6-4 Explaining and Treating Drug Abuse
Why do people become addicted to drugs? Early explanations centered on pleasure and dependence: habitual drug users initially feel pleasure but then endure psychological and physiological withdrawal symptoms as the drug wears off. They feel anxious, insecure, or just plain sick without the drug, so they take it again to alleviate those symptoms. In this way, they get hooked on the drug.
Although this dependency hypothesis may account for part of drug-
Wanting-
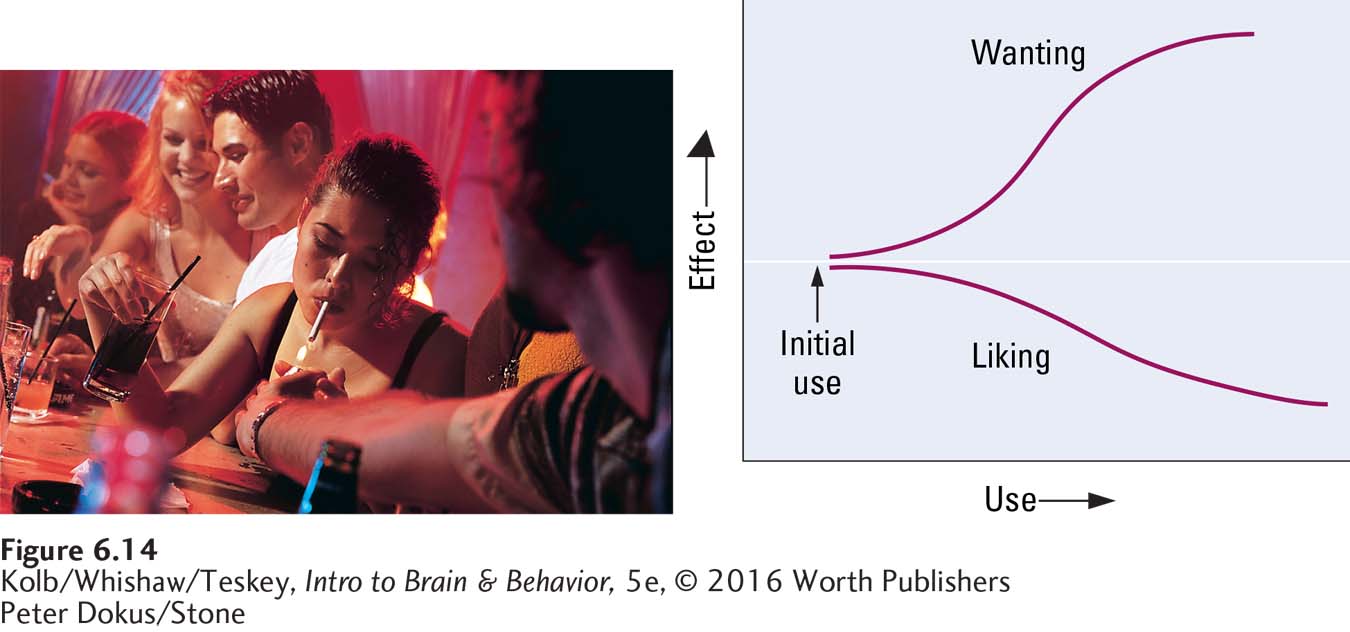
To account for all the facts about drug abuse and addiction, Terry Robinson and Kent Berridge (2008) proposed the incentive sensitization theory, also called the wanting-
195
The first step on the proposed road to drug dependence is the initial experience, when the drug affects a neural system associated with pleasure. At this stage, the user may like the substance—
In classical (Pavlovian) conditioning, learning to associate a formerly neutral stimulus (the sound of a bell) with a stimulus (food) elicits an involuntary response (salivation).
