COSTLY CARE
In the United States, only 15 states currently mandate that health insurance policies must offer coverage for infertility treatment, and those that do often do not cover the more expensive treatments, like IVF. As a consequence, many patients must pay out of pocket. Because the costs of treatment are so high, many doctors find themselves under pressure to be aggressive with treatment with patients who have limited resources. Therefore, financial considerations can dictate a course of treatment, even when the treatment is unlikely to be successful or to be too successful, as in Suleman’s and Gosselin’s cases.
679
IVF has a higher success rate—about 40%, according to ASRM—but if the woman must undergo multiple rounds before becoming pregnant, the $12,400 price tag can be prohibitive.
As of 2013, a single insemination treatment (including fertility drugs and monitoring) can cost as much as $1,200—steep, but barely one-tenth the cost of an average in vitro fertilization cycle. Many couples may choose insemination over in vitro fertilization simply because it is less expensive, even though the procedure has a low success rate. On average, only 10% to 20% of all insemination treatments result in a live birth. But younger women and women who take fertility drugs and, as a result, have multiple ovulations, tend to have higher success rates. The multiple ovulations increase the odds of a successful pregnancy by insemination.
IVF has a higher success rate—about 40%, according to ASRM—but if the woman must undergo multiple rounds before becoming pregnant, the $12,400 price tag can be prohibitive. This financial burden can cause couples to hedge their bets by choosing to implant more embryos at one time than is typically recommended. The more embryos that are transferred into a woman’s uterus during each round of IVF, the higher the odds of a pregnancy.

680
In the wake of the revelation that Suleman had received multiple rounds of IVF, many people wanted to know how an unemployed 33-year-old with six children afforded to pay for the costly procedures. Suleman has said in interviews that she saved money for several years while working at a state mental hospital and later supported her family with money from student loans. The Associated Press and various newspapers also reported after the octuplets were born that Suleman received at least $165,000 in disability benefits from the state of California between 2002 and 2008 for an on-the-job injury she sustained in 1999. In addition, Suleman has said she received unemployment insurance and food stamps, as well financial support from the state for her other children, some of whom have disabilities. But even with this governmental support, given her large family and lack of an income, her financial resources would have been limited.
681
Medical details revealed during a court case brought by the California Medical Board in 2009 against Suleman’s doctor, Michael Kamrava, show that Kamrava created 14 embryos and implanted a dozen of them—six times the recommended number for a patient Suleman’s age. Eight embryos survived, and the babies were delivered 9 weeks prematurely by cesarean section (C-section). The Associated Press reported that during the hearing Kamrava said he regretted implanting the 12 embryos and “would never do it again.”

Kamrava further stated that Suleman was adamant about using all 12 embryos, even though he suggested implanting only 4. “She just wouldn’t accept doing anything else with those embryos. She did not want them frozen, she did not want them transferred to another patient in the future,” he said, according to the AP story. Kamrava said that he consented only after Suleman agreed to have a fetal abortion if necessary to reduce risk. After the implantation, however, he only heard from Suleman after the birth of her octuplets, despite his numerous attempts to contact her.
