neither required to meet the basic survival needs of an animal nor controlled by homeostatic mechanisms. Thus, nonregulatory behaviors include everything else we do—
| Categories of Motivated Behavior |
|---|
| Some Regulatory Behaviors |
| Internal body temperature |
| Eating and drinking |
| Salt consumption |
| Waste elimination |
| Some Nonregulatory Behaviors |
| Sex |
| Parenting |
| Aggression |
| Food preference |
| Curiosity |
| Reading |
Some nonregulatory behaviors, such as sexual intercourse, entail the hypothalamus, but most of them probably do not. Rather, such behaviors entail a variety of forebrain structures, especially the frontal lobes. Presumably, as the forebrain evolved and enlarged, so did our range of nonregulatory behaviors.
Most nonregulatory behaviors are strongly influenced by external stimuli. As a result, sensory systems must play some role in controlling them. For example, the sexual behavior of most male mammals is strongly influenced by the pheromone emitted by receptive females. If the olfactory system is not functioning properly, we can expect abnormalities in sexual behavior. We will return to sexual behavior in Section 12-5, as we investigate how a nonregulatory behavior is controlled. But first we explore the brain structures that take part in motivated behaviors—
Regulatory Function of the Hypothalamic Circuit
Figure 2-30 diagrams ANS pathways and connections.
The hypothalamus maintains homeostasis by acting on both the endocrine system and the autonomic nervous system (ANS) to regulate our internal environment. The hypothalamus also influences the behaviors selected by the rest of the brain, especially by the limbic system. Although it constitutes less than 1 percent of the human brain’s volume, the hypothalamus controls an amazing variety of motivated behaviors, ranging from heart rate to feeding and sexual activity.
Hypothalamic Involvement in Hormone Secretions
A principal function of the hypothalamus is to control the pituitary gland, which is attached to it by a stalk (Figure 12-12A). Figure 12-12B diagrams the anatomic location of the hypothalamus in each hemisphere, with the thalamus above and the optic tracts just lateral.
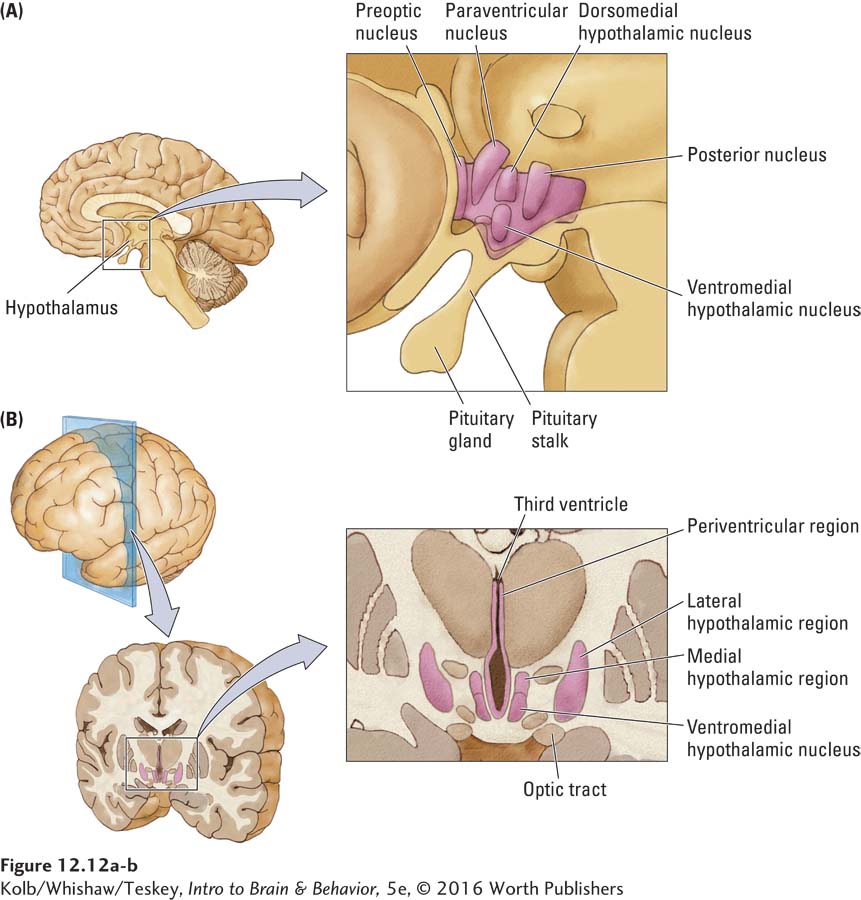
We can divide the hypothalamus into three regions, lateral, medial, and periventricular, illustrated in frontal view in Figure 12-13, is the medial forebrain bundle (MFB).
Section 6-4 elaborates on dopamine’s importance in experiences related to drug use.
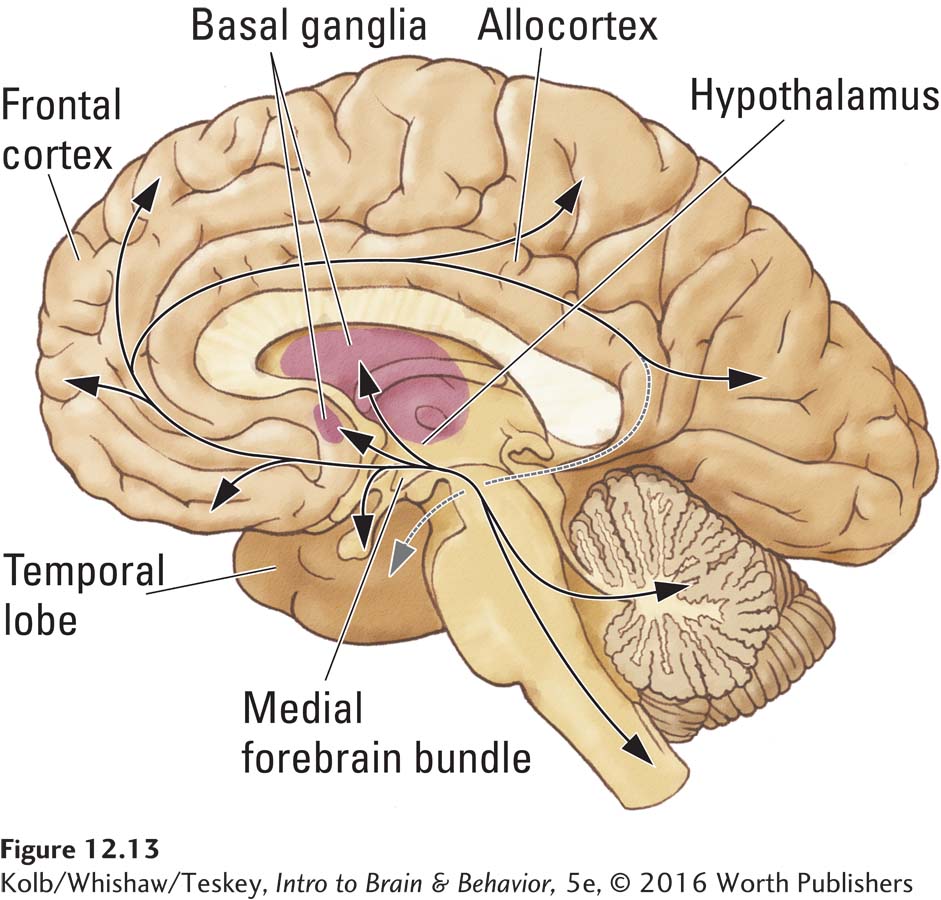
The MFB connects brainstem structures with various parts of the limbic system and forms the activating projections that run from the brainstem to the basal ganglia and frontal cortex. Fibers that ascend from the dopamine-
Section 5-2 reviews the structures and functions of peptide neurotransmitters.