With each use, the drug taker increasingly associates the cues related to drug use—
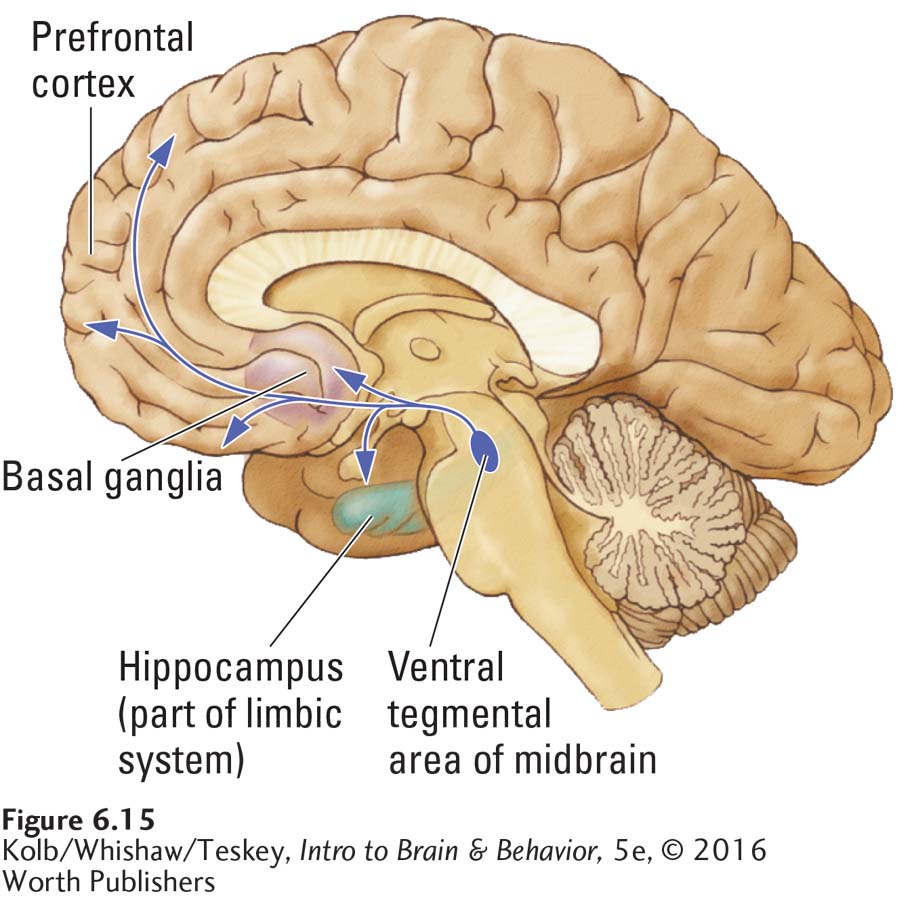
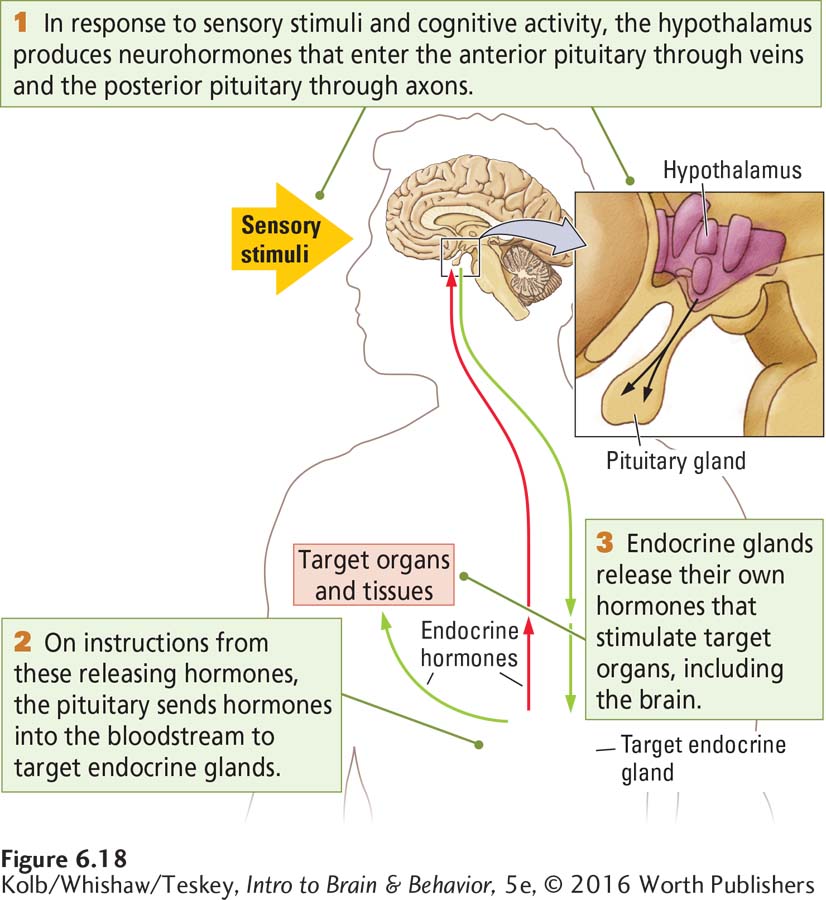
The neural basis of addiction is proposed to involve multiple brain systems. The decision to take a drug is made in the prefrontal cortex, an area that participates in most daily decisions. When a drug is taken, it activates opioid systems in the brainstem that are generally related to pleasurable experiences. And wanting drugs may spring from activity in the mesolimbic pathways of the dopaminergic activating system.
In these mesolimbic pathways, diagrammed in Figure 6-15, the axons of dopamine neurons in the midbrain project to structures in the basal ganglia, to the frontal cortex, and to the limbic system. When drug takers encounter cues associated with drug taking, the mesolimbic system becomes active, releasing dopamine. Dopamine release is the neural correlate of wanting.
When a rat is placed in an environment where it anticipates a favored food or sex, investigators record dopamine increases in the striatum (see Section 7-5).
Another brain system may be responsible for conditioning drug-
Multiple findings align with the wanting-
Notwithstanding support for a dopamine basis for addiction, recent research suggests more than one type of addiction. Some rats become readily conditioned to cues associated with reinforcement, for example a bar that delivers a reward when pressed. Other animals ignore the bar’s incentive salience but are attracted to the location where they receive reinforcement. Animals that display the former behavior are termed sign trackers and the other group, goal trackers. Sign trackers exposed to addictive drugs appear to attribute incentive salience to drug-
196
We can extend wanting-
Why Doesn’t Everyone Abuse Drugs?
