56.1 Drug Therapies
Drug or placebo effect? For many people, depression lifts while taking an antidepressant drug. But people given a placebo may experience the same effect. Double-blind clinical trials suggest that, especially for those with severe depression, antidepressant drugs do have at least a modest clinical effect.
56-1 What are the drug therapies? How do double-blind studies help researchers evaluate a drug’s effectiveness?
Since the 1950s, discoveries in psychopharmacology (the study of drug effects on mind and behavior) have revolutionized the treatment of people with severe disorders, liberating hundreds of thousands from hospital confinement. Thanks to drug therapy, along with efforts to replace hospitalization with community mental health programs, today’s resident population of mental hospitals is a small fraction of what it was a half-century ago. For some who are unable to care for themselves, however, release from hospitals has meant homelessness, not liberation.
Almost any new treatment, including drug therapy, is greeted by an initial wave of enthusiasm as many people apparently improve. But that enthusiasm often diminishes after researchers subtract the rates of (1) normal recovery among untreated persons and (2) recovery due to the placebo effect, which arises from the positive expectations of patients and mental health workers alike. Even mere exposure to advertising about a drug’s supposed effectiveness can increase its effect (Kamenica et al., 2013). So, to evaluate the effectiveness of any new drug, researchers give half the patients the drug, and the other half a similar-appearing placebo. Because neither the staff nor the patients know who gets which, this is called a double-blind procedure. The good news: In double-blind studies, some drugs have proven useful.
Antipsychotic Drugs
The revolution in drug therapy for psychological disorders began with the accidental discovery that certain drugs, used for other medical purposes, calmed patients with psychoses (disorders in which hallucinations or delusions indicate some loss of contact with reality). These first-generation antipsychotic drugs, such as chlorpromazine (sold as Thorazine), dampened responsiveness to irrelevant stimuli. Thus, they provided the most help to patients experiencing positive symptoms of schizophrenia, such as auditory hallucinations and paranoia (Lehman et al., 1998; Lenzenweger et al., 1989).
Perhaps you can guess an occasional side effect of L-dopa, a drug that raises dopamine levels for Parkinson’s patients: hallucinations.
The molecules of most conventional antipsychotic drugs are similar enough to molecules of the neurotransmitter dopamine to occupy its receptor sites and block its activity. This finding reinforces the idea that an overactive dopamine system contributes to schizophrenia.
Antipsychotics also have powerful side effects. Some produce sluggishness, tremors, and twitches similar to those of Parkinson’s disease (Kaplan & Saddock, 1989). Long-term use of antipsychotics can produce tardive dyskinesia, with involuntary movements of the facial muscles (such as grimacing), tongue, and limbs. Although not more effective in controlling schizophrenia symptoms, many of the newer-generation antipsychotics, such as risperidone (Risperdal) and olanzapine (Zyprexa), have fewer of these effects. These drugs may, however, increase the risk of obesity and diabetes (Buchanan et al., 2010; Tiihonen et al., 2009).
Antipsychotics, combined with life-skills programs and family support, have given new hope to many people with schizophrenia (Guo, 2010). Hundreds of thousands of patients have left the wards of mental hospitals and returned to work and to near-normal lives (Leucht et al., 2003).
Antianxiety Drugs
Like alcohol, antianxiety drugs, such as Xanax or Ativan, depress central nervous system activity (and so should not be used in combination with alcohol). Antianxiety drugs are often successfully used in combination with psychological therapy. One antianxiety drug, the antibiotic D-cycloserine, facilitates the extinction of learned fears in combination with behavioral treatments. Experiments indicate that the drug enhances the benefits of exposure therapy and helps relieve the symptoms of posttraumatic stress disorder and obsessive-compulsive disorder (Davis, 2005; Kushner et al., 2007).
A criticism sometimes made of the behavior therapies—that they reduce symptoms without resolving underlying problems—is also made of drug therapies. Unlike the behavior therapies, however, these substances may be used as an ongoing treatment. “Popping a Xanax” at the first sign of tension can create a learned response; the immediate relief reinforces a person’s tendency to take drugs when anxious. Antianxiety drugs can also be addictive. After heavy use, people who stop taking them may experience increased anxiety, insomnia, and other withdrawal symptoms.
Over the dozen years at the end of the twentieth century, the rate of outpatient treatment for anxiety disorders, obsessive-compulsive disorder, and posttraumatic stress disorder nearly doubled. The proportion of psychiatric patients receiving medication during that time increased from 52 to 70 percent (Olfson et al., 2004). And the new standard drug treatment for anxiety disorders? Antidepressants.
