13-3 Sleep Stages and Dreaming
Waking behavior encompasses periods when we are physically active or inactive, and so does sleep. Our sleeping behavior consists of periods of rest, napping, long bouts of sleep, and sleep-
| Recommended Sleep Duration by Age | |
|---|---|
| Age | Sleep time (hours) |
| Newborn up to 3 months | 14– |
| Infant under 1 year | 12– |
| Toddler up to 3 years | 11– |
| Preschool | 10– |
| Elementary- |
9– |
| Adolescent |
8– |
| Adult |
7– |
| Adult 65 years and older |
7– |
Measuring How Long We Sleep
A crude measure of sleeping and waking behavior is the self-
Some people nap for a brief period in the daytime; others never nap. Benjamin Franklin is credited with the aphorism “early to bed and early to rise makes a man healthy wealthy and wise,” but measures of sleep behavior indicate that the correlation Franklin proposed does not actually exist. Variations in sleeping times are normal, and napping normally is good.
Measuring Sleep in the Laboratory
457
Laboratory sleep studies allow researchers to measure sleep accurately and to record physiological changes associated with sleep. Miniaturized sleep-
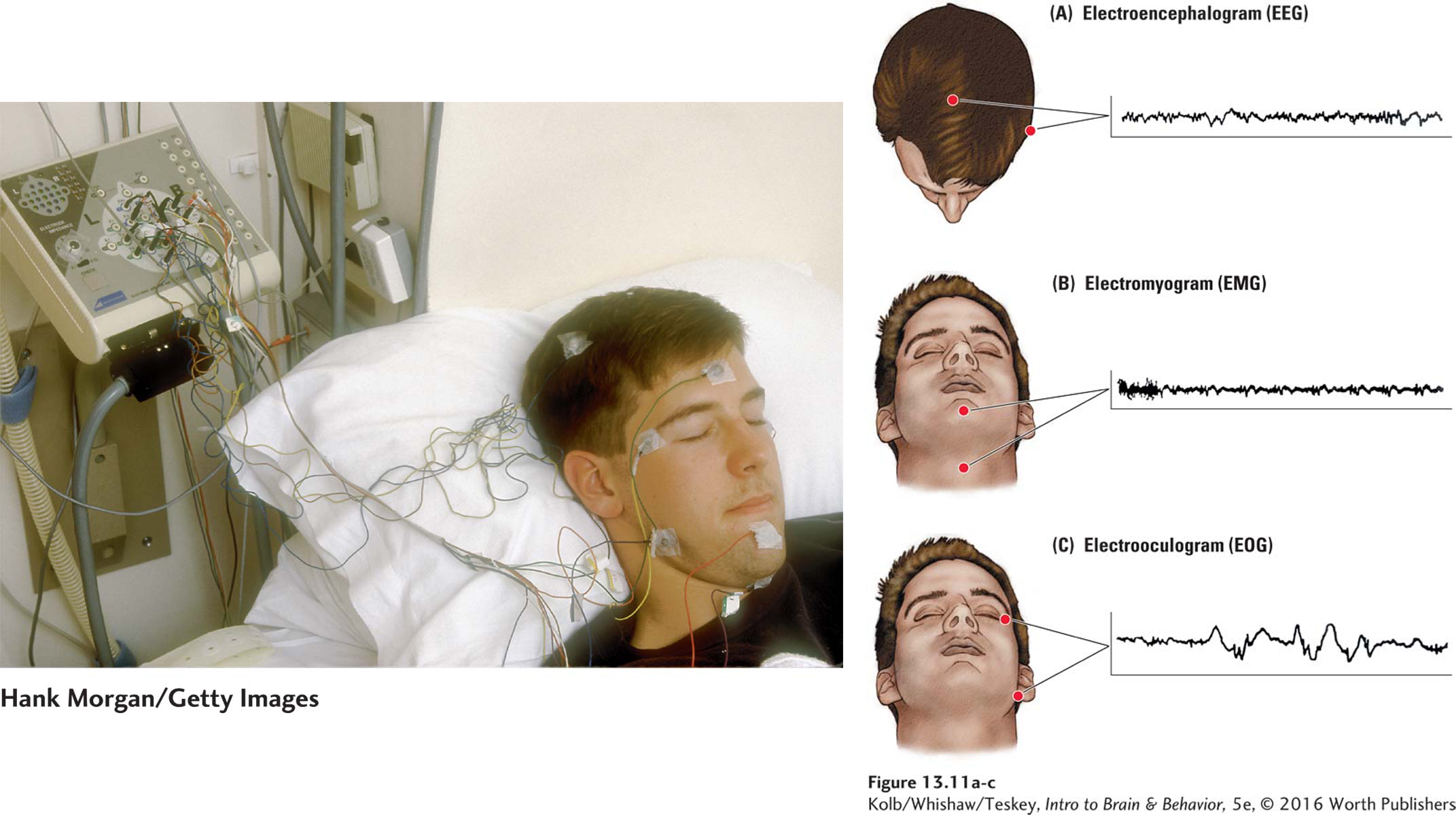