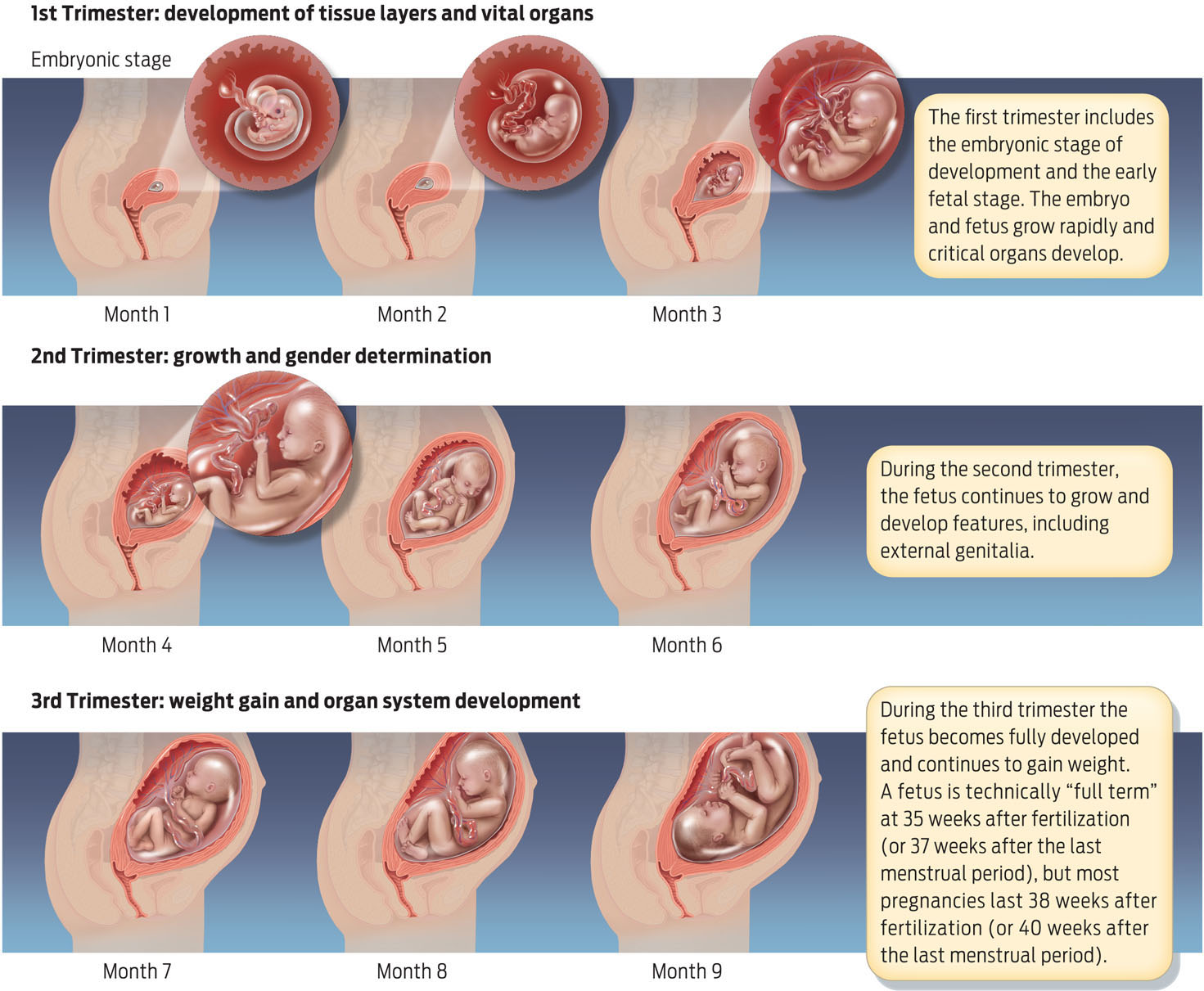
From a medical perspective, the birth of multiples from any assisted reproduction procedure carries risks. According to the March of Dimes, 50% of twins and 90% of triplets are born prematurely, as are virtually all quads and quintuplets. A premature baby is defined as one born before 37 completed weeks of pregnancy. When babies are born prematurely, their organs may not be fully developed, which can lead to medical problems. In particular, their lungs are often immature and so the babies must be hooked up to mechanical breathing ventilators, which sometimes scar the lungs so that these children will for the rest of their lives be prone to asthma, pneumonia, chronic lung disease, and other respiratory disorders. And because their brains aren’t fully developed, premature babies are susceptible to brain hemorrhages and to developmental difficulties, including learning disabilities (see UP CLOSE: PRENATAL DEVELOPMENT).
UP CLOSE PRENATAL DEVELOPMENT
Pregnancy is divided into three trimesters. A normal pregnancy lasts 38 weeks from the time of fertilization, which is 40 weeks from the last menstrual period.
