After a meal, when blood glucose rises above its normal level of 5 mM, the pancreatic β cells respond to the rise in glucose (and the concurrent rise in amino acids) by releasing insulin into the blood (Figure 16-39). We saw in Chapter 14 that these cells store insulin in a dehydrated, almost crystalline form in secretory vesicles; as with all regulated secretory pathways, secretion is triggered by a rise in cytosolic Ca2+. Insulin secretion is triggered by a rise in extracellular glucose, which causes a proportionate increase in the rate of glucose entry into the cells and a corresponding increase in the rate of glycolysis. The resulting rise in the concentration of cytosolic ATP causes closing of an ion channel unique to the β cells—an ATP-gated K+ channel—reducing the efflux of K+ ions from the cell. The resulting depolarization of the plasma membrane triggers the opening of voltage-sensitive Ca2+ channels, an increase in cytosolic Ca2+, and insulin secretion.
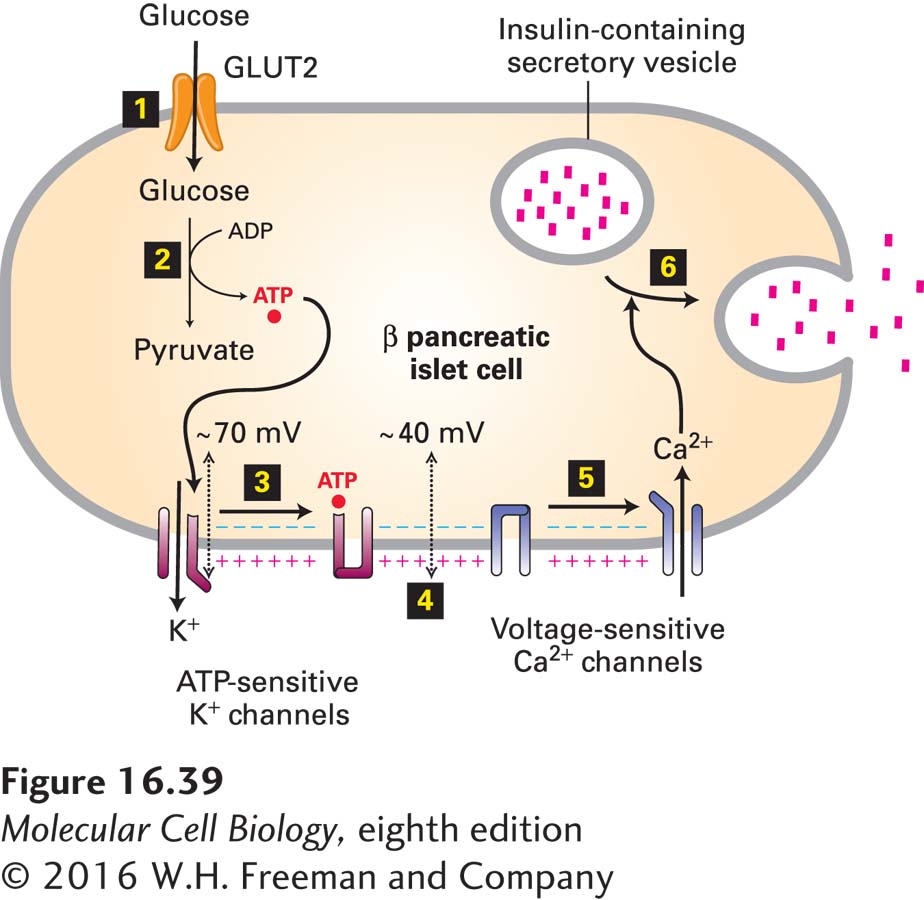
FIGURE 16-39 Secretion of insulin in response to a rise in blood glucose. The entry of glucose into pancreatic β cells is mediated by the GLUT2 glucose transporter (step 1). Because the Km for glucose of GLUT2 is 20 mM, a rise in extracellular glucose from 5 mM, characteristic of the fasting state, causes a proportional increase in the rate of glucose entry (see Figure 11-4). The conversion of glucose into pyruvate is thus accelerated, resulting in an increase in the concentration of ATP in the cytosol (step 2). The binding of ATP to ATP-sensitive K+ channels in the β cells closes those channels (step 3), thus reducing the efflux of K+ ions from the cell. The resulting small depolarization of the plasma membrane (step 4) triggers the opening of voltage-sensitive Ca2+ channels (step 5). The influx of Ca2+ ions raises the cytosolic Ca2+ concentration, triggering the fusion of insulin-containing secretory vesicles with the plasma membrane and the secretion of insulin (step 6). See J. Q. Henquin, 2000, Diabetes 49:1751.