Each hypothalamic nucleus is anatomically distinct, and most have multiple functions, in part because the cells in each nucleus contain a different mix of peptide neurotransmitters. Each peptide participates in different behaviors. For instance, transmitters in the cells in the paraventricular nucleus may be vasopressin, oxytocin, or various combinations of other peptides (such as enkephalin and neurotensin). When peptide neurotransmitters act, we may experience a range of feelings such as well-
413
The production of various neuropeptides hints at the special relation between the hypothalamus and the pituitary. The pituitary consists of distinct anterior and posterior glands, as shown in Figure 12-14. The posterior pituitary is composed of neural tissue and is essentially a continuation of the hypothalamus.
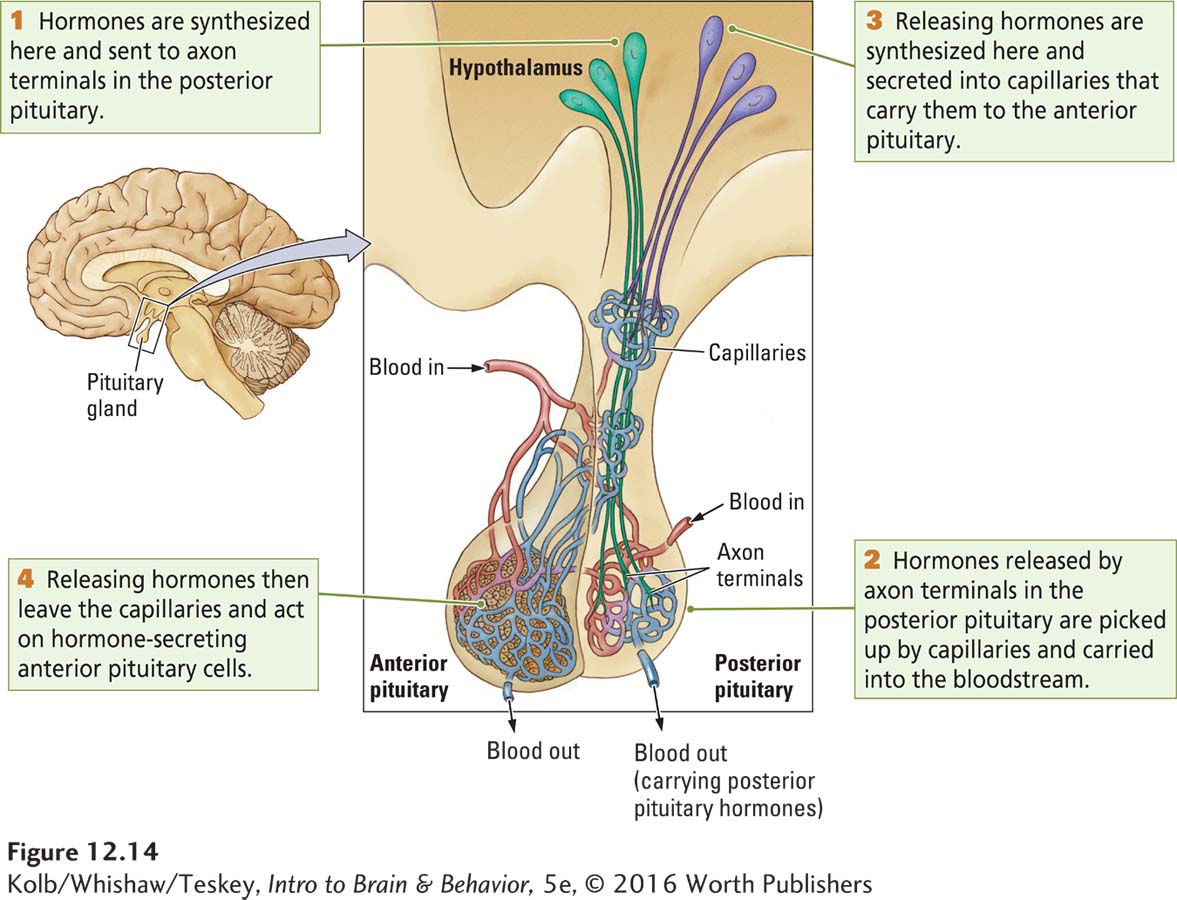
Neurons in the hypothalamus make peptides (e.g., oxytocin and vasopressin) that are transported down their axons to terminals lying in the posterior pituitary. If these neurons become active, they send action potentials to the terminals to release the peptides stored there. But rather than affecting another neuron, as occurs at most synapses, capillaries (tiny blood vessels) in the posterior pituitary’s rich vascular bed pick up these peptides.
The peptides then enter the bloodstream, which carries them to distant targets where they exert their effects. Vasopressin, for example, affects water resorption by the kidneys, and oxytocin controls both uterine contractions and the ejection of milk by mammary glands in the breasts. Peptides can have multiple functions, depending on where their receptors are. Thus, oxytocin not only controls milk ejection in females but also performs a more general role in several forms of affiliative behavior, including parental care, grooming, and sexual behavior in both men and women (Insel & Fernald, 2004).
414
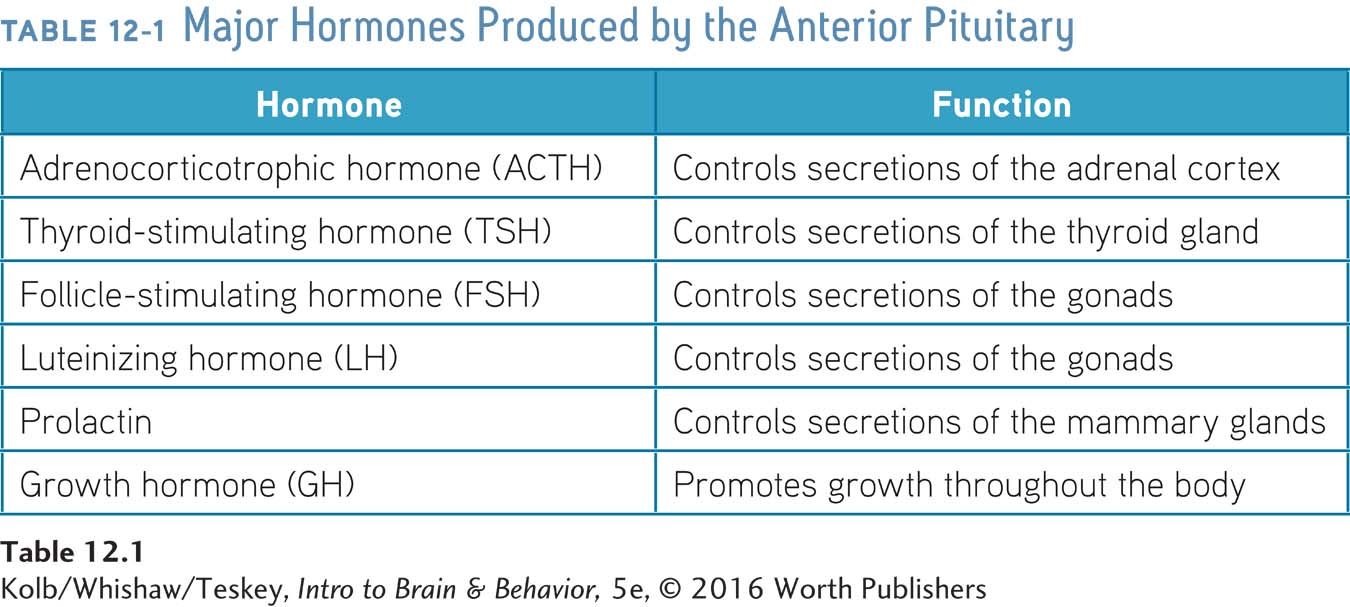
The glandular tissue of the anterior pituitary, by contrast, synthesizes various hormones. The major hormones and their functions are listed in Table 12-1. The hypothalamus controls the release of these anterior pituitary hormones by producing releasing hormones, peptides that act to increase or decrease hormone release. Produced by hypothalamic cell bodies, releasing hormones are secreted into capillaries that transport them to the anterior pituitary, as Figure 12-14 shows.