Electrodes pasted onto standard locations on the skull’s surface yield an electroencephalogram (EEG), a record of brain wave activity. Electrodes placed on neck muscles provide an electromyogram (EMG), a record of muscle activity. Electrodes located near the eyes provide an electrooculogram (EOG), a record of eye movements. Body temperature, circulating hormones, and blood glucose levels provide additional measures of sleep.
Stages of Waking and Sleeping
Figure 7-9 diagrams EEG patterns that reflect a range of conscious states in humans.
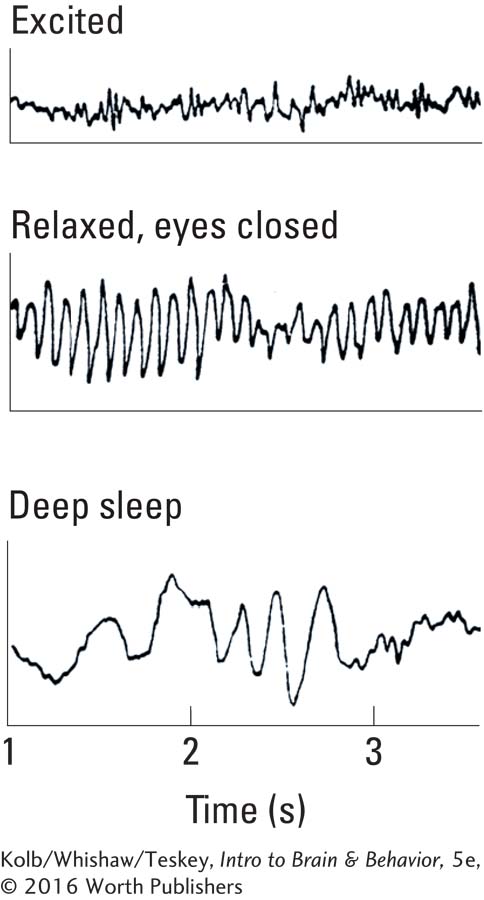
Biological measurements show that sleep, like waking, is not a unitary state but encompasses several stages. For example, the EEG recording shows distinct patterns of brain wave activity as the neocortex generates distinct rhythmic patterns for states categorized as awake, relaxed, drowsy, sleep, deep sleep, and dreaming.
Waking State
When a person is awake, the EEG pattern consists of small-
458
Relaxed State
When participants relax and close their eyes, they may produce the alpha (α) rhythm—large, extremely regular brain waves with a frequency ranging from 7 to 11 Hz. Humans generate alpha rhythms in the region of the visual cortex at the back of the brain, and the rhythms abruptly stop if a relaxed person is disturbed or opens his or her eyes. Not everyone displays alpha rhythms, and some people display them much better than others.
