5.3 The Nonvisual Senses
For humans, vision is the major sense. More of our brain cortex is devoted to vision than to any other sense. Yet without hearing, touch, taste, smell, and body position and movement, our experience of the world would be vastly diminished.
Hearing
audition the sense or act of hearing.
Like our other senses, our hearing, or audition, helps us adapt and survive. Hearing provides information and enables relationships. It lets us communicate invisibly, shooting unseen air waves across space and receiving the same from others. Hearing loss is therefore an invisible disability. To not catch someone’s name, to not grasp what someone is asking, and to miss the hilarious joke is to be deprived of what others know, and sometimes to feel excluded. (As a person with hearing loss, I [DM] know the feeling.)
Most of us, however, can hear a wide range of sounds, and the ones we hear best are those in the range of the human voice. With normal hearing, we are remarkably sensitive to faint sounds, such as a child’s whimper. (If our ears were only slightly more sensitive, we would hear a constant hiss from the movement of air molecules.) We also are acutely sensitive to sound differences. Among thousands of possible voices, we easily distinguish an unseen friend’s. Moreover, hearing is fast. Your reaction to a sudden sound is at least 10 times faster than your response when you suddenly see something “from the corner of your eye, turn your head toward it, recognize it, and respond to it” (Horowitz, 2012). A fraction of a second after such events stimulate your ear’s receptors, millions of neurons are working together to extract the essential features, compare them with past experience, and identify the sound (Freeman, 1991). For hearing as for seeing, we wonder: How do we do it?
Sound Waves: From the Environment Into the Brain
153
LOQ 5-

Hit a piano key and you unleash the energy of sound waves. Moving molecules of air, each bumping into the next, create waves of compressed and expanded air, like ripples on a pond circling out from a tossed stone. Our ears detect these brief air pressure changes.
frequency the number of complete wavelengths that pass a point in a given time (for example, per second).
pitch a tone’s experienced highness or lowness; depends on frequency.
Like light waves, sound waves vary in shape. The height, or amplitude, of sound waves determines their perceived loudness. Their length, or frequency, determines the pitch (the high or low tone) we experience. Long waves have low frequency—
We measure sounds in decibels, with zero decibels representing the lowest level detectable by human ears. Normal conversation registers at about 60 decibels. A whisper falls at about 20 decibels, and a jet plane passing 500 feet overhead registers at about 110 decibels. Prolonged exposure to any sounds above 85 decibels can produce hearing loss. Tell that to football fans of the NFL’s Kansas City Chiefs who, in 2014, broke the Guinness World Record for the noisiest stadium at 142 decibels (Liberman, 2015). Hear today, gone tomorrow.
Retrieve + Remember
Question 5.13
•The amplitude of a sound wave determines our perception of ____________ (loudness/pitch).
ANSWER: loudness
Question 5.14
•The longer the sound waves, the ____________ (lower/higher) their frequency and the ___________ (lower/higher) their pitch.
ANSWERS: lower; lower
Decoding Sound Waves
LOQ 5-
How does vibrating air morph into nerve impulses that your brain can decode as sounds?