A releasing hormone can either stimulate or inhibit the release of an anterior pituitary hormone. For example, the anterior pituitary produces the hormone prolactin, but its release is controlled by a prolactin-
FEEDBACK LOOPS When the level of, say, thyroid hormone is low, the hypothalamus releases thyroid-
415
Receptors in the hypothalamus detect the thyroid hormone level. When that level rises, the hypothalamus lessens its secretion of TSH-
The hypothalamus initiates a cascade of events that culminates in hormone secretion, but it pays attention to how much hormone is released. When a certain level is reached, it stops its hormone-
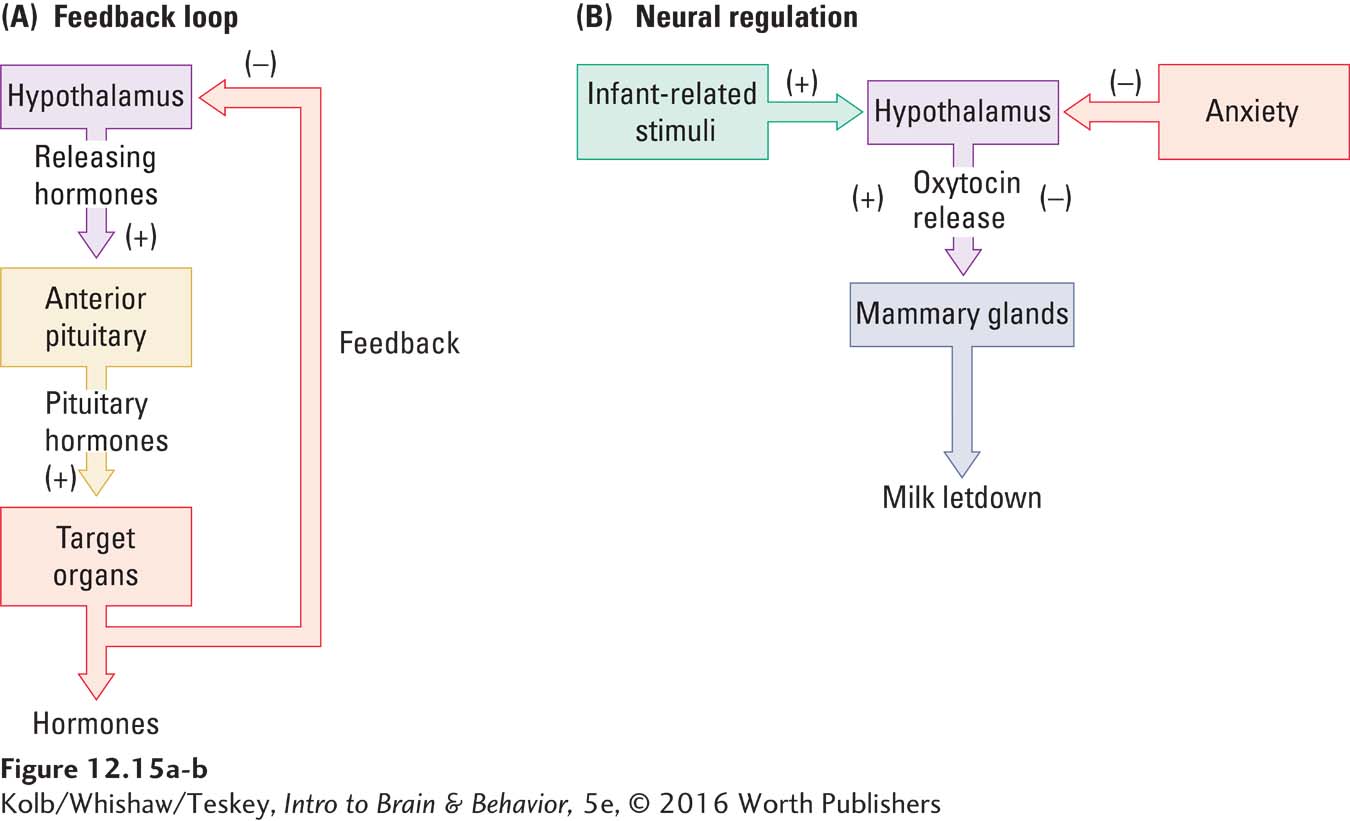
NEURAL CONTROL Hormonal activities of the hypothalamus necessitate regulation by other brain structures, such as the limbic system and the frontal lobes. Figure 12-15B diagrams this neural control in relation to the effects of oxytocin released from the hypothalamus by the paraventricular nucleus, which lies within the periventricular region illustrated in Figure 12-12. As stated earlier, one function of oxytocin is to stimulate cells of the mammary glands to release milk. As shown in Figure 12-15B, when an infant suckles the breast, the tactile stimulation causes hypothalamic cells to release oxytocin, which stimulates milk letdown. In this way, the oxytocin cells participate in a fairly simple reflex that is both neural and hormonal.
Other stimuli can influence oxytocin release, however, which is where control by other brain structures comes in. For example, the sight, sound, or even thought of her baby can trigger a lactating mother to eject milk. Conversely, as diagrammed in Figure 12-15B, feelings of anxiety in a lactating woman can inhibit milk ejection. These excitatory and inhibitory influences exerted by cognitive activity imply that the cortex can influence neurons in the periventricular region. It is likely that projections from the frontal lobes to the hypothalamus perform this role.
EXPERIENTIAL RESPONSES A third control on the hormonal activities of the hypothalamus is the brain’s responses to experience: neurons in the hypothalamus undergo structural and biochemical changes just as cells in other brain regions do. In other words, hypothalamic neurons are like neurons elsewhere in the brain in that they can be changed by heavy demands on them.
Recall the principle of neuroplasticity from Section 2-6.
Such changes in hypothalamic neurons can affect hormone output. For instance, when a woman is lactating, the cells producing oxytocin increase in size to promote oxytocin release and meet the increasing demands of a growing infant for more milk. Through this control, which is mediated by experience, a mother provides her baby with sufficient milk over time.
416
Hypothalamic Involvement in Generating Behavior
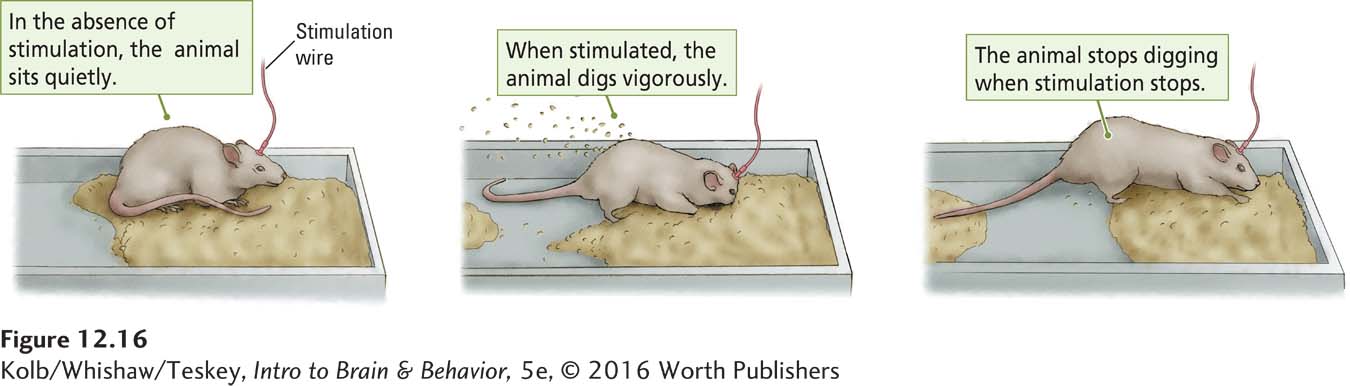
Not only does the hypothalamus control hormone systems, it is also central in generating behavior. This function was first demonstrated by studies in which stimulating electrodes were placed in the hypothalamus of various animals, ranging from chickens to rats and cats. When a small electric current was delivered through a wire electrode, an animal suddenly engaged in some complex behavior—
The onset and termination of these behaviors depended entirely on hypothalamic stimulation. For example, if an electrode in a certain location elicited feeding behavior, the animal ate as soon as the stimulation was turned on and continued to eat until the stimulation was turned off. If the food was removed, however, the animal would not eat but might engage in other behaviors, such as drinking. Recall that Roger, profiled in Section 12-1, ate continuously if foodlike materials were present, corresponding to the continuous hypothalamic activity caused by a tumor.