Drowsy State
When a person grows drowsy, the EEG indicates that beta wave activity in the neocortex gives way to slower EEG wave activity. The amplitude of the EEG waves increases and their frequency becomes a slower theta (θ) rhythm of 4-
Sleeping State
As participants enter deeper sleep, they produce yet slower, larger EEG waves called delta (δ) rhythms. Delta rhythm has a frequency of 1 to 3 Hz and is associated with the loss of consciousness that characterizes sleep. This stage is sometimes called slow-
REM and NREM Sleep Phases
Sleep consists of periods when a sleeper is relatively still and periods when the mouth, fingers, and toes twitch. This behavior is readily observed in household pets and bed partners. In 1955 Eugene Aserinsky and Nathaniel Kleitman (Lamberg, 2003), working at the University of Chicago, observed that the twitching is periodic and is also associated with rapid eye movements (REM). Other than twitches and eye movements, the EMG indicates that muscles are inactive, a condition termed atonia (Greek via Latin, “without tone”).
By accumulating and analyzing REM recorded on EEGs, the Chicago investigators were the first to identify REM sleep, a fast-
Other Sleep-
Although electrophysiological measures define the sleep stages, many other bodily and physiological events are associated with waking and sleep stages. Measures of metabolic activity, such as body temperature, generally decline during sleep. Breathing and heart rate provide further insights into waking and sleeping. The sleeper’s behavior—
A Typical Night’s Sleep
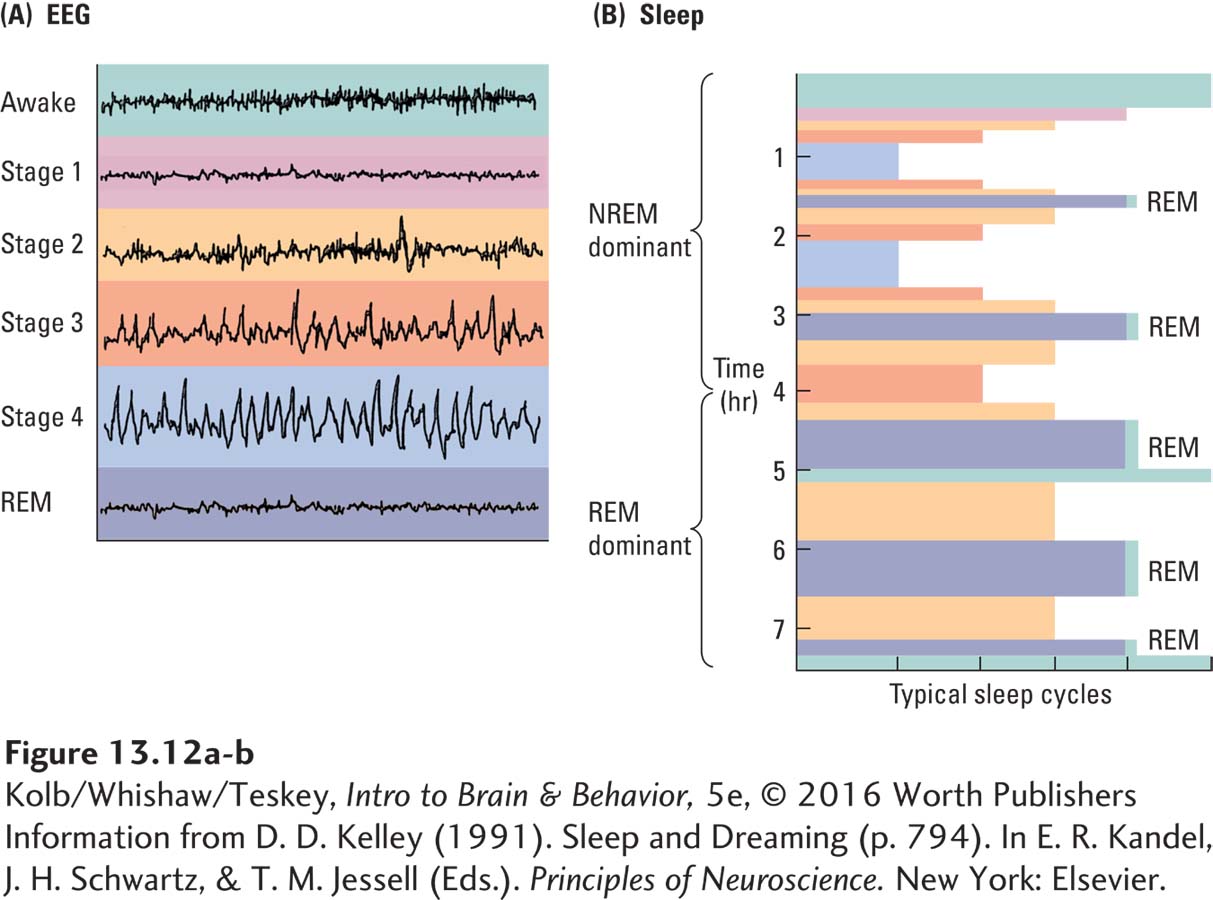
Figure 13-12A displays the EEG patterns associated with waking, NREM sleep, and REM sleep from a typical night’s sleep. NREM sleep is divided into four stages on the basis of EEG recordings. The main change in the progression from stage 1 sleep through stage 4 sleep is the increased size and slowing speed of brain waves.