Observing that some people are more prone than others to drug abuse and dependence, scientists have investigated and found three lines of evidence suggesting a genetic contribution to differences in drug use. First, if one identical twin (same genotype) abuses alcohol, the other twin is more likely to abuse it than if the twins are fraternal (have only some genes in common). Second, people adopted shortly after birth are more likely to abuse alcohol if their biological parents were alcoholic, even though they have had almost no contact with those parents. Third, although most animals do not care for alcohol, selective breeding of mice, rats, and monkeys can produce strains that consume large quantities of it.
Each line of evidence presents problems, however. Perhaps identical twins show greater concordance rates (incidence of similar behavioral traits) for alcohol abuse because their environments are more similar than those of fraternal twins. And perhaps the link between alcoholism in adoptees and their biological parents has to do with nervous system changes due to prenatal exposure to the drug. Finally, the fact that animals can be selectively bred for alcohol consumption does not mean that all human alcoholics have a similar genetic makeup. The evidence for a genetic basis of alcohol abuse will become compelling only when a gene or set of genes related to alcoholism is found.
Less-
Epigenetics offers another explanation of susceptibility to addiction (Hillemacher et al., 2015). Addictive drugs may reduce the transcriptional ability of genes related to voluntary control and increase the transcriptional ability of other genes related to behaviors susceptible to addiction. Epigenetic changes in an individual’s gene expression may be relatively permanent and can be passed along, perhaps through the next few generations. For these reasons, epigenetics can account both for the enduring behaviors that support addiction and for the tendency of drug addiction to be inherited.