Figure 12-16 illustrates the effect of stimulation at a site that elicits digging. When no current is delivered, the animal sits quietly. When the current is turned on, the animal vigorously digs in the sawdust; when the current is turned off, the animal stops digging. If the sawdust is removed, it does not dig.
Two more important characteristics of behaviors generated by hypothalamic stimulation are related to (1) survival and (2) reward. Animals apparently find the stimulation of these behaviors pleasant, as suggested by the fact that they willingly expend effort, such as pressing a bar, to trigger the stimulation. Recall that cats kill birds and mice because the act of stalking and killing prey is rewarding to them. Similarly, we can hypothesize that animals eat because eating is rewarding, drink because drinking is rewarding, and mate because mating is rewarding.
Organizing Function of the Limbic Circuit
The limbic circuit derives its name from the Latin limbus, meaning border.
We now turn our attention to parts of the brain that interact with the hypothalamus in generating motivated and emotional behaviors. These brain structures evolved as a ring around the brainstem in early amphibians and reptiles. Nearly 150 years ago, Paul Broca, impressed by this evolutionary development, called these structures the limbic lobe.
Allocortex is found in the brain of mammals and other chordates, especially birds and reptiles.
Known collectively as the limbic system today, these structures are formed from a primitive three-
417
Organization of the Limbic Circuit
As anatomists began to study the limbic structures, connections to the hypothalamus became evident. It also became apparent that the limbic system has a role in emotion. For instance, in the 1930s, James Papez observed that people with rabies display radically abnormal emotional behavior, and postmortem examinations showed that the rabies had selectively attacked the hippocampus. (Definitive proof of rabies remains postmortem hippocampal examination.)
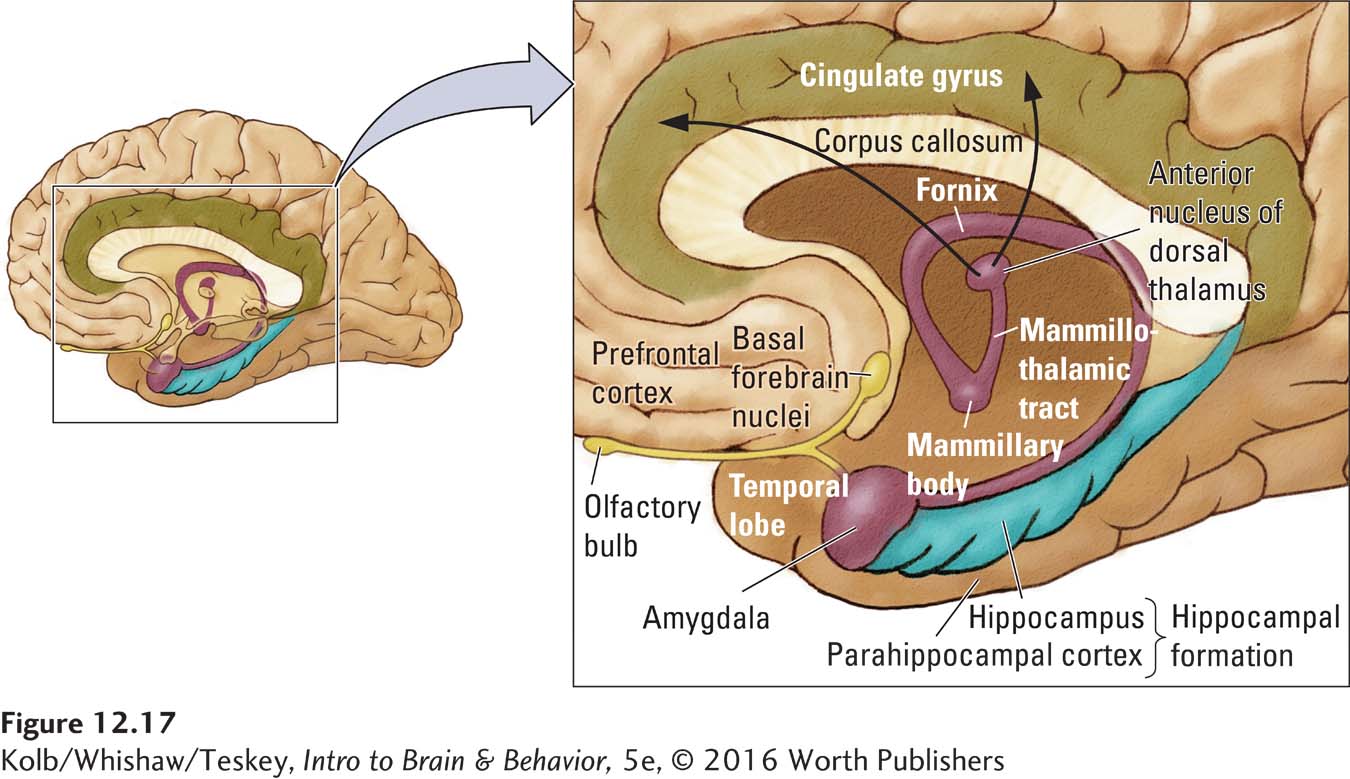
Papez concluded from his observations that the limbic lobe and associated subcortical structures provide the neural basis of emotion. He proposed a neural circuit, traced in Figure 12-18A, now known as the Papez circuit, whereby emotion could reach consciousness, presumed at that time to reside in the cerebral cortex. In 1949, Paul MacLean expanded Papez’s concept of the limbic circuit to include the amygdala and prefrontal cortex. Figures 12-17 and 12-18A show the amygdala lying adjacent to the hippocampus in the temporal lobe, with the prefrontal cortex lying just anterior.
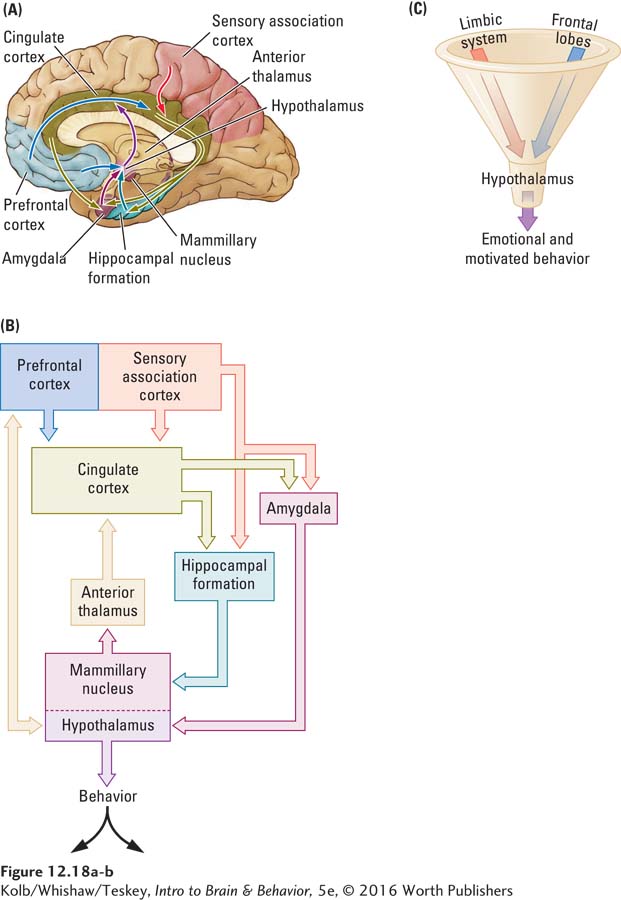
Figure 12-18B charts the limbic circuit schematically. The hippocampus, amygdala, and prefrontal cortex all connect with the hypothalamus. The mammillary nucleus of the hypothalamus connects to the anterior thalamus, which in turn connects with the cingulate cortex. The cingulate cortex completes the circuit by connecting with the hippocampal formation, amygdala, and prefrontal cortex. This anatomical arrangement can be compared to the funnel in Figure 12-18C, which shows the hypothalamus as the spout leading to motivated and emotional behavior.