The designation of these stages assumes that the sleeper moves from relatively shallow sleep in stage 1 to deep sleep in stage 4. Self-
459
Figure 13-12B graphs one participant cycling through these stages in the course of a night’s sleep. Notice that the depth of sleep changes several times through the four stages of NREM sleep, then entry into REM sleep. This NREM–
The labels indicating REM sleep in Figure 13-12B tell us that the sleep stage durations roughly divide sleep into two parts, the first dominated by NREM sleep, the second dominated by REM sleep. Separate measures of body temperature record that it is lowest (about 1.5°C below a normal temperature of 37.7°C) during the earlier NREM-
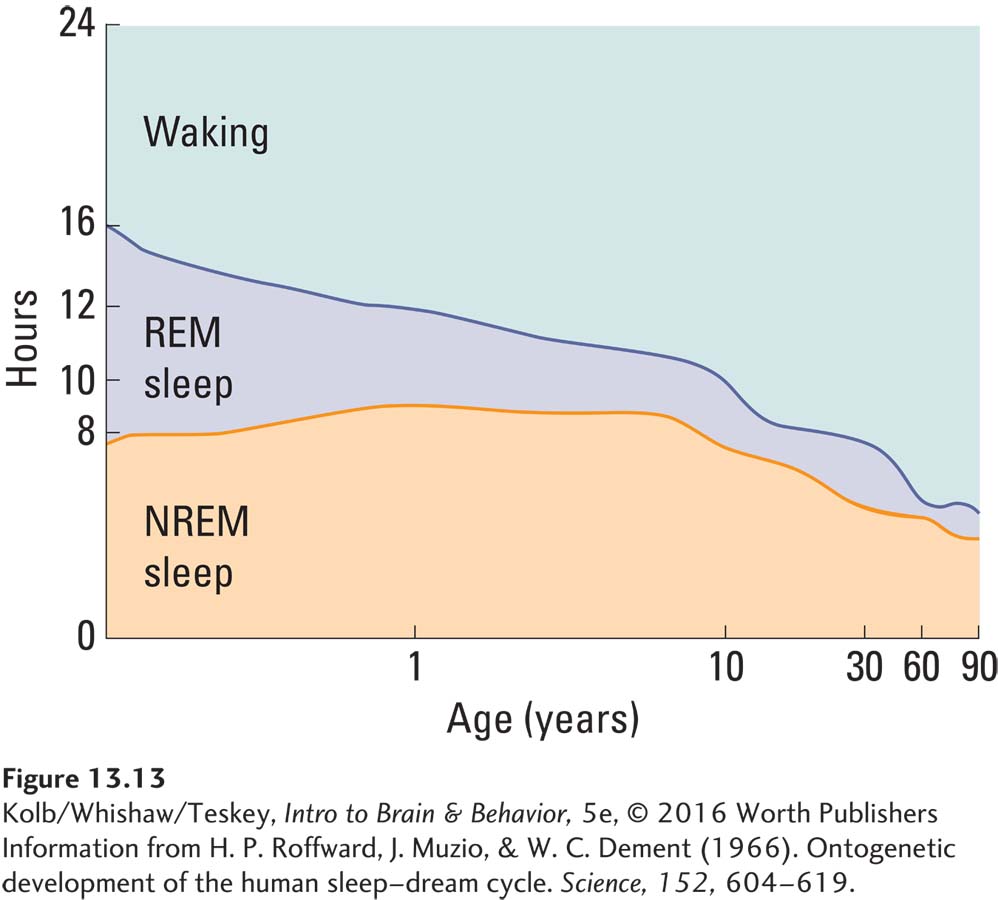
Findings from sleep laboratory studies confirm that individuals tend to conform to this sleep pattern with some variability. Studies also confirm that REM sleep takes up substantial time: adults who typically sleep about 8 hours spend about 2 of those hours in REM. A person’s duration of REM sleep varies at different times of life and changes dramatically over the life span. Periods of REM sleep are high in infancy; they increase during growth spurts, in conjunction with physical exertion, and during pregnancy. Figure 13-13 shows that most people sleep less as they grow older. In the first 2 years of life REM sleep makes up nearly half of sleep time, but it declines proportionately until in middle age it constitutes little more than 10 percent of sleep time.
Contrasting NREM Sleep and REM Sleep
Although it seems an inactive period, a remarkable range of activity takes place during sleep. Events associated with NREM sleep and REM sleep, for example, are dramatically different, not only in physiological measures but also in such behavioral events as cognition, memory storage, and sleep disorders.