Treating Drug Abuse
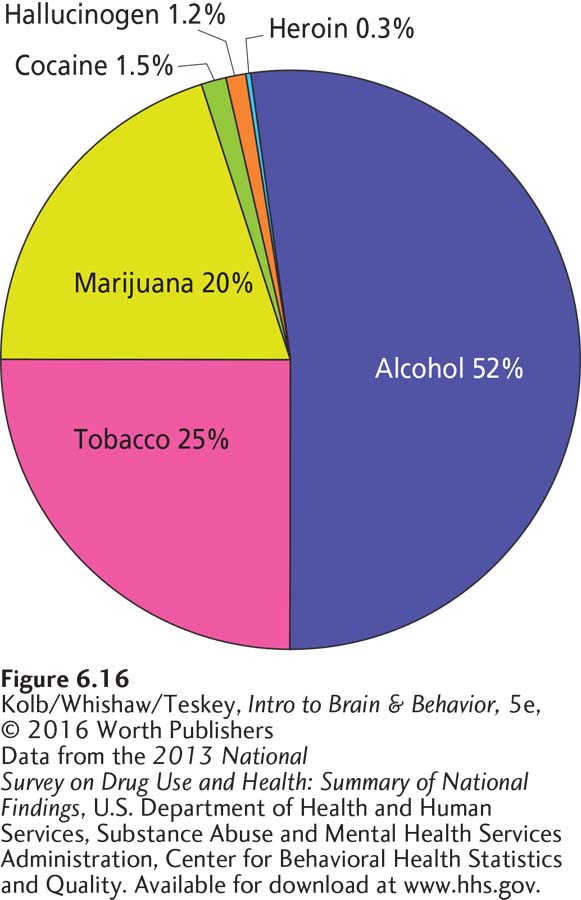
Figure 6-16 charts the relative incidence of drug use in the United States—
Treating drug abuse is difficult in part because legal proscriptions are irrational. In the United States, the Harrison Narcotics Act of 1914 made heroin and a variety of other drugs illegal and made the treatment of addicted people by physicians in their private offices illegal. The Drug Addiction Treatment Act of 2000 partly reversed this prohibition, allowing the treatment of patients but with a number of restrictions. In addition, legal consequences attending drug use vary greatly with the drug and the jurisdiction.
197
From a health standpoint, tobacco has much higher proven health risks than does marijuana. Moderate use of alcohol is likely benign. Moderate use of opioids is likely impossible. Social coercion is useful in reducing tobacco use: witness the marked decline in smoking as a result of prohibitions against smoking in public places. Medical intervention is necessary to provide methadone and other drug treatment of opioid abusers.
The numerous approaches to treating drug abuse vary, depending on the drug. Many online sites support self-
Neuroscience research will continue to lead to a better understanding of the neural basis of drug use and to better treatment. The best approach to any drug treatment likely recognizes that addiction is a lifelong problem for most people. Thus, drug addiction must be treated in the same way as chronic behavioral addictions and medical problems—
Can Drugs Cause Brain Damage?