Antidepressant Drugs
The antidepressants were named for their ability to lift people up from a state of depression, and this was their main use until recently. The label is a bit of a misnomer now that these drugs are increasingly being used to successfully treat anxiety disorders, obsessive-compulsive disorder, and posttraumatic stress disorder (Wetherell et al., 2013). Many of these drugs work by increasing the availability of neurotransmitters, such as norepinephrine or serotonin, which elevate arousal and mood and appear scarce when a person experiences feelings of depression or anxiety. The most commonly prescribed drugs in this group, including Prozac and its cousins Zoloft and Paxil, work by blocking the reabsorption and removal of serotonin from synapses (FIGURE 56.1). Given their use in treating disorders other than depression—from anxiety to strokes—these drugs are most often called SSRIs—selective serotonin reuptake inhibitors (rather than antidepressants) (Kramer, 2011). Some of the older antidepressant drugs work by blocking the reabsorption or breakdown of both norepinephrine and serotonin. Though effective, these dual-action drugs have more potential side effects, such as dry mouth, weight gain, hypertension, or dizzy spells (Anderson, 2000; Mulrow, 1999). Administering them by means of a patch, which bypasses the intestines and liver, helps reduce such side effects (Bodkin & Amsterdam, 2002).
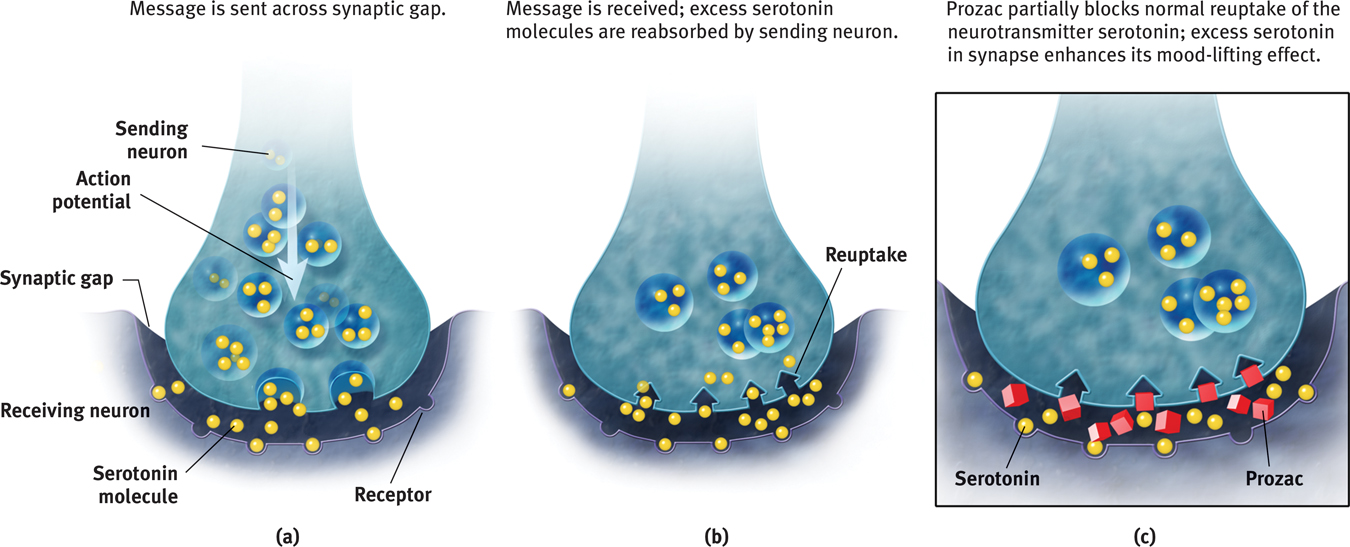
 Figure 56.1
Figure 56.1
Biology of antidepressants Shown here is the action of Prozac, which partially blocks the reuptake of serotonin.
Be advised: Patients with depression who begin taking antidepressants do not wake up the next day singing, “It’s a beautiful day!” Although the drugs begin to influence neurotransmission within hours, their full psychological effect often requires four weeks (and may involve a side effect of diminished sexual desire). One possible reason for the delay is that increased serotonin promotes new synapses plus neurogenesis—the birth of new brain cells—perhaps reversing stress-induced loss of neurons (Launay et al., 2011). Researchers are also exploring the possibility of quicker-acting antidepressants. One, ketamine, blocks hyperactive receptors for glutamate, a neurotransmitter, and causes a burst of new synapses—but with possible side effects such as hallucinations (Grimm & Scheidegger, 2013; Naughton et al., 2014).