There is now little doubt that most limbic system structures, especially the amygdala and hypothalamus, take part in emotional behaviors, as detailed later in this section. But most limbic structures perform important roles in various motivated behaviors as well, especially in motivating species-
418
Amygdala
Named for the Greek word for almond because of its shape, the amygdala consists of three principal subdivisions, the corticomedial area, the basolateral area, and the central area. Like the hypothalamus, the amygdala receives inputs from all sensory systems. But in contrast with the hypothalamic neurons, more complex stimuli are necessary to excite amygdalar neurons. Indeed, many amygdalar neurons are multimodal: they respond to more than one sensory modality. In fact, some respond to the entire sensory array: sight, sound, touch, taste, and smell. These amygdalar cells must shape a rather complex image of the sensory world.
Section 15-3 elaborates on multisensory integration and the binding problem.
The amygdala sends connections primarily to the hypothalamus and the brainstem, where it influences neural activity associated with emotions and species-
Amygdala stimulation can also induce eating and drinking. We observed a man who drank water every time the stimulation was turned on. (There happened to be a pitcher of water on the table next to him.) Within 20 minutes, he had consumed about 2 liters of water. When asked if he was thirsty, he said, “No, not really. I just feel like drinking.”
The amygdala’s role in eating can be seen in patients with amygdalar lesions. Like Roger as a result of his tumor, many of these patients lose discrimination in their food choices, eating foods that were formerly unpalatable to them. Lesions of the amygdala may also give rise to hypersexuality.
Executive Function of the Frontal Lobes
The amygdala is intimately connected to the functioning of the frontal lobes that constitute all cortical tissue anterior to the central sulcus. This large area is made up of several functionally distinct regions mapped in Figure 12-19A.
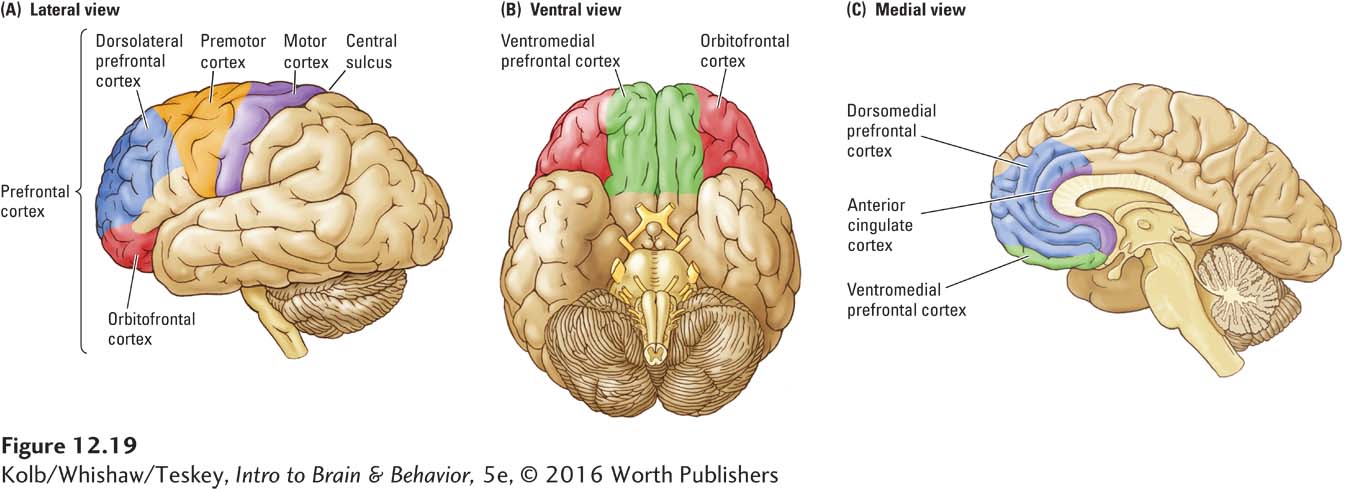
Figure 11-2 charts the hierarchy of frontal lobe regions with regard to movement.
The motor cortex controls fine movements, especially of the fingers, hands, toes, feet, tongue, and face. The premotor cortex participates in selecting appropriate movement sequences. For instance, a resting dog may get up in response to its owner’s call, which serves as an environmental cue for a series of movements processed by one region of the premotor cortex. Or a dog may get up for no apparent reason and wander about the yard, a sequence of actions in response to an internal cue processed by a different premotor region.
419
Prefrontal Anatomy and Connections
Prefrontal literally means in front of the front.
As shown in Figure 12-19A, the prefrontal cortex (PFC) is anterior to the premotor cortex. The PFC is key to controlling executive functions such as planning movements. Its three primary areas are the dorsolateral region; the orbitofrontal cortex (OFC), also shown from a ventral aspect in Figure 12-19B; and the ventromedial PFC. The anterior cingulate cortex (ACC), shown in Figure 12-19C, is closely associated with the PFC, although not strictly part of it.
We focus here on the PFC and motivation and emotion. In Section 15-2 we turn to the PFC and cognition.
The prefrontal cortex contributes to specifying the goals toward which movement should be directed. It controls the processes by which we select movements appropriate to the particular time and context. This selection may be cued by internal information, such as memory and emotion, or it may be made in response to context (environmental information).
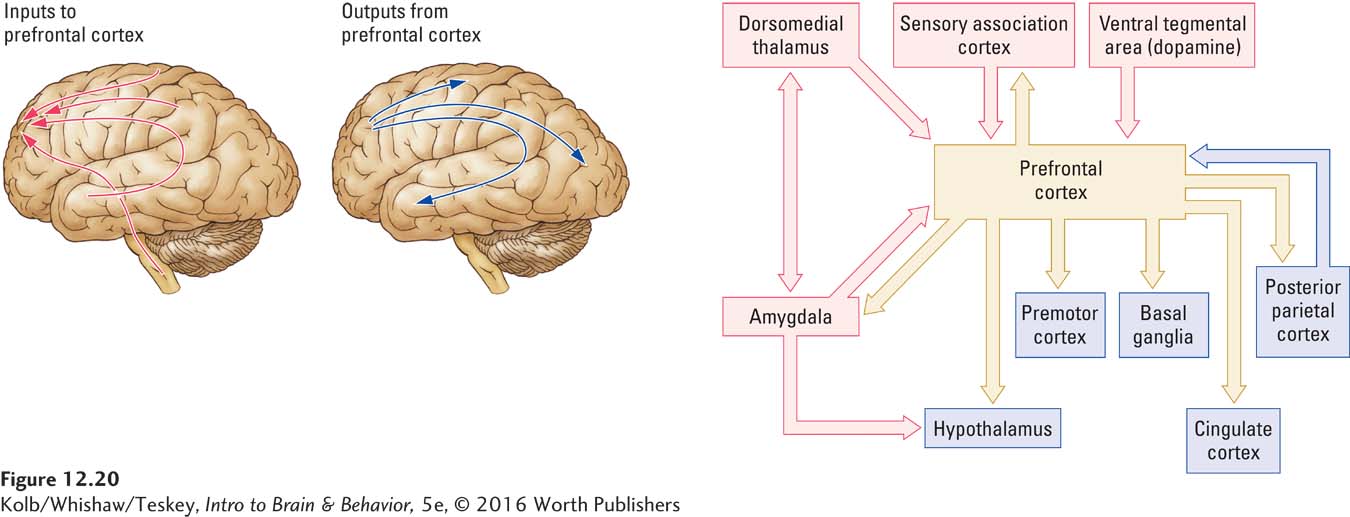
Like the amygdala, the frontal lobes receive highly processed information from all sensory areas, and many neurons in the prefrontal cortex, like those in the amygdala, are multimodal. As shown in Figure 12-20, the prefrontal cortex receives input via connections from the amygdala, dorsomedial thalamus, sensory association cortex, posterior parietal cortex, and the dopaminergic cells of the ventral tegmental area.