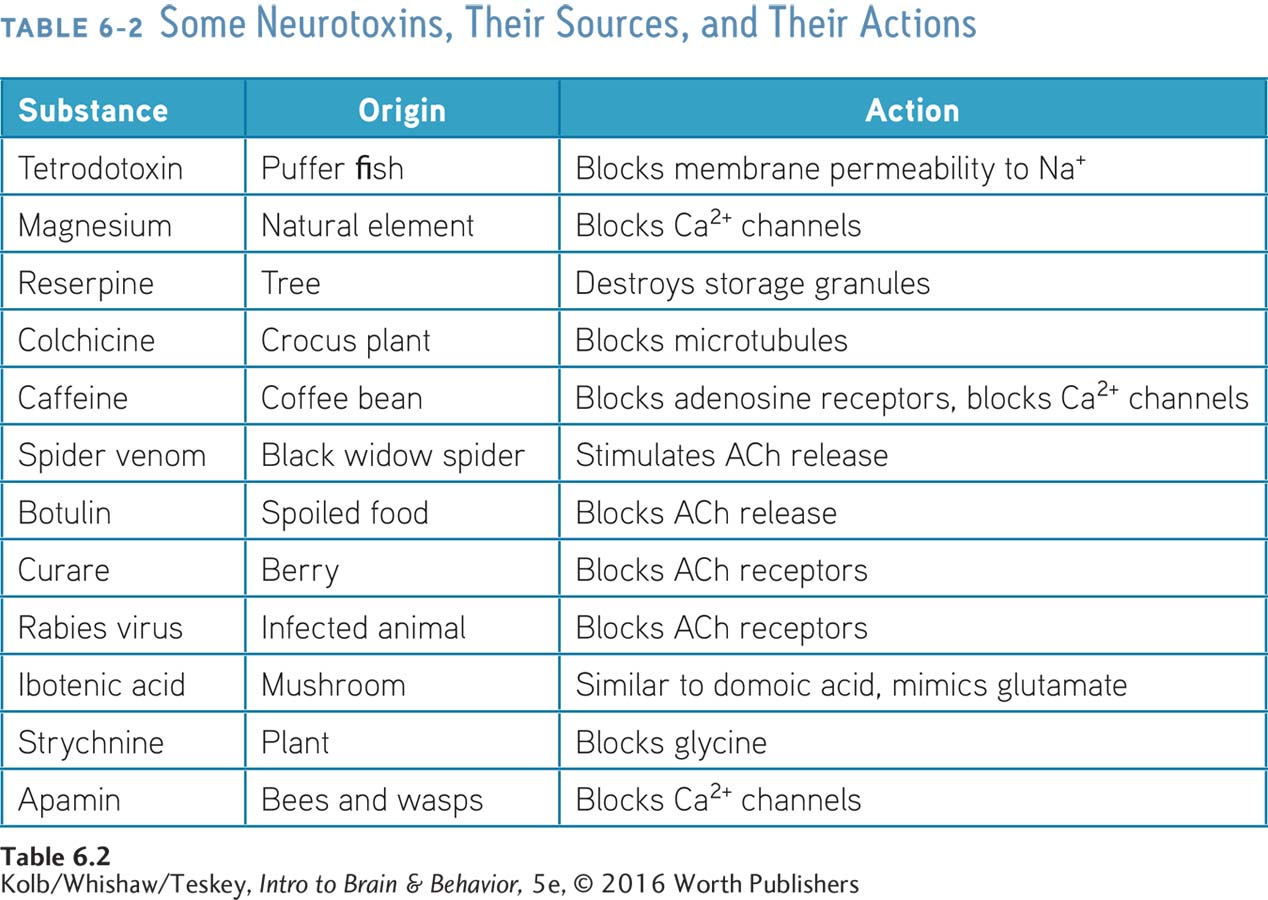
Many natural substances can act as neurotoxins; Table 6-2 lists some of them. Ongoing investigations of the neurotoxicity of these substances and other drugs in animal models show that many cause brain damage. Whether drugs of abuse cause brain damage in humans—
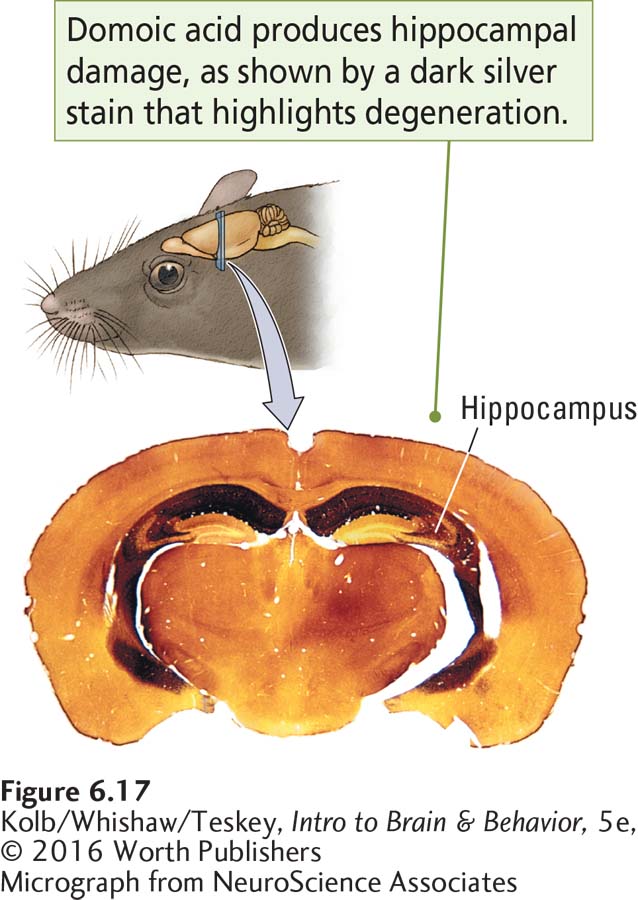
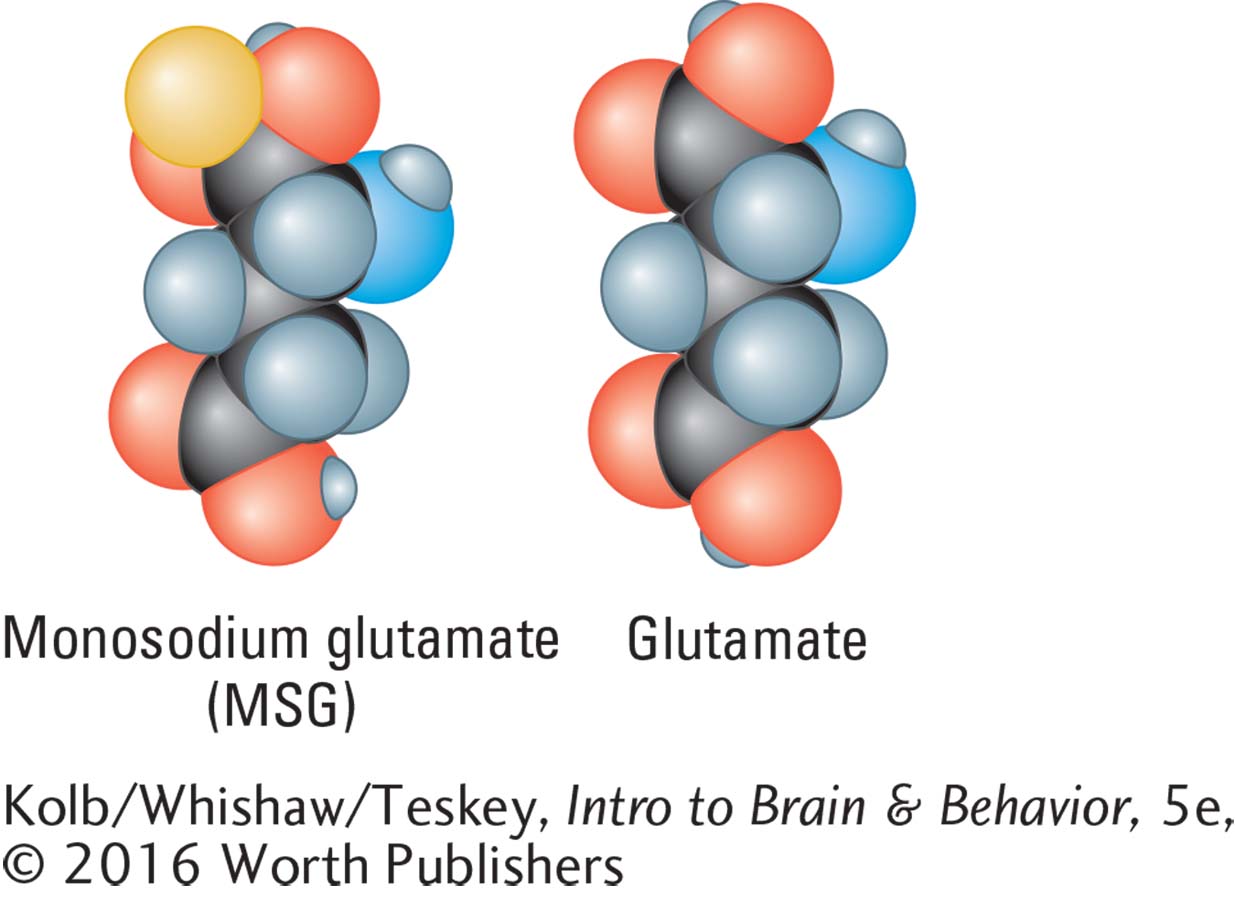
In the late 1960s, many reports linked monosodium glutamate, MSG, a salty-
This line of research led to the discovery that many glutamatelike substances, including domoic acid and kainic acid, both toxins in seaweed, and ibotenic acid, which is found in some poisonous mushrooms, similarly kill neurons (Figure 6-17). Some drugs, such as PCP and ketamine, also act as glutamate agonists, leaving open the possibility that at high doses they too can cause neuronal death.