During NREM sleep body temperature declines, heart rate and blood flow decrease, body weight decreases from water loss in perspiration, and growth hormone levels increase. NREM sleep is also the time when we toss and turn in bed, pull on the covers, and engage in other movements. (For an extreme example see Clinical Focus 13-4, Restless Legs Syndrome.) If we talk in our sleep or grind our teeth, we do so during NREM sleep. If we flail, banging an arm or kicking a foot, we usually do so in NREM sleep. Some people even get up and walk around, and this sleepwalking takes place during NREM sleep. All this activity during our so-
460
CLINICAL FOCUS 13-4
Restless Legs Syndrome
I’ve always been a fairly untalented sleeper. Even as a child, it would take me some time to fall asleep, and I would often roll around searching for a comfortable position before going under. But my real difficulties with sleeping did not manifest themselves until early adulthood. . . .
Initially, my symptoms consisted of a mild tingling in my legs. It caused me to be fidgety and made it hard to fall asleep. Eventually, I went through a number of days without much sleep and reached a point where I simply could not function. I went to a doctor who prescribed a small course of sleeping medication (a benzodiazepine). I was able to get good sleep and my sleep cycle seemed to get back on track. Over the next decade I had periodic bouts of tingling in my legs which caused me to be fidgety and interfered with sleep. As time passed, the bouts occurred with increasing frequency and the symptoms became more noticeable and uncomfortable. I would simply suffer through these bouts, sleeping poorly and paying the consequences. . . .
Being a student, I did not have a regular doctor. Unfortunately, most physicians I met did not know about restless legs syndrome, or RLS, and thought I was “drug seeking” or merely stressed out. I received a variety of patronizing responses and found these experiences insulting and demeaning. . . .