Section 16-4 elaborates on the causes of and treatments for schizophrenia.
Dopaminergic input is important for regulating how prefrontal neurons react to stimuli, including emotional ones. Abnormalities in this dopaminergic projection may account for some disorders, including schizophrenia, in which people evince little emotional reaction to typically arousing stimuli.
PFC output influences movement (Section 11-1), memory (Section 14-3), and cognition (Section 15-2).
Figure 12-20 also shows the areas to which the prefrontal cortex sends connections—
Prefrontal Functions
The prefrontal cortex takes part in selecting behaviors appropriate to the particular time and place. Selection may be cued by internal information or made in response to the environmental context. Disruption to this selection function can be seen in people with injury to the dorsolateral frontal lobe (see Figure 12-19A). They become overly dependent on environmental cues to determine their behavior. Like small children, they can be easily distracted by what they see or hear. We have all experienced a loss of concentration to some extent, but for a patient with frontal lobe damage, the problem is exaggerated and persistent. Because the person becomes so absorbed in irrelevant stimuli, he or she cannot act on internalized information most of the time.
420
A good example is J. C., in whom bilateral damage to the dorsolateral prefrontal cortex resulted from having a tumor removed. J. C. would lie in bed most of the day fixated on television programs. He was aware of his wife’s opinion of this behavior, but only the sound of the garage door opening when she returned home from work in the evening would stimulate him into action. Getting out of bed was controlled by this specific environmental cue; without it, he seemed to lack motivation. Television completely distracted him from acting on internal knowledge of things that he could or should do.
Adapting behavior appropriately to the environmental context also is a PFC function. Most people readily change their behavior to match the situation at hand. We behave one way with our parents, another with our friends, another with our children, and yet another with our coworkers. Each set of people constitutes a different context, and we shift our behaviors accordingly. Our tone of voice, our use of slang or profanity, and the content of our conversations are quite different in different contexts.
Even among our peers we act differently, depending on who is present. We may be relaxed in the presence of some people and ill at ease with others. It is therefore no accident that the size of the frontal lobes is related to species’ sociability. Social behavior is extremely rich in contextual information, and humans are highly social animals.
Focus 1-1 and Section 1-2 recount behavioral effects of TBI; Section 14-5 details recovery; Section 16-3 explores TBI symptoms and treatments.
Controlling behavior in context requires detailed sensory information, which is conveyed from all sensory regions to the frontal lobes. This sensory input includes not only information from the external world but also internal information from the ANS. People with damage to the orbital prefrontal cortex, as is common in traumatic brain injuries, have difficulty adapting their behavior to the context, especially the social context. Consequently, they often make social gaffes.
Section 15-2 considers the frontal lobes and the executive function of planning.
In summary, the role of the frontal lobes in selecting behaviors is important for considering what causes behavior. The frontal lobes act much like a composer, but instead of selecting notes and instruments, they select our actions. Not surprisingly, the frontal lobes are sometimes described as housing the brain’s executive functions. To grasp the full extent of frontal lobe control of behavior, see Clinical Focus 12-2, Agenesis of the Frontal Lobe.
CLINICAL FOCUS 12-2
Agenesis of the Frontal Lobes
The role of the frontal lobes in motivated behavior is perhaps best understood by looking at J. P.’s case, described in detail by Stafford Ackerly (1964). Born in December 1914, J. P. was a problem child. Early on, he became a wanderer. Policemen would find him miles from home, as he had no fear of being lost. Severe whippings by his father did not deter him.
J. P.’s behavioral problems continued and expanded as he grew older, and by adolescence, he was constantly in trouble. Yet J. P. also had a good side. When he started school, his first-
As she was composing the letter, she looked up to find J. P. exposing himself to the class and masturbating. This juxtaposition of polite manners and odd behavior characterized J. P.’s conduct throughout his life. At one moment he was charming; at the next he was engaged in socially unacceptable behavior.
J. P. developed no close friendships with people of either sex, in large part because of his repeated incidents of public masturbation, stealing, excessive boastfulness, and wandering. He was a person of average intelligence who seemed unaffected by the consequences of his behavior. Police officers, teachers, and neighbors all ascribed intention to J. P.’s behavior: all believed that he was willfully misbehaving and blamed his parents for not enforcing sufficiently strict discipline.
Perhaps as a result, not until he was 19 years old was J. P.’s true condition detected. To prevent him from serving a prison term for repeated automobile theft, a lawyer suggested that J. P. undergo psychiatric evaluation. The psychiatrist who examined him ordered an X-
Failure of a structure to develop is known as agenesis; J. P.’s condition was agenesis of the frontal lobes. His case offers an unusual opportunity to study the role of the frontal lobes in motivated behavior.
Clearly, J. P. lacked the bag of mental tricks that most people use to come to terms with the world. Normally behavior is affected both by its past consequences and by current environmental input. J. P. did not seem much influenced by either factor. As a result, the world was simply too much for him. He always acted childlike and was unable to formulate plans or to inhibit many of his behaviors. He acted on impulse. At home, he was prone to aggressive outbursts about small matters, especially with regard to his mother.
Curiously, J. P. seemed completely unaware of his life situation. Even though the rest of his brain was working fairly well—
Stimulating and Expressing Emotion
421
Emotion, like motivation, is intangible: it is an inferred state. But the importance of emotion to our everyday lives is hard to exaggerate. Emotion can motivate us. It inspires artistic expression, for example, from poetry to filmmaking to painting. Many people enjoy the arts simply because they evoke emotions. And while people find certain emotions pleasant, severe and prolonged negative emotions, especially anxiety and depression, can cause clinical disorders.
To explore neural control of emotions, we must first specify the types of behavior we want to explain. Think of any significant emotional experience you’ve had recently. Perhaps you had a serious disagreement with a close friend. Maybe you just got engaged to be married.
A common characteristic of such experiences includes autonomic responses such as rapid breathing, sweating, and dry mouth. Emotions may also entail strong subjective feelings that we label as anger, fear, or love, among others. Finally, emotions typically entail thoughts or plans related to the experience itself and may take the form of replaying conversations and events in your mind, anticipating what you might say or do under similar circumstances in the future or in planning your married life.
These three forms of emotional experience suggest the influence of different neural systems. The autonomic component must include the hypothalamus and associated structures, as well as the enteric nervous system. The components of subjective feelings are more difficult to localize but clearly include the amygdala and probably parts of the frontal lobes. And thoughts and plans are likely to be cortical. What is the relation between our cognitive experience of an emotion and the associated physiological changes?
One view is that physiological changes (such as trembling and rapid heartbeat) come first, and the brain then interprets these changes as an emotion. This perspective implies that the brain (most likely the cortex) produces a cognitive response to autonomic information. That response varies with the context in which the autonomic arousal occurs, including the effects on the gut via the ENS. In cases of extreme autonomic activity, serotonin release surges in the gut, which can lead to diarrhea and cramping. If we are frightened by a movie, we feel a weaker, shorter-
Two lines of evidence support the James–
The second line of evidence supporting the view that physiological changes are the starting point for emotions comes from people with reduced information about their own autonomic arousal, for example, owing to spinal cord injury. Spinal injury results in a decrease in perceived emotion, and its severity depends on how much sensory input is lost. Figure 12-21 illustrates this relation. People with the greatest loss of sensory input, which occurs with injuries at the uppermost end of the spinal cord, also have the greatest loss of emotional intensity. In contrast, people with low spinal injuries retain most of their visceral input and have essentially typical emotional reactions.