198
Glutamatelike drugs are toxic because they act on glutamate receptors. Glutamate receptor activation results in an influx of Ca2+ into the cell, which through second messengers activates a suicide gene leading to apoptosis (cell death). This discovery shows that a drug might be toxic not only because of its general effect on cell function but also as an agent that activates normal cell processes related to apoptosis.
We must add that there is no evidence that moderate consumption of MSG is harmful.
What about the many recreational drugs that affect the nervous system? Are any neurotoxic? Sorting out the effects of the drug itself from the effects of other factors related to taking the drug is a major problem. Chronic alcohol use, for instance, can be associated with damage to the thalamus and limbic system, producing severe memory disorders. Alcohol, however, does not directly cause this damage. Alcoholics typically obtain low amounts of thiamine (vitamin B1) in their diet, and alcohol interferes with the intestine’s absorption of thiamine. Thiamine plays a vital role in maintaining cell membrane structure.
Focus 5-4 reports the chilling case of heroin addicts who developed Parkinson disease after using synthetic heroin, owing to a contaminant (MPTP) in the drug.
Similarly, among the many reports of people who have a severe psychiatric disorder subsequent to abusing certain recreational drugs, in most cases determining whether the drug initiated the condition or aggravated an existing problem is difficult. Exactly determining whether the drug itself or some contaminant in it caused a harmful outcome also is difficult. With the increasing sensitivity of brain imaging studies, however, evidence is increasing that many drugs used recreationally can cause brain damage and cognitive impairments.
The strongest evidence comes from the study of the synthetic amphetaminelike drug MDMA, also called Ecstasy, and in pure powdered form, Molly (Büttner, 2011). Although MDMA is structurally related to amphetamine, it produces hallucinogenic effects and is called a hallucinogenic amphetamine. Findings from animal studies show that doses of MDMA approximating those taken by human users result in the degeneration of very fine serotonergic nerve terminals. In monkeys, significant terminal loss may be permanent, as shown in Figure 6-18.
Memory impairments and damage in MDMA users revealed by brain imaging may be a result of similar neuronal damage (Cowan et al., 2008). MDMA may also contain a contaminant, paramethoxymethamphetamine (PMMA). This notoriously toxic amphetamine is often called Dr. Death because the difference between a dose that causes behavioral effects and a dose that causes death is minuscule (Vevelstad et al., 2012). Contamination by unknown compounds can occur in any drug purchased on the street.
The psychoactive properties of cocaine are similar to those of amphetamine, and so cocaine also is suspect with respect to brain damage. Cocaine use is related to the blockage of cerebral blood flow and other changes in blood circulation. Brain imaging studies suggest that cocaine use can be toxic to neurons, because several brain regions are reduced in size in cocaine users (Liu et al., 2011).
Focus 7-3 explores the hypothesis that genetic vulnerability predisposes some adolescents to develop a psychosis when exposed to cannabis.