Antidepressant drugs are not the only way to give the body a lift. Aerobic exercise, which calms people who feel anxious and energizes those who feel depressed, does about as much good for most people with mild to moderate depression, and has additional positive side effects. Cognitive therapy, by helping people reverse their habitual negative thinking style, can boost the drug-aided relief from depression and reduce the posttreatment risk of relapse (Hollon et al., 2002; Keller et al., 2000; Vittengl et al., 2007). Better yet, some studies suggest, is to attack depression (and anxiety) from both below and above (Cuijpers et al., 2010; Walkup et al., 2008): Use antidepressant drugs (which work, bottom-up, on the emotion-forming limbic system) in conjunction with cognitive-behavioral therapy (which works, top-down, starting with changed frontal lobe activity).
“No twisted thought without a twisted molecule.”
Attributed to psychologist Ralph Gerard
Researchers generally agree that people with depression often improve after a month on antidepressants. But after allowing for natural recovery and the placebo effect, how big is the drug effect? Not big, report Irving Kirsch and his colleagues (1998, 2002, 2010, 2014). Their analyses of double-blind clinical trials indicate that placebos accounted for about 75 percent of the active drug’s effect. In a follow-up review that included unpublished clinical trials, the antidepressant drug effect was again modest (Kirsch et al., 2008). The placebo effect was less for those with severe depression, which made the added benefit of the drug somewhat greater for them. “Given these results, there seems little reason to prescribe antidepressant medication to any but the most severely depressed patients, unless alternative treatments have failed,” Kirsch concluded (BBC, 2008). A newer analysis confirms that the antidepressant benefit compared to placebos is “minimal or nonexistent, on average, in patients with mild or moderate symptoms.” For those folks, aerobic exercise or psychotherapy is often effective. But among patients with “very severe” depression, the medication advantage becomes “substantial” (Fournier et al., 2010).
 HOW WOULD YOU KNOW? To better understand how clinical researchers have explored these questions, complete LaunchPad’s How Would You Know How Well Antidepressants Work?
HOW WOULD YOU KNOW? To better understand how clinical researchers have explored these questions, complete LaunchPad’s How Would You Know How Well Antidepressants Work?
Mood-Stabilizing Medications
In addition to antipsychotic, antianxiety, and antidepressant drugs, psychiatrists have mood-stabilizing drugs in their arsenal. For those suffering the emotional highs and lows of bipolar disorder, the simple salt lithium can be an effective mood stabilizer. Australian physician John Cade discovered this in the 1940s when he administered lithium to a patient with severe mania and the patient became well in less than a week (Snyder, 1986). After suffering mood swings for years, about 7 in 10 people with bipolar disorder benefit from a long-term daily dose of this cheap salt, which helps prevent or ease manic episodes and, to a lesser extent, lifts depression (Solomon et al., 1995). Kay Redfield Jamison (1995, pp. 88–89) described the effect:
Lithium prevents my seductive but disastrous highs, diminishes my depressions, clears out the wool and webbing from my disordered thinking, slows me down, gentles me out, keeps me from ruining my career and relationships, keeps me out of a hospital, alive, and makes psychotherapy possible.
Lithium reduces bipolar patients’ risk of suicide—to about one-sixth of bipolar patients not taking lithium (Oquendo et al., 2011). Naturally occurring lithium in drinking water has also correlated with lower suicide rates (across 18 Japanese cities and towns) and lower crime rates (across 27 Texas counties) (Ohgami et al., 2009; Schrauzer & Shrestha, 1990, 2010; Terao et al., 2010). Although we do not fully understand why, lithium works. And so does Depakote, a drug originally used to treat epilepsy and more recently found effective in the control of manic episodes associated with bipolar disorder.
RETRIEVAL PRACTICE
- How do researchers evaluate the effectiveness of particular drug therapies?
Researchers assign people to treatment and no-treatment conditions to see if those who receive the drug therapy improve more than those who don’t. Double-blind controlled studies are most effective. If neither the therapist nor the client knows which participants have received the drug treatment, then any difference between the treated and untreated groups will reflect the drug treatment’s actual effect.
- The drugs given most often to treat depression are called __________ . Schizophrenia is often treated with __________ drugs .
antidepressants; antipsychotic