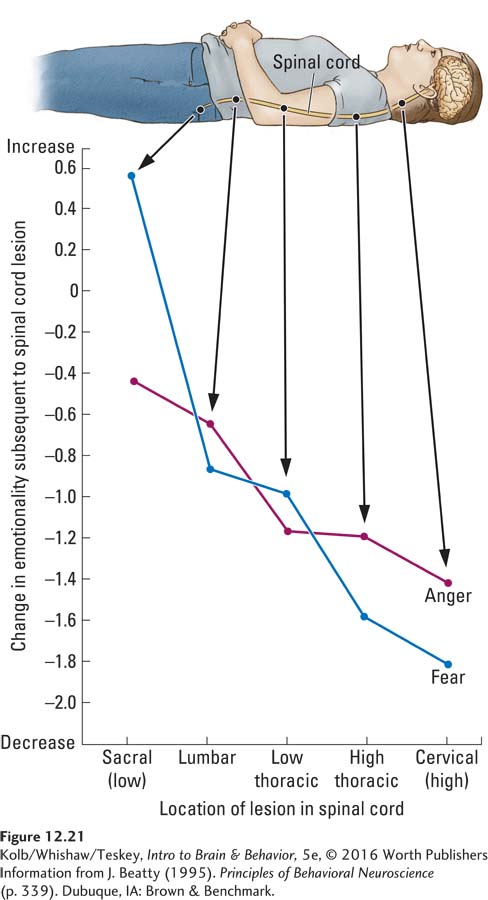
After Christopher Reeve’s spinal cord was severed at the cervical level (high), his emotions may have been blunted, but his motivation clearly remained intact. See Section 11-1.
Antonio Damasio (1999) emphasized an important additional aspect of the link between emotional and cognitive factors in his somatic marker hypothesis. When Damasio studied patients with frontal lobe injuries, he was struck by how they could be highly rational in analyzing the world yet still make decidedly irrational social and personal decisions. The explanation, he argued, is that the neural machinery underlying emotion no longer affectsthe reasoning of people with frontal lobe injury, either consciously or unconsciously. Cut off from critical emotional input, many social and personal decisions suffer.
422
The grizzly bear attack recounted in Section 11-4 confirms the primacy of emotion—
To account for these observations, Damasio proposed that emotions are responses induced by either internal or external stimuli not normally attended to consciously. For example, if you encounter a bear as you walk down the street (presuming that you live in a place where this event could take place), the stimulus is processed rapidly without conscious appraisal. In other words, a sensory representation of the bear in the visual cortex is transmitted directly to brain structures, such as the amygdala, that initiate an emotional response.
This emotional response includes actions on structures in the forebrain and brainstem and ultimately on the ANS. The amygdala has connections to the frontal lobes, so the emotional response can influence the frontal lobes’ appraisal. But if the frontal lobes are injured, emotional information is excluded from cognitive processing, so the quality of emotion-
To summarize, Damasio’s somatic marker hypothesis proposes how emotions are normally linked to a person’s thoughts, decisions, and actions. In a typical emotional state, certain brain regions send messages to many other brain areas and to most of the rest of the body through hormones and the ANS. These messages produce a global change in the organism’s state, and the altered state influences behavior, often unconsciously.
Amygdala and Emotional Behavior
In addition to controlling certain species-
Tameness and loss of fear
Indiscriminate dietary behavior (eating many types of formerly rejected foods)
Greatly increased autoerotic, homosexual, and heterosexual activity with inappropriate object choice (e.g., the sexual mounting of chairs)
Tendency to attend to and react to every visual stimulus
Tendency to examine all objects by mouth
Visual agnosia, an inability to recognize objects or drawings of objects
Section 9-4 describes varieties of visual form agnosia in a range of case studies.
Visual agnosia results from damage to the ventral visual stream in the temporal lobe, but the other symptoms are related to the amygdalectomy. Tameness and loss of fear are especially striking. Monkeys that normally show a strong aversion to stimuli such as snakes show no fear of them whatsoever. In fact, amygdalectomized monkeys may pick up live snakes and even put them in their mouth.
Focus 2-2 examines some causes and symptoms of encephalitis.
Although Klüver–
The amygdala’s role in Klüver–
Throughout human history, exploiting fear has proved especially effective in controlling group behavior.
423
Awareness of danger and of safety has both an innate and a learned component, as Joe LeDoux (1996) emphasized. The innate component, much as in the IRMs described in Section 12-3, is the automatic processing of species-
A rat that has never encountered a ferret thus shows an immediate fear response to the odor of ferret. Other novel odors (such as peppermint or coffee) do not produce an innate fear reaction. The innate response triggers in the rat an autonomic activation that stimulates conscious awareness of danger.
In contrast, the learned component of fear consists of the avoidance of specific animals, places, and objects that the organism has come to associate with danger. The organism is not born with this avoidance behavior prewired. In a similar way, animals learn to increase contact with environmental stimuli that they associate with positive outcomes, such as food or sexual activity or, in the laboratory, drugs. Damage to the amygdala interferes with all these behaviors. The animal loses not only its innate fears but also its acquired fears of and preferences for certain environmental stimuli.
To summarize, a species’ survival requires a functioning amygdala. It influences autonomic and hormonal responses through its connections to the hypothalamus. It influences our conscious awareness of the positive and negative consequences of events and objects through its connections to the prefrontal cortex.
Prefrontal Cortex and Emotional Behavior
At about the same time that Klüver and Bucy began studying their monkeys, Carlyle Jacobsen was studying the effects of frontal lobotomy on the cognitive capacities of two chimpanzees. A frontal lobotomy destroys substantial brain tissue as the result of inserting a sharp instrument into the frontal lobes and moving it back and forth.
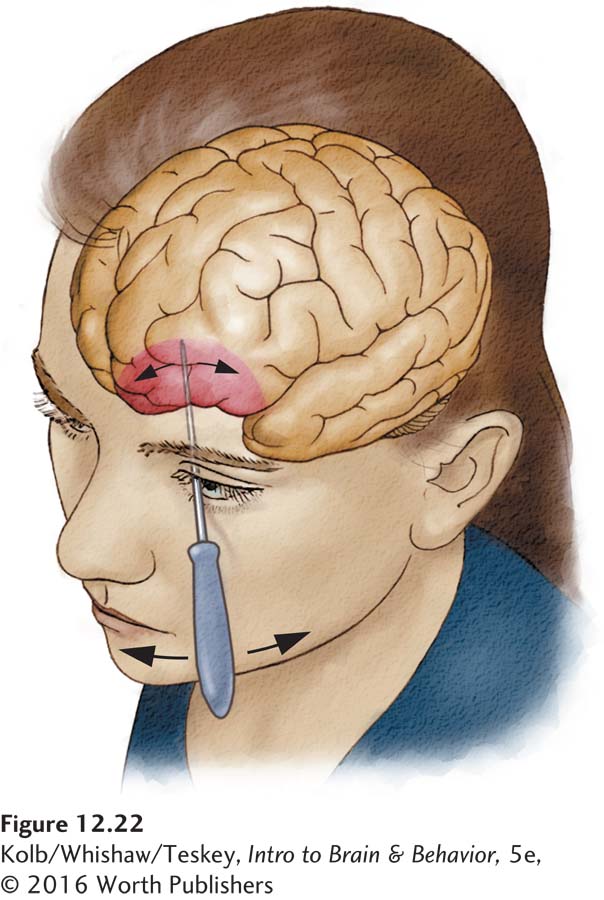
In 1936, Jacobsen reported that one of the chimps was particularly neurotic before being subjected to this procedure. It became more relaxed afterward. Incredibly, a leading Portuguese neurologist of the time, Egas Moniz, seized on this observation as a treatment for behavioral disorders in humans, and the frontal lobotomy, illustrated in Figure 12-22, was initiated as the first technique of psychosurgery, or neurosurgery intended to alter behavior.
The use of psychosurgery grew rapidly in the 1950s. In North America alone, nearly 40,000 people received frontal lobotomies as a treatment for psychiatric disorders. Not until the 1960s was any systematic research conducted into the effects of frontal lesions on social and emotional behavior. By this time, the frontal lobotomy had virtually vanished as a “treatment.” We now know that prefrontal lesions in various species, including humans, severely affect social and emotional behavior.
Agnes is a case in point. We met Agnes at the psychiatric hospital where we met Roger (whose indiscriminate eating we described in Section 12-1). At the time, Agnes, a 57-
The first thing we noticed about Agnes was that she exhibited no outward sign of emotion. She showed virtually no facial expression. Agnes had been subjected to a procedure known as a frontal leukotomy because her husband, an oil tycoon, felt that she was too gregarious. Evidently, he felt that her “loose lips” were a detriment to his business dealings. He convinced two psychiatrists that she would benefit from psychosurgery, and her life was changed forever.