These medical conditions impose a huge burden on the health care system. Experts who have considered Suleman’s case have stated that the medical bill for the delivery and postnatal care of her eight babies likely totaled $1.5 to $3 million. Kaiser Permanente, where Suleman delivered her babies, has asked MediCal, the tax payer-funded state health insurance system, to foot the bill.
To reduce the birth of multiples and prevent the associated health problems, in 2006 the ASRM recommended transferring no more than two embryos in women under 35 years of age and no more than five in women over 40, because as a woman ages the success rate tends to drop. These guidelines appear to have been helped: in 2009, 3.6% of all infants born via assisted reproduction were triplets, as compared to 6.4% in 2003. But assisted reproduction still results in a high number of twins—in 2009, 43% percent of births from IVF alone were twins, compared to 3% of all births.
682
If nothing else, these high profile cases have served as a wake-up call.
— BARBARA COLLURA
Despite the drop in multiple births, some lawmakers want more control. The risk that doctors may act against the ASRM guidelines, with negative consequences for women and their babies, remains.
After a lengthy investigation, the California Medical Board revoked Kamrava’s medical license, effective July 1, 2011. The Board claimed he was negligent not only in Suleman’s case, but also in the cases of two other women who suffered serious medical complications because of aggressive fertility treatments.
Lawmakers are concerned that there is nothing to prevent cases like these from happening again. Several states are considering legislation that would regulate doctors. A Missouri bill, for example, would require doctors not to exceed the ASRM’s embryo-transfer guidelines, while a Georgia bill would put a strict limit on the number of embryos that can be transferred. But experts fear that regulation would hinder good care. Fertility doctors need flexibility to tailor treatment to a couple’s individual condition of fertility, they argue. Such legislation “seeks to substitute the judgment of politicians for that of physicians and their patients,” ASRM president R. Dale McClure said in a statement evaluating the Georgia bill.
Instead of putting controls on doctors, some groups favor regulation that would require health insurers to cover infertility diagnostics and treatment, for example. The 2010 Affordable Care Act, passed by Congress and signed into law by President Obama, does not include infertility treatments in the “Essential Health Benefits” that health insurers will be required to cover beginning in 2014. However, it does make changes to the tax code that would allow individuals to write off a larger portion of the cost of these procedures on their income taxes.
As long as fertility treatment continues to be a financial burden on couples, fertility doctors will face pressure from patients to give them the most for their money, says Barbara Collura, executive director of RESOLVE, an infertility advocacy group. Broad health insurance coverage would eliminate the cost factor. The result might be that couples would be able to forgo treatments such as insemination that have high risks with low success rates and skip directly to IVF when appropriate.
“If nothing else, these high profile cases have served as a wake-up call,” says Collura. The community of health care workers is examining its own procedures and methods because it would rather self-regulate than have regulation imposed on it from the outside, she adds. “After Suleman, the community is really looking into how it [the birth of octuplets] happened and how it can prevent it from happening again.” 
683
FOR COMPARISON Why Do Organisms Have Sex?
Reproduction is a fundamental fact of life: all species must reproduce if they are to survive. But not all organisms reproduce in the same way, and not all have sex.
Sexual reproduction—reproduction that involves the combination of eggs and sperm from female and male individuals—occurs in most eukaryotic organisms: animals, plants, fungi, and protists. In humans and other mammals, fertilization of an egg by sperm occurs internally, in a female oviduct. This approach to sex allows the fertilized egg to be protected as it grows but limits the number of eggs that can be fertilized at any one time. Internal fertilization also requires that the male and female physically copulate in order to achieve fertilization. In humans and other mammals, the penis serves as a sperm delivery system to place sperm in a location where they can easily swim to the egg.