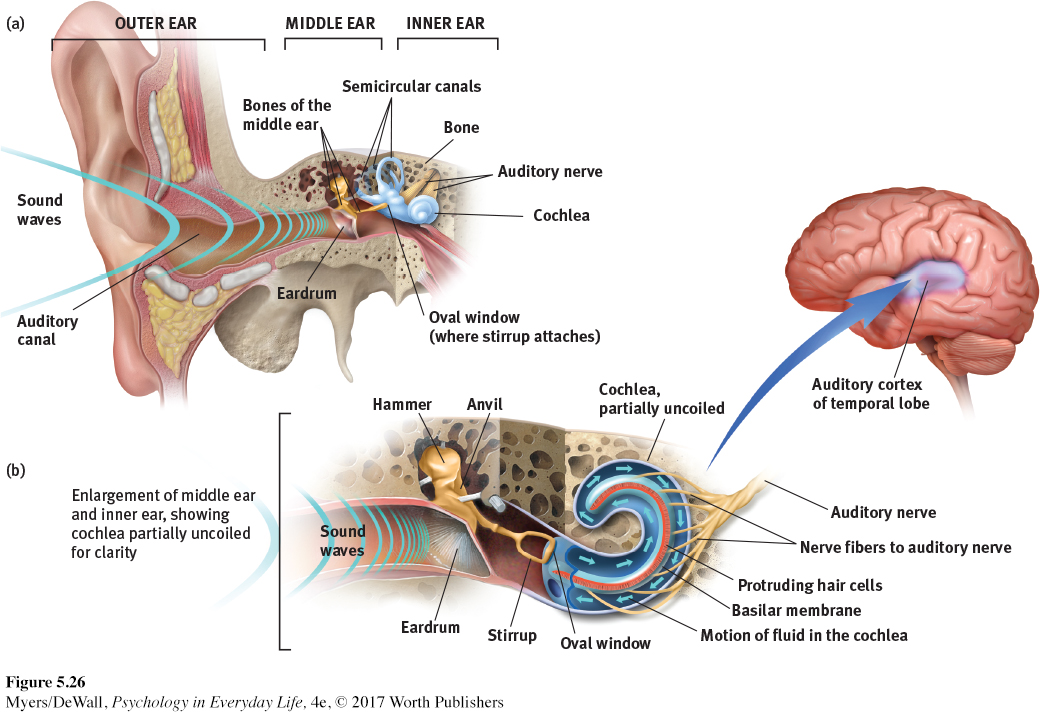
The process begins when sound waves entering your outer ear trigger a mechanical chain reaction. Your outer ear channels the waves into your auditory canal, where they bump against your eardrum, causing this tight membrane to vibrate (FIGURE 5.26a).
middle ear the chamber between the eardrum and cochlea containing three tiny bones (hammer, anvil, and stirrup) that concentrate the vibrations of the eardrum on the cochlea’s oval window.
cochlea [KOHK-
inner ear the innermost part of the ear, containing the cochlea, semicircular canals, and vestibular sacs.
In your middle ear, three tiny bones (the hammer, anvil, and stirrup) pick up the vibrations and transmit them to the cochlea, a snail-
The incoming vibrations then cause the cochlea’s membrane-
The hair cell movements in turn trigger impulses in nerve cells, whose axons combine to form the auditory nerve. The auditory nerve carries the impulses to your thalamus and then on to your auditory cortex in your brain’s temporal lobe.
From vibrating air, to tiny moving bones, to fluid waves, to electrical impulses to the brain: You hear!
Perhaps the most magical part of the hearing process is the hair cells—
sensorineural hearing loss hearing loss caused by damage to the cochlea’s receptor cells or to the auditory nerves; the most common form of hearing loss, also called nerve deafness.
conduction hearing loss a less common form of hearing loss, caused by damage to the mechanical system that conducts sound waves to the cochlea.
Damage to the cochlea’s hair cell receptors or their associated nerves can cause sensorineural hearing loss (or nerve deafness). Occasionally, disease damages hair cell receptors, but more often the culprits are biological changes linked with heredity and aging, or prolonged exposure to ear-
154
 For an interactive review of how we perceive sound, visit LaunchPad’s PsychSim 6: The Auditory System. For an animated explanation, visit LaunchPad’s Concept Practice: The Auditory Pathway.
For an interactive review of how we perceive sound, visit LaunchPad’s PsychSim 6: The Auditory System. For an animated explanation, visit LaunchPad’s Concept Practice: The Auditory Pathway.
Hair cells have been compared to carpet fibers. Walk around on them and they will spring back. But leave a heavy piece of furniture on them and they may never rebound. As a general rule, any noise we cannot talk over (loud machinery, fans screaming at a sports event, music blasting at maximum volume) may be harmful, especially if we are exposed to it often or for a long time (Roesser, 1998). And if our ears ring after such experiences, we have been bad to our unhappy hair cells. As pain alerts us to possible bodily harm, ringing in the ears alerts us to possible hearing damage. It is hearing’s version of bleeding.