To perform a leukotomy, as illustrated in Figure 12-22, a surgeon uses a special knife called a leukotome to sever the connections of a region of the orbitofrontal cortex (see Figure 12-19). In our conversations with Agnes, we quickly discovered her considerable insight into the changes brought about by the leukotomy. In particular, she indicated that she no longer had any feelings about things or most people, although, curiously, she was attached to her dog. She said that she often just felt empty and much like a zombie.
424
Agnes’s only moment of real happiness in the 30 years since her operation was the sudden death of her husband, whom she blamed for ruining her life. Unfortunately, Agnes had squandered her dead husband’s considerable wealth as a consequence of her inability to plan or organize. This inability, we have seen, is another symptom of prefrontal injury.
The orbitofrontal area has direct connections with the amygdala and hypothalamus. Its stimulation can produce autonomic responses, and as we saw in Agnes, damage to the orbital region can produce severe personality change characterized by apathy and loss of initiative or drive. The orbital cortex is probably responsible for the conscious awareness of emotional states produced by the rest of the limbic system, especially the amygdala.
ASD is the topic of Focus 8-2; schizophrenia, of Focus 8-5.
Agnes’s loss of facial expression is also typical of frontal lobe damage. In fact, people with frontal lobe injuries and people who have schizophrenia or autism spectrum disorder are usually impaired at both producing and perceiving facial expressions, including a wide range of expressions found in all human cultures—
Although facial expression is a key to recognizing emotion, so is tone of voice, or prosody. Patients with damage to the frontal lobe are devoid of prosody, both in their own conversations and in understanding the prosody of others. The lost ability to comprehend or produce emotional expression in both faces and language partly explains those patients’ apathy. In some ways, they are similar to spinal cord patients who have lost autonomic feedback and so can no longer feel the arousal associated with emotion. These patients can no longer either read emotion in other people’s faces and voices or express it in their own.
Some psychologists have proposed that our own facial expressions provide us with important clues to what we are feeling. This idea has been demonstrated in experiments reviewed by Pamela Adelmann and Robert Zajonc (1989). In one such study, people were required to contract their facial muscles by following instructions about which parts of the face to move. Unbeknown to the participants, the movements produced happy and angry expressions. Afterward, they viewed a series of slides and reported how the slides made them feel.
They said that they felt happier when they were inadvertently making a happy face and angrier when making the angry face. Patients with frontal lobe damage presumably have no such feedback from their own facial expressions, which could contribute to their emotional experiences being dampened.
Emotional Disorders
Major depression, detailed in Focus 6-3, is among the most treatable psychological disorders. Cognitive and intrapersonal therapies are as effective as drugs. See Section 16-4.
Major depression, a highly disruptive emotional disorder, is characterized by some or all the following: prolonged feelings of worthlessness and guilt, the disruption of normal eating habits, sleep disturbances, a general slowing of behavior, and frequent thoughts of suicide. A depressed person feels severely despondent for a long time. Major depression is common in our modern world, with a prevalence of about 6 percent of the population at any given time.
Depression has a genetic component. It not only runs in families but also frequently tends to occur in both members of a pair of identical twins. The genetic component in depression implies a biological abnormality, but the cause remains unknown. However, neuroscience researchers’ interest in the role of epigenetic changes in depression is increasing. One hypothesis is that early life stress may produce epigenetic changes in the prefrontal cortex (see the review by Schroeder et al., 2010).
Excessive anxiety is an even more common emotional problem than depression. Anxiety disorders, including posttraumatic stress disorder (PTSD), phobias, generalized anxiety disorder, panic disorder, and obsessive-
425
CLINICAL FOCUS 12-3
Anxiety Disorders
Animals typically become anxious at times, especially when they are in obvious danger. But anxiety disorders are different. They are characterized by intense feelings of fear or anxiety inappropriate for the circumstances. People with an anxiety disorder have persistent and unrealistic worries about impending misfortune. They also tend to have multiple physical symptoms attributable to hyperactivity of the sympathetic nervous system.
G. B.’s case is a good example. He was a 36-
Extensive medical testing and multiple attacks over about 2 years eventually led to the diagnosis of generalized anxiety disorder. Like most of the 5 percent of the U.S. population who have an anxiety disorder at some point in their life, G. B. was unaware that he was overly anxious. The cause of generalized anxiety is difficult to pinpoint, but one likely explanation is related to the cumulative effect of general stress.
Although G. B. appeared outwardly calm most of the time, he had been a prodemocracy activist in communist Poland, a dangerous position. Because of the dangers, he and his family eventually escaped from Poland to Turkey, and from there they went to Canada. G. B. may have had continuing worries about the repercussions of his political activities—
The most common and least disabling type of anxiety disorders are phobias. A phobia pertains to a clearly defined, dreaded object (such as spiders or snakes) or situation (such as enclosed spaces or crowds). Most people have a mild aversion to some types of stimuli. Such aversion becomes a phobia only when a person’s feelings about a disliked stimulus lead to overwhelming fear and anxiety.
The incidence of disabling, that is, serious enough to interfere with living well, phobias is surprisingly high—
Panic disorder has an estimated incidence on the order of 3 percent of the population. Symptoms include recurrent attacks of intense terror that begin without warning and without any apparent relation to external circumstances. Panic attacks usually last only a few minutes, but the experience is always terrifying. Sudden activation of the sympathetic nervous system leads to sweating, a wildly beating heart, and trembling.
Although panic attacks may occur only occasionally, the victim’s dread of another episode may be continual. Consequently, many people with panic disorder also have agoraphobia, a fear of public places or situations in which help might not be available. This phobia makes some sense, because a person with a panic disorder may feel particularly vulnerable about the possibility of having an attack in a public place.
Freud believed that anxiety disorders are psychological in origin and treatable with talking therapies in which people confront their fears. Today, cognitive-
Pharmacologically, anxiety disorders are most effectively treated with benzodiazepines such as diazepam (Valium), the best known. Alprazolam (Xanax) is the most commonly prescribed drug for panic attacks. Benzodiazepines act by augmenting GABA’s inhibitory effect and are believed to exert a major influence on neurons in the amygdala.
Whether treatments are behavioral, pharmacological, or both, the general goal is normalizing brain activity in the limbic system.

426
Figure 6-7 illustrates antianxiety agents’ action at the GABAA receptor.
As with depression, the root cause of anxiety disorders is unknown, but the effectiveness of the drug treatments described in Clinical Focus 12-3 implies a biological basis. The most widely prescribed anxiolytic (antianxiety) drugs are the benzodiazepines, such as Valium, Librium, and Xanax. Why would the brain have a mechanism for benzodiazepine action? It certainly did not evolve to allow us to take Valium. Probably this mechanism is part of a system that both increases and reduces anxiety levels. The mechanism for raising anxiety seems to entail a compound known as diazepam-
Section 16-4 further explores anxiety disorders and reviews treatments.
Increased anxiety can be beneficial, especially if we are drowsy and need to be alert to deal with a crisis. Impairment of this survival mechanism or the one that reduces anxiety can cause serious emotional problems, even anxiety disorders.
12-4 REVIEW
Neuroanatomy of Motivated and Emotional Behavior
Before you continue, check your understanding.
Question 1
The two types of motivated behaviors are ______________ behaviors, which maintain homeostasis, and ______________ behaviors, encompassing basically all other behaviors.
Question 2
The brain’s homeostat for many functions is found in the ______________.
Question 3
The three brain structures housing the major behavioral circuitry involved in motivation and emotion are ______________ , ______________ , and ______________.
Question 4
The prefrontal cortex has three main subdivisions: ______________ , ______________ , and ______________.
Question 5
Damage to the ______________ is the primary cause of Klüver–
Question 6
The anterior pituitary gland produces ______________.
Question 7
Contrast the functions of the limbic system and the frontal lobes.
Answers appear in the Self Test section of the book.