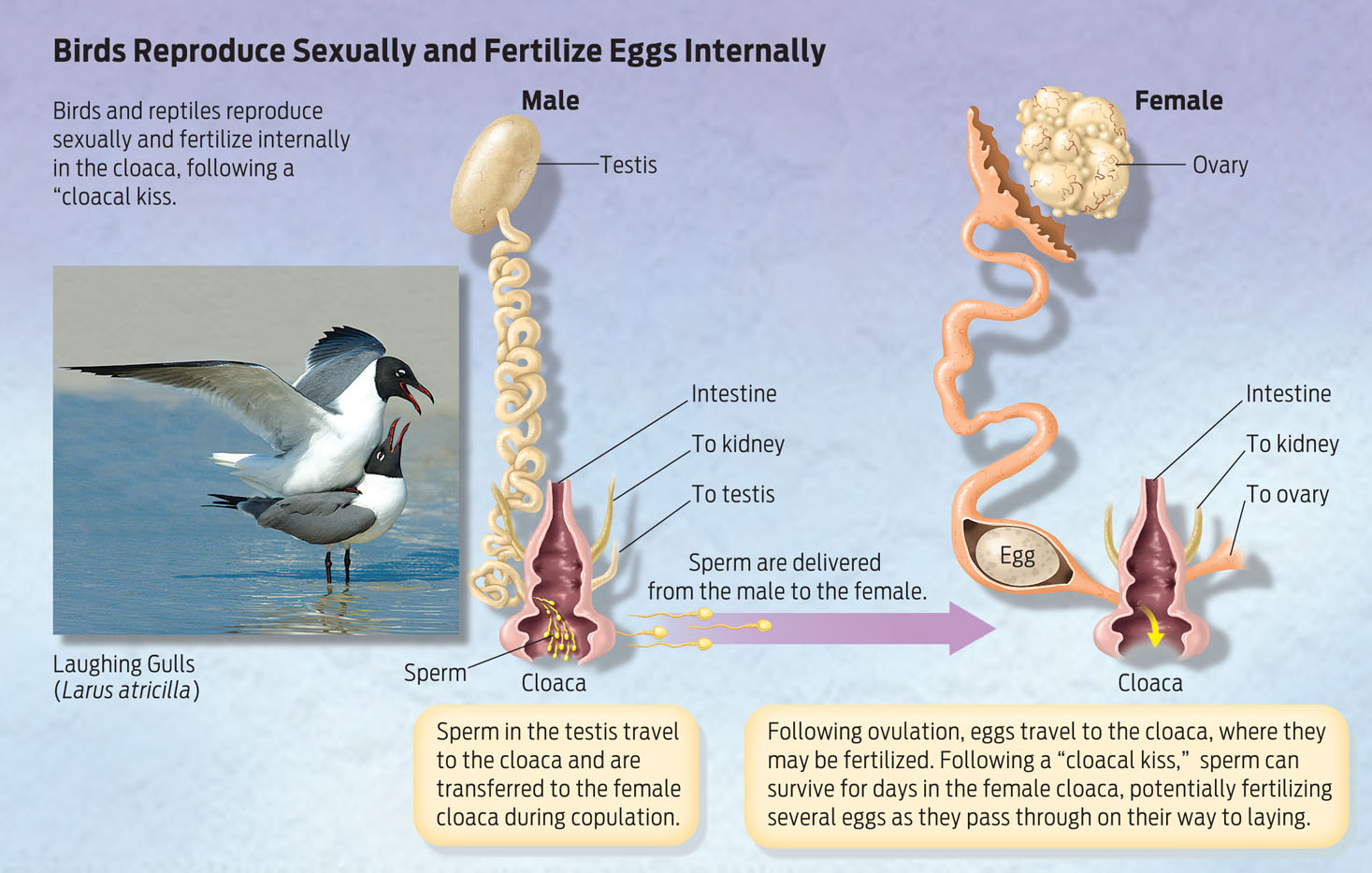
Many nonmammalian species also rely on internal fertilization, but use a very different sexual anatomy. Internal fertilization in birds and reptiles, for example, occurs in an organ called the cloaca (plural: “cloacae”). The cloaca is the shared opening for solid waste, urine, and the reproductive system. When birds have sex, they briefly touch their cloacae together in what’s called a cloacal kiss. This speedy kiss-and-run is sufficient to transfer sperm from the male to the female.