Worldwide, 1.23 billion people are challenged by hearing loss (Global Burden of Disease, 2015). Since the early 1990s, teen hearing loss has risen by a third and now affects 1 in 5 teens (Shargorodsky et al., 2010). Teen boys more than teen girls or adults blast themselves with loud volumes for long periods (Zogby, 2006). (Does it surprise you that men’s hearing tends to be less acute than women’s?) People who spend many hours behind a power mower, above a jackhammer, or in a loud club should wear earplugs, or they risk needing a hearing aid later. “Condoms or, safer yet, abstinence,” say sex educators. “Earplugs or walk away,” say hearing educators.
cochlear implant a device for converting sounds into electrical signals and stimulating the auditory nerve through electrodes threaded into the cochlea.
Nerve deafness cannot be reversed. For now, the only way to restore hearing is a sort of bionic ear—
How Do We Locate Sounds?
155
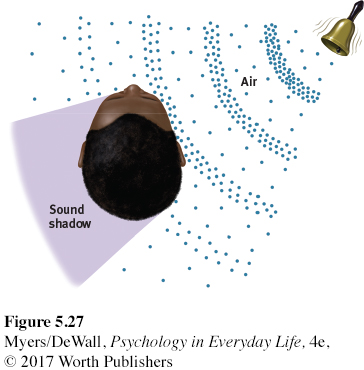
Why don’t we have one big ear—
Touch
LOQ 5-

If you had to lose one sense, which would you give up? If you could have only one, which would you keep?
Although not the first sense to come to mind, touch might be a good choice for keeping. Right from the start, touch enables our development. Infant monkeys allowed to see, hear, and smell—
Humorist Dave Barry was perhaps right to joke that your skin “keeps people from seeing the inside of your body, which is repulsive, and it prevents your organs from falling onto the ground.” But skin does much more. Our “sense of touch” is actually a mix of four basic and distinct skin senses: pressure, warmth, cold, and pain. Other skin sensations are variations of these four. For example, stroking side-
Touch sensations involve more than feelings on our skin, however. A soft touch on the leg evokes a different cortical response when a straight man believes he was caressed by an attractive woman rather than by another man (Gazzola et al., 2012). Such responses show how quickly our thinking brain influences our sensory responses. This thought-
Pain—What Is It and How Can We Control It?
LOQ 5-
Be thankful for occasional pain. Pain is your body’s way of telling you something has gone wrong. Drawing your attention to a burn, a break, or a sprain, pain orders you to change your behavior—
Many more people live with chronic pain, which is rather like an alarm that won’t shut off. Persistent backaches, arthritis, headaches, and cancer-
Our feeling of pain reflects both bottom-
156

BIOLOGICAL INFLUENCES Pain is a physical event produced by your senses. But pain differs from some of your other sensations. No one type of stimulus triggers pain, the way light triggers vision. And no specialized receptors process pain signals, the way the rods and cones in your eyes react to light rays. Instead, you have sensory receptors (nociceptors), mostly in your skin, which detect hurtful temperatures, pressure, or chemicals.
Your experience of pain also depends in part on the genes you inherited and on your physical characteristics. Women are more sensitive to pain than are men—
But pain is not merely a physical event in which injured nerves send impulses to a specific brain area—
Phantoms may haunt other senses, too. People with hearing loss often experience the sound of silence: tinnitus, a phantom sound of ringing in the ears. Those who lose vision to glaucoma, cataracts, diabetes, or macular degeneration may experience phantom sights—
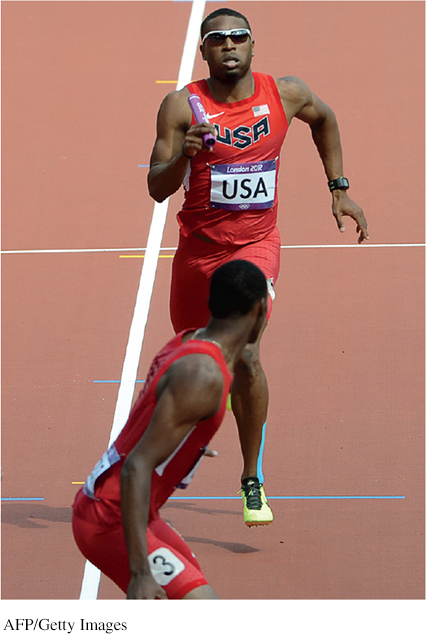
PSYCHOLOGICAL INFLUENCES One powerful influence on our perception of pain is the attention we focus on it. Athletes, focused on winning, may perceive pain differently and play through it. After a tackle in the first half of a competitive game, Swedish professional soccer player Mohammed Ali Khan said he “had a bit of pain” but thought it was “just a bruise.” He played on. In the second half he was surprised to learn from an attending doctor that his leg was broken. The pain in sprain is mainly in the brain.