When I took my current position, I started seeing a doctor on a regular basis, and experimented with better medications. By this time, my sleep was being seriously affected by RLS. The sensations in my legs were something like a combination of an ache in my muscles (much like one gets after exercising) and an electrical, tingling sensation. They would be briefly relieved with movement, such as stretching, rubbing, contracting my muscles, or changing position, but would return within seconds. In fact, my wife says my cycle is about 13 to 15 seconds between movements. I do this either when awake or during sleep. Trying not to move greatly increases the discomfort—
I am very up front about the fact that I have RLS. In fact, whenever I teach the topic of sleep and sleep disorders in my brain and behavior classes, I always make some time to talk about my experiences with RLS. Occasionally, students approach me with their own difficulties, and I try to provide them with information and resources. (Stuart Hall, Ph.D., University of Montana)
People with the sleep disorder restless legs syndrome (RLS) experience unpleasant sensations in the legs—
Many people who display RLS have a related sleep disorder, periodic limb movement in sleep (PLMS), characterized by involuntary jerking or bending leg movements that typically occur every 10 to 60 seconds during sleep. Some people make hundreds of such movements per night; they disturb their sleep, can wake themselves, and assuredly annoy bed partners.
RLS may affect as much as 10 percent of the population, more commonly women than men. In mild cases massage, exercise, stretching, and hot baths may be helpful. For more severe cases, patients can restrict their intake of caffeine and take benzodiazepines to help them get to sleep.
RLS is difficult to treat (Wijemanne & Jankovic, 2015). L-Dopa, a drug used to treat Parkinson disease, is a frequent treatment, but no evidence confirms that RLS occurs more frequently in Parkinson patients, whose condition is related to low dopamine function. RLS has been associated with poor iron uptake, especially in the substantia nigra, and some people have been helped by iron supplements. One focus of research into RLS is to improve iron absorption by the brain.
REM sleep is no less eventful than NREM sleep. During REM sleep our eyes move; our toes, fingers, and mouths twitch; and males have penile erections. Still, we are paralyzed, as indicated by atonia. This absence of muscle tone stems from motor neuron inhibition by sleep regions of our brainstem. In the sleep lab atonia is recorded on an electromyogram as the absence of muscle activity (see Figure 13-11B).
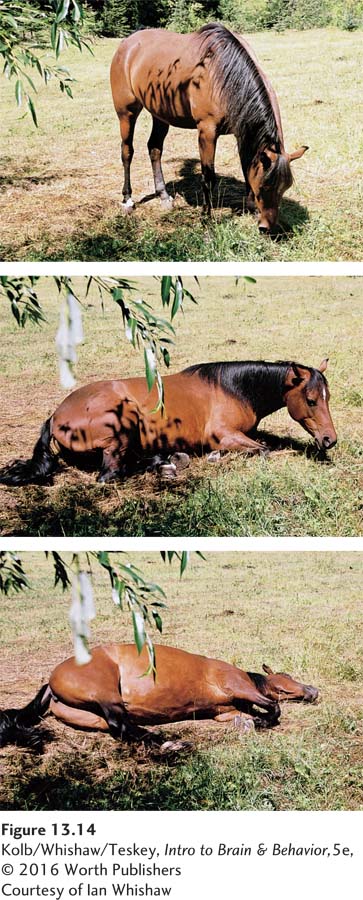
Posture is not completely lost during NREM sleep. You can get an idea of NREM sleep posture by observing a cat or dog sleeping. During NREM they may be lying down but still have some posture, with the head partly supported in a partially upright position. At the onset of REM sleep the animal usually subsides into a sprawled position as muscle paralysis sets in. Figure 13-14 illustrates the sleep postures of a horse. Horses can sleep while standing up by locking their knee joints, and they can sleep while lying down with their head held slightly up. At these times they are in NREM sleep. When they are completely sprawled out, they are in REM sleep.
461
During REM sleep mammals’ limbs twitch visibly, and if you look carefully at the face of a dog or cat, you will also see the skin of the snout twitch and the eyes move behind the eyelids. It might seem strange that an animal that is paralyzed can make small twitching movements, but the neural pathways that mediate these twitches obviously are spared the paralysis.