Interestingly, human female embryos have a cloaca, but the single cloacal opening divides into separate openings during embryonic development. In very rare cases, baby girls are born with an intact cloaca—having only one opening, rather than the usual three. Surgical correction to form distinct anal, vaginal, and urethral openings is possible in these cases.
684
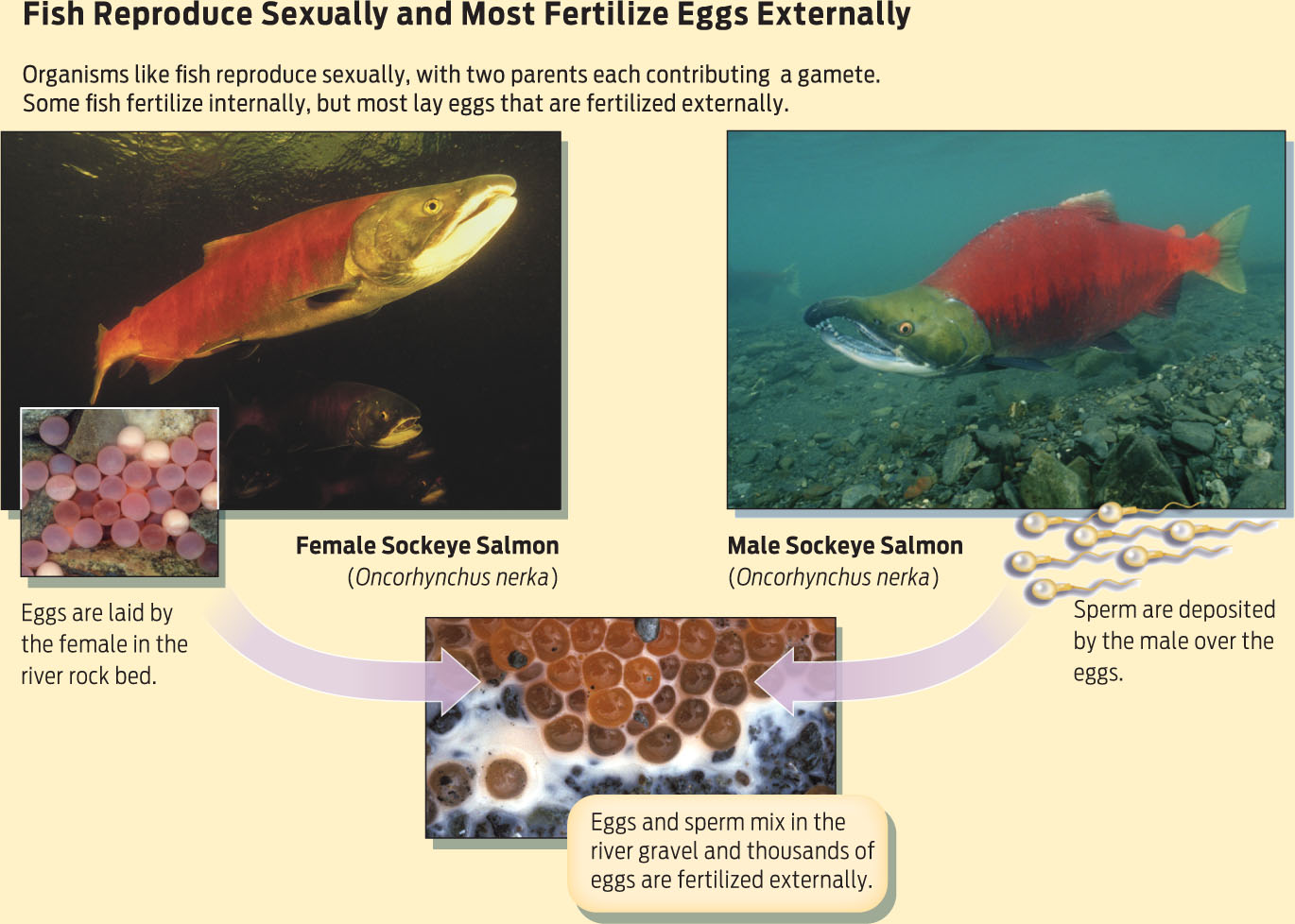
Not all sex takes place inside the body. Many fish and amphibians rely on external fertilization—their gametes fuse in the outside environment. Female salmon, for example, deposit their eggs in gravel nests in streambeds. Male salmon then swim over the eggs and release sperm, fertilizing thousands of eggs simultaneously. Other aquatic species such as coral and hydra also reproduce this way. Some plant species also practice external fertilization.