We also seem to edit our memories of pain. The pain we experience may not be the pain we remember. In experiments, and after medical procedures, people overlook how long a pain lasted. Their memory snapshots instead record two points: the peak moment of pain, and how much pain they felt at the end. In one experiment, people put one hand in painfully cold water for 60 seconds, and then the other hand in the same painfully cold water for 60 seconds, followed by a slightly less painful 30 seconds more (Kahneman et al., 1993). Which experience would you expect they recalled as most painful?
Curiously, when asked which trial they would prefer to repeat, most preferred the longer trial, with more net pain—
SOCIAL-
157
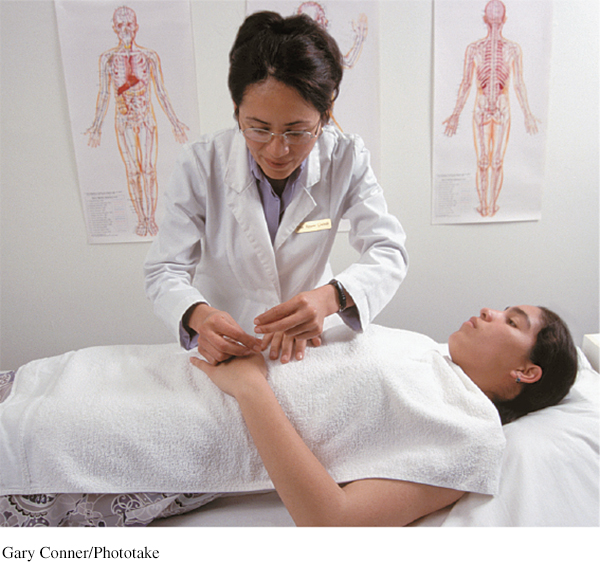
CONTROLLING PAIN If pain is where body meets mind—
We have some built-
“Pain is increased by attending to it.”
Charles Darwin, The Expression of the Emotions in Man and Animals, 1872
Even placebos can help, by dampening the central nervous system’s attention and responses to painful experiences—
When endorphins combine with distraction, amazing things can happen. Have you ever had a health care professional suggest that you focus on a pleasant image (“Think of a warm, comfortable environment”) or perform some task (“Count backward by 3s”)? These are effective ways to activate brain pathways that decrease pain and increase tolerance (Edwards et al., 2009). For burn victims receiving painful wound care, an even more effective distraction is escaping into a computer-
hypnosis a social interaction in which one person (the hypnotist) suggests to another person (the subject) that certain perceptions, feelings, thoughts, or behaviors will spontaneously occur.
Better yet, research suggests, maximize pain relief by combining a placebo with distraction (Buhle et al., 2012), and amplify their effects with hypnosis. Imagine you are about to be hypnotized. The hypnotist invites you to sit back, fix your gaze on a spot high on the wall, and relax. You hear a quiet, low voice suggest, “Your eyes are growing tired . . . Your eyelids are becoming heavy . . . now heavier and heavier . . . They are beginning to close . . . You are becoming more deeply relaxed . . . Your breathing is now deep and regular . . . Your muscles are becoming more and more relaxed. Your whole body is beginning to feel like lead.” After a few minutes of this hypnotic induction, you may experience hypnosis.
Hypnotists have no magical mind-
Can hypnosis relieve pain? Yes. Hypnosis inhibits pain-
But how does hypnosis work? Psychologists have proposed two explanations.