One explanation for the twitching of eyes, face, and distal parts of the limbs is that such movements help to maintain blood flow in those parts of the body. Another explanation is that the brain is developing coordinated movements and tuning the neural circuits that support those movements—
An additional change resulting from atonia during REM sleep is that mechanisms that regulate body temperature stop working and body temperature moves toward room temperature. You may wake up from REM sleep feeling cold or hot (or because you are cold or hot), depending on the temperature of the room, because your body has drifted toward room temperature during a REM period.
Dreaming
The most remarkable aspect of REM sleep—
How often do we dream? Reports by people on their dreaming behavior once suggested that dreaming was quite variable: some reported that they dreamed frequently and others that they never dreamed. Waking participants up during REM periods showed that everyone dreams, that they dream several times each night, and that dreams last longer as a sleep session progresses. Those who claimed not to dream presumably forgot their dreams. Perhaps people forget their dreams because they do not wake up during a dream or immediately afterward, which allows subsequent NREM sleep activity to erase the memory of the dream. Perhaps, too, the neural systems that store our daily memories are inactive during NREM sleep.
How long do dreams last? Common wisdom once suggested that dreams last but an instant. By waking people up at different intervals after the onset of REM sleep and matching the reported dream content to the previous duration of REM sleep, however, researchers demonstrated that dreams appear to take place in real time. An action that a person performs in a dream lasts about as long as it would take to perform while awake. It is likely that time shrinking is a product of remembering a dream, just as time shrinking is a feature of our recall of other memories.
What We Dream About
Studying dreaming in a sleep laboratory allows researchers to study other questions that have always intrigued people: Why do we dream? What do we dream about? What do dreams mean?
462
Figure 16-1 presents a contemporary take on Freud’s model of the mind.
Past explanations of dreaming have ranged from messages from the gods to indigestion. The first modern treatment of dreams was described by the founder of psychoanalysis, Sigmund Freud, in The Interpretation of Dreams, published in 1900. Freud reviewed the early literature on dreams, described a methodology for studying them, and provided a theory to explain their meaning. We briefly consider Freud’s theory because it remains popular in psychoanalysis and in the arts and is representative of other psychoanalytical theories of dreams.
Freud suggested that the function of dreams is the symbolic fulfillment of unconscious wishes. His theory of personality is that people have both a conscious and an unconscious. Freud proposed that the unconscious contains unacknowledged desires and wishes that are sexual. He further proposed that dreams have two levels of meaning. The manifest content of a dream is a series of often-
Freud provided a method for interpreting manifest symbols and reconstructing the latent content of dreams. For example, he pointed out that a dream usually begins with an incident from the previous day, incorporates childhood experiences, and includes ongoing unfulfilled wishes. He also identified several types of dreams, such as those that deal with childhood events, anxiety, and wish fulfillment. The latent content of the dream was important to Freud and other psychoanalysts in clinical practice because interpretation of dreams was proposed to offer insight into a patient’s problems.
Other psychoanalysts, unhappy with Freud’s emphasis on sex, developed their own methods of interpretation. The psychoanalyst Carl Jung, a contemporary of Freud, proposed that dream symbolism signifies distant human memories encoded in the brain but long since lost to conscious awareness. Jung proposed that dreams allow the dreamer to relive the history of the human race—
The dream research of Freud and his contemporaries was also impeded by their reliance on a subject’s memory of a dream and by the fact that many subjects were patients. This situation unquestionably resulted in the selection of the unusual by both the patient and the analyst. Now researchers study dreams more objectively by waking participants and questioning them.
Experimental analysis indicates that most dreams are related to events that happened quite recently and concern ongoing problems. Colors of objects, symbols, and emotional content most often relate to events taking place in a person’s recent waking period. Calvin Hall and his colleagues (1982) documented more than 10,000 dreams of healthy people and found that more than 64 percent are associated with sadness, anxiety, or anger. Only about 18 percent are happy. Hostile acts against the dreamer outnumber friendly acts by more than two to one. Surprisingly, in regard to Freud’s theory, only about 1 percent of dreams include sexual feelings or acts.