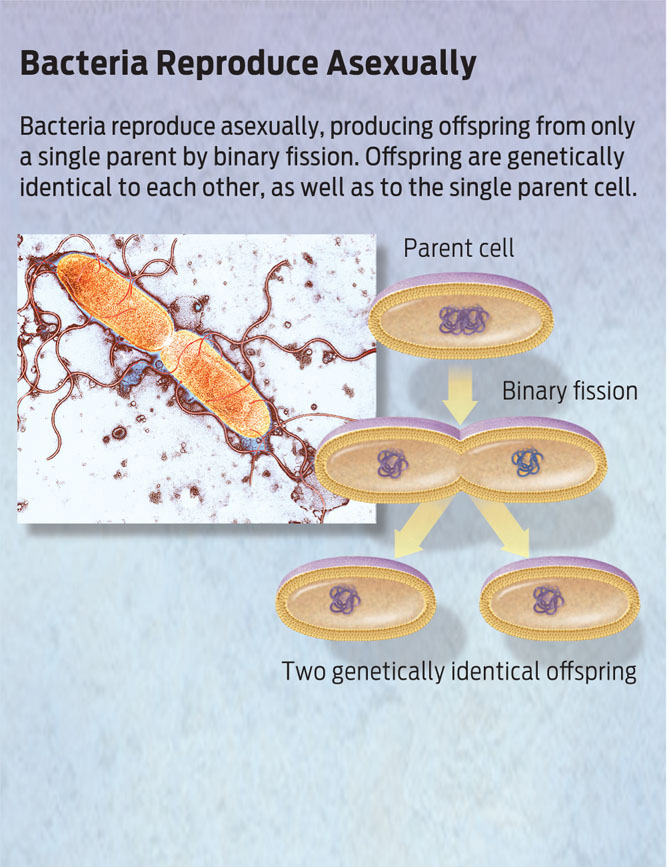
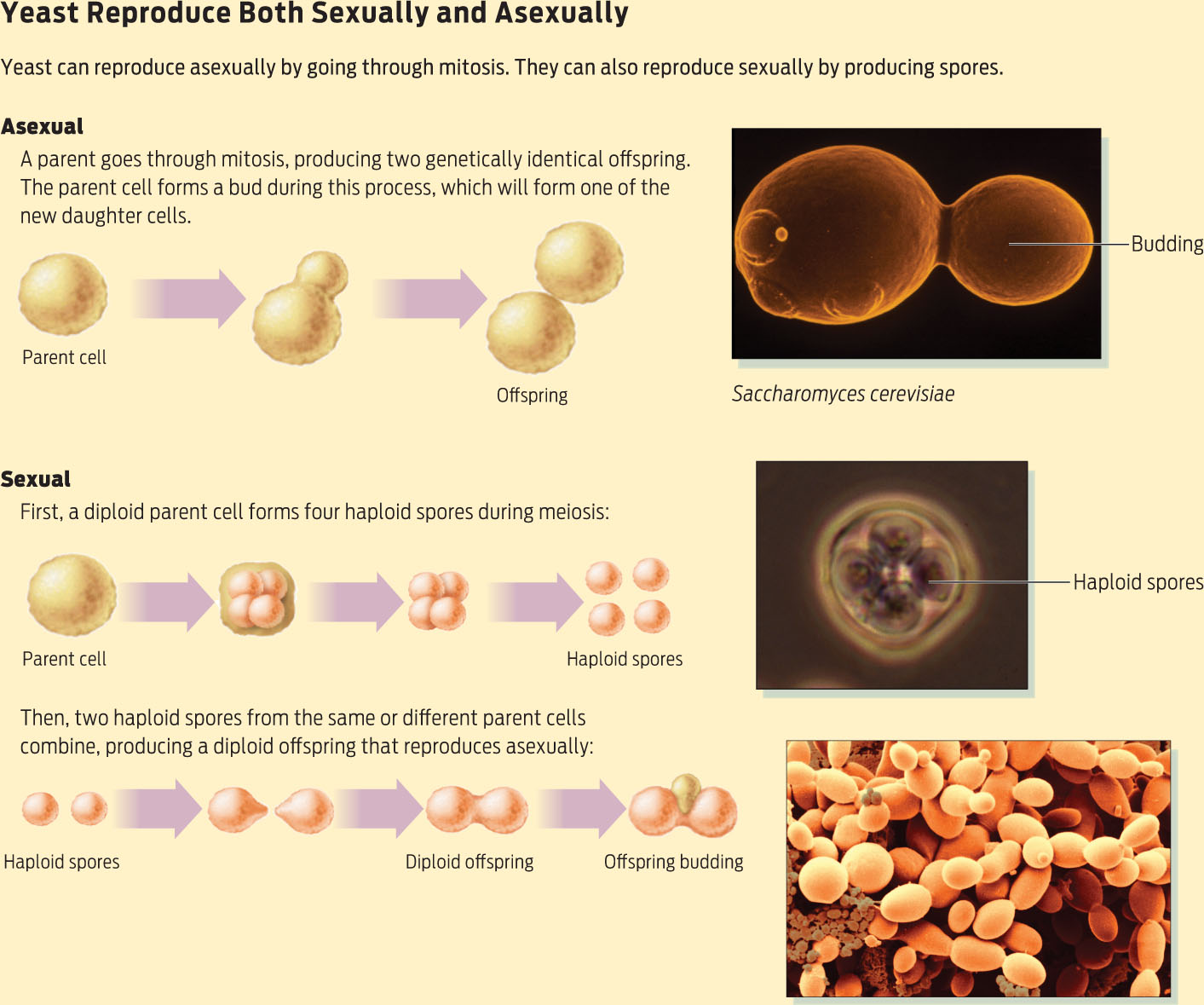
Many very successful creatures reproduce without having sex at all. Bacteria, for example, reproduce asexually—without additional genetic input from another individual. In asexual reproduction, a single parent cell simply divides to produce identical offspring. Some organisms, such as certain types of fungus, can reproduce both sexually and a sexually. Baker’s yeast (Saccharomyces cerevisiae) is a fungus that is commonly used to make bread rise. S. cerevisiae can produce gametes called spores, and these gametes can fuse to generate zygotes that develop into unicellular yeast. But both the spores and the yeast can also make exact copies of themselves by mitotic cell division, resulting in identical populations of cells.
685
If some organisms can reproduce on their own, without the involvement of a partner, why bother having sex at all? Biologists don’t fully understand why sex evolved, but they do have some good ideas. One hypothesis has to do with the evolutionary advantage of combining genetic information from two individuals. The resulting genetic diversity may enable offspring to better survive and adapt to changing environments—better than they would if each individual were identical to the parent.
686
But there are downsides to sex, too. Sexual reproduction generally takes longer than asexual reproduction. Certain bacteria, for example, can reproduce in as little as 20 minutes, which is a great evolutionary advantage in the race of natural selection. And sexual reproduction requires more energy and investment, especially on the part of the female. Internal fertilization, in particular, places a large demand on the mother. In the case of birds and reptiles, she has to produce an energy-rich egg in which the embryo will develop, and then in some cases protect it while it hatches. In most mammals, the maternal investment is even greater: she must supply all nutrients to a growing fetus and also provide a protective environment within her body during the long time it takes for a fetus to grow into a baby. However, this maternal investment, while leaving the mother vulnerable during the pregnancy, often results in the successful birth of a baby from each egg that is fertilized, compared to the exposed embryos that result from external fertilization, which are often eaten by predators before they ever mature.
Over time, different organisms have evolved different reproductive strategies that ensure that their offspring survive in the particular environment each organism occupies.
687