Social influence theory contends that hypnosis is a form of social influence—
a by- product of normal social and mental processes (Lynn et al., 1990, 2015; Spanos & Coe, 1992). In this view, hypnotized people, like actors caught up in a role, begin to feel and behave in ways appropriate for “good hypnotic subjects.” They may allow the hypnotist to direct their attention and fantasies away from pain. 158
posthypnotic suggestion a suggestion, made during a hypnosis session, to be carried out after the subject is no longer hypnotized; used by some clinicians to help control undesired symptoms and behaviors.
Dissociation theory proposes that hypnosis is a special dual-
processing state of dissociation— a split between normal sensations and conscious awareness. Dissociation theory seeks to explain why, when no one is watching, hypnotized people may carry out posthypnotic suggestions (which are made during hypnosis but carried out after the person is no longer hypnotized) (Perugini et al., 1998). It also offers an explanation for why people hypnotized for pain relief may show brain activity in areas that receive sensory information, but not in areas that normally process pain- related information (Rainville et al., 1997). Selective attention may also be at work (Chapter 2). Brain scans show that hypnosis increases activity in the brain’s attention systems (Oakley & Halligan, 2013). Thus, hypnosis doesn’t block the sensory input itself, but it may block our attention to those stimuli. This helps explain why injured soldiers, caught up in battle, may feel little or no pain until they reach safety.
So, is hypnosis to be explained as normal social influence or a special dissociative state? As the debate continues, stay tuned for further research.
Retrieve + Remember
Question 5.15
•Which of the following options has NOT been proven to reduce pain?
Distraction
Hypnosis
Phantom limb sensations
Endorphins
ANSWER: c
Taste
LOQ 5-
Like touch, our sense of taste involves several basic sensations. Taste’s sensations were once thought to be sweet, sour, salty, and bitter, with all others stemming from a mixture of these four (McBurney & Gent, 1979). Then, as researchers searched for specialized fibers for those four taste sensations, they discovered a fifth sensation—
Tastes give us pleasure, but they also help us survive. Pleasant tastes attracted our ancestors to foods rich in energy or protein (see TABLE 5.2). Unpleasant tastes warned them away from new foods that might be toxic. The taste preferences of today’s 2-
| Taste | Indicates |
|---|---|
| Sweet | Energy source |
| Salty | Sodium essential to physiological processes |
| Sour | Potentially toxic acid |
| Bitter | Potential poisons |
| Umami | Proteins to grow and repair tissue |
Taste is a chemical sense. Look into a mirror and you’ll see little bumps on the top and sides of your tongue. Each bump contains 200 or more taste buds. Each taste bud contains a pore that catches food chemicals. In each taste bud pore, 50 to 100 taste receptor cells project antenna-
It doesn’t take much to trigger receptor responses. If a stream of water is pumped across your tongue, the addition of a concentrated salty or sweet taste for only one-
Taste receptors reproduce themselves every week or two, so if hot food burns your tongue, it hardly matters. However, as you grow older, it may matter more, because the number of taste buds in your mouth will decrease, as will your taste sensitivity (Cowart, 1981). (No wonder adults enjoy strong-
159
There’s more to taste than meets the tongue. Our expectations also influence what we taste. When told a sausage roll was “vegetarian,” people in one experiment judged it inferior to its identical partner labeled “meat” (Allen et al., 2008). In another experiment, hearing that a wine cost $90 rather than its real $10 price made it taste better and triggered more activity in a brain area that responds to pleasant experiences (Plassman et al., 2008).
Smell

Inhale, exhale. Between birth’s first inhale and death’s last exhale, about 500 million breaths of life-
Smell, like taste, is a chemical sense. We smell something when molecules of a substance carried in the air reach a tiny cluster of receptor cells at the top of each nasal cavity. These 20 million olfactory receptors, waving like sea anemones on a reef, respond selectively—
For an animated explanation of how we smell, visit LaunchPad’s Concept Practice: Sense of Smell.