Contemporary researchers continue to attempt to interpret dream content. The two approaches that follow are polar: one sees no meaning in dreams, and the other sees the content of dreams as reflecting biologically adaptive coping mechanisms. The first approach is bottom-
Dreams as Meaningless Brain Activity
In his bottom-
463
Chapter 14 describes the extent of frontal cortex involvement in memory. Attention is the topic of Section 15-2.
Furthermore, Hobson proposes, on the basis of PET imaging, that part of the frontal cortex is less active in dreaming than in waking. The frontal cortex controls working memory for recent events and attention. The dreamer thus cannot remember and link dream events as they take place, because monitoring by the frontal cortex is required for these functions. On waking, the dreamer may attempt to come up with a story line for these fragmented meaningless images.
In Hobson’s hypothesis dreams are personal in that memories and experiences are activated but have no meaning. So the following dream, for example, with its bizarre delusional and fragmented elements, represents images synthesized to accompany brain activation. Any apparent meaning is invented after the fact, in this case by the middle-
I found myself walking in a jungle. Everything was green and fresh and I felt refreshed and content. After some time I encountered a girl whom I did not know. The most remarkable thing about her was her eyes, which had an almost gold color. I was really struck by her eyes not only because of their unique color but also because of their expression. I tried to make out other details of her face and body but her eyes were so dominating that was all I could see. Eventually, however, I noticed that she was dressed in a white robe and was standing very still with her hands at her side. I then noticed that she was in a compound with wire around it. I became concerned that she was a prisoner. Soon, I noticed other people dressed in white robes and they were also standing still or walking slowly without swinging their arms. It was really apparent that they were all prisoners. At this time I was standing by the fence that enclosed them, and I was starting to feel more concerned. Suddenly it dawned on me that I was in the compound and when I looked down at myself I found that I was dressed in a white robe as well. I remember that I suddenly became quite frightened and woke up when I realized that I was exactly like everyone else. The reason that I remembered this dream is the very striking way in which my emotions seemed to be going from contentment, to concern, to fear as the dream progressed. I think that this dream reflected my desire in the 1970s to maintain my individuality. (Recounted by A. W.)
Dreams as a Coping Strategy
Anttio Revonsuo of Finland uses content analysis to argue that dreams are biologically adaptive in that they lead to enhanced coping strategies for threatening life events (Valli & Revonsuo, 2009). The evolutionary aspect of this top-
Dream threats are the same events that are threatening in waking life (Figure 13-15). For example, animals and strange men who could be characterized as enemies figure prominently in dreams. Dream content incorporates the current emotional problems of the dreamer and leads to improvements in and adjustments to life problems.
Erich Lessing/Art Resource
464
In contrast with the threat interpretation of dreams and from their own analysis of dream content, Malcolm-
An extension of the top-
Part of the challenge in studying dreams is that they occur throughout our sleep–
Much about dreams is not understood. Very young children spend a lot of time in REM sleep yet do not report complex dreams filled with emotion and conflict. Children may experience brief frightening dreams called night terrors during NREM sleep. Night terrors can be so vivid that the child continues to experience the dream and the fear after awaking. A 4-
13-3 REVIEW
Sleep Stages and Dreaming
Before you continue, check your understanding.
Question 1
Sleep consists of two phases: ____________, which stands for ____________, and ____________, which stands for ____________.
Question 2
REM sleep is characterized by eye movement, as recorded by the ____________; atonia, recorded by the ____________; and waking activity, recorded by the ____________.
Question 3
Sleepers experience about ____________ REM sleep periods each night, with each period ____________ as sleep progresses.
Question 4
Evidence from sleep lab analysis suggests that ____________ dreams and that dreams take place in ____________.
Question 5
What major factor makes interpreting dreams difficult?
Answers appear in the Self Test section of the book.