Chronic marijuana use has been associated with psychotic attacks. Clinical Focus 6-4, Drug-Induced Psychosis, describes one. The marijuana plant contains at least 400 chemicals, 60 or more of which are structurally related to its active ingredient, tetrahydrocannabinol. Determining whether a psychotic attack is related to THC or to some other chemical in marijuana is almost impossible.
Whether or not THC can cause psychosis, there is no evidence that the disease is a result of brain damage. Indeed, beyond the therapeutic applications of TCH cited in Section 6-2, recent studies suggest that THC may have neuroprotective properties. It can aid brain healing after traumatic brain injury and slow the progression of diseases associated with brain degeneration, including Alzheimer disease and Huntington disease (Nguyen et al., 2014).
199
CLINICAL FOCUS 6-4
Drug-
At age 29, R. B. S. smoked marijuana chronically. For years, he had been selectively breeding a potent strain of marijuana in anticipation of the day when it would be legalized. R. B. S. made his living as a pilot, flying small freight aircraft into coastal communities in the Pacific Northwest.
One evening, R. B. S. had a sudden revelation: he was no longer in control of his life. Convinced that a small computer had been implanted in his brain when he was 7 years old and was manipulating his behavior, he confided in a close friend, who urged him to consult a doctor. R. B. S. insisted that he had undergone the surgery when he participated in an experiment at a local university. He also claimed that all the other children who participated in the experiment had been murdered.
The doctor told R. B. S. that the computer implantation was unlikely but called the psychology department at the university and got confirmation that children had in fact taken part in an experiment conducted years before. The records of the study had long since been destroyed. R. B. S. believed that this information completely vindicated his story. His delusional behavior persisted and eventually cost him his pilot’s license.
R. B. S. seemed to compartmentalize the delusion. When asked why he could no longer fly, he intently recounted the story of the implant and the murders, asserting that its truth had cost him the medical certification needed for a license. Then he happily and appropriately discussed other topics.
R. B. S. had a mild focal psychosis: he was losing contact with reality. In some cases, this break is so severe and the capacity to respond to the environment so impaired and distorted that the person can no longer function. People in a state of psychosis may hallucinate, may have delusions, or may withdraw into a private world isolated from people and events around them.
A variety of drugs can produce psychosis, including LSD, amphetamine, cocaine, and, as shown by this case, marijuana. At low doses THC, the active ingredient in marijuana, has mild sedative-
Marijuana comes from the leaves of the hemp plant, Cannabis sativa. Humans have used hemp for thousands of years to make rope, paper, cloth, and a host of other products. And marijuana has a number of beneficial medical effects. In the Pacific Northwest, marijuana is the largest agricultural crop and makes a larger contribution to the economy than does forestry. In some states marijuana can legally be purchased for personal use, and in many states its medical use is legal. Under federal law, however, it remains illegal everywhere in the United States.
R. B. S.’s heavy marijuana use certainly raises the suspicion that the drug had some influence on his delusional condition (Wilkinson et al., 2014). Cannabis use has been reported to moderately increase the risk of psychotic symptoms in young people and has a much stronger effect in those with a predisposition for psychosis, especially if potent strains are used (Di Forti et al., 2015). Although there is evidence that heavy marijuana use may be associated with alterations in brain development, it is unclear whether brain abnormalities are a result of marijuana use or a causal factor in its use (Lubman et al., 2015).

6-4 REVIEW
Explaining and Treating Drug Abuse
Before you continue, check your understanding.
Question 1
The wanting-
Question 2
At the neural level, the decision to take a drug is made in the brain’s _______. Once taken, the drug activates opioid systems related to pleasurable experiences in the _______. Drug cravings may originate in the _______, and the repeated pairing of drug-
200
Question 3
As an alternative to explanations of susceptibility to addiction based on genetic _______,_______ can account both for the enduring behaviors that support addiction and for the tendency of drug addiction to be inherited.
Question 4
It is hard to determine whether recreational drugs cause brain damage in humans because it is difficult to distinguish the effects of _______ from the effects of _______.
Question 5
Briefly describe the basis for a reasonable approach to treating drug addiction.
Answers appear in the Self Test section of the book.