Odor molecules come in many shapes and sizes—
Aided by smell, a mother fur seal returning to a beach crowded with pups will find her own. Human mothers and nursing infants also quickly learn to recognize each other’s scents (McCarthy, 1986). A smell’s appeal—
Our sense of smell is less impressive than our senses of seeing and hearing. Looking out across a garden, we see its forms and colors in wonderful detail and hear a variety of birds singing. Yet we smell few of the garden’s scents without sticking our nose directly into the blossoms. We also have trouble recalling odors by name. But we have a remarkable capacity to recognize long-
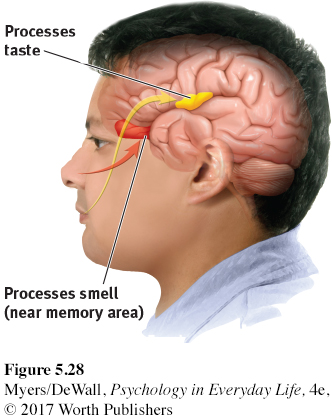
Our brain’s circuitry helps explain an odor’s power to evoke feelings, memories, and behaviors (FIGURE 5.28). A hotline runs between the brain area that receives information from the nose and other brain centers associated with emotions and memories. In experiments, people have become more suspicious when exposed to a fishy smell during a trust game (Lee & Schwarz, 2012). When exposed to a sweet taste, others became sweeter on their romantic partners and more helpful to others (Meier et al., 2012; Ren et al., 2015). And when riding on a train car with the citrus scent of a cleaning product, people left less trash behind (de Lange et al., 2012).
160
Retrieve + Remember
Question 5.16
•How does our system for sensing smell differ from our sensory systems for vision, touch, and taste?
ANSWER: We have two types of retinal receptors, four basic touch senses, and five taste sensations. But we have no specific smell receptors. Instead, different combinations of odor receptors send messages to the brain, enabling us to recognize some 1 trillion different smells.
Body Position and Movement
LOQ 5-
kinesthesia [kin-
Using only the five familiar senses we have so far considered, you could not put food in your mouth, stand up, or reach out and touch someone. Nor could you perform the “simple” act of taking one step forward. That act requires feedback from, and instructions to, some 200 muscles, and it engages brain power that exceeds the mental activity involved in reasoning. Like all your other voluntary movements, taking a step is possible because of your sense of kinesthesia, which keeps you aware of your body parts’ position and movement. You came equipped with millions of position and motion sensors in muscles, tendons, and joints all over your body. These sensors provide constant feedback to your brain. Twist your wrist one degree, and your brain receives an immediate update.
You can momentarily imagine being blind or deaf. Close your eyes, plug your ears, and experience the dark stillness. But what would it be like to live without the benefits of kinesthesia? Ian Waterman of Hampshire, England, knows. In 1972, at age 19, Waterman contracted a rare viral infection that destroyed the nerves that enabled his sense of light touch and of body position and movement. People with this condition report feeling disconnected from their body, as though it is dead, not real, not theirs (Sacks, 1985). With long practice, Waterman has learned to walk and eat—

Vision interacts with kinesthesia for you, too. Stand with your right heel in front of your left toes. Easy. Now close your eyes and try again. Did you wobble?
vestibular sense the sense of body movement and position, including the sense of balance.
A companion vestibular sense works hand in hand with kinesthesia to monitor your head’s (and thus your body’s) position and movement. Two structures in your inner ear join forces to help you maintain your balance. The first, your semicircular canals, look like a three-
If you twirl around and then come to an abrupt halt, it takes a few seconds for the fluid in your semicircular canals and for your kinesthetic receptors to return to their neutral state. The aftereffect fools your dizzy brain with the sensation that you’re still spinning. This illustrates a principle underlying perceptual illusions: Mechanisms that normally give us an accurate experience of the world can, under special conditions, fool us. Understanding how we get fooled provides clues to how our perceptual system works.
Retrieve + Remember
Question 5.17
•Where are kinesthetic sense and vestibular sense receptors located?
ANSWER: Kinesthetic sense receptors are located in our joints, tendons, and muscles. Vestibular sense receptors are located in our inner ear.