15.10 Self-Harm Behaviours: When the Mind Turns against Itself
We all have an innate drive to keep ourselves alive. We eat when we are hungry, get out of the way of fast-moving vehicles, and go to school so we can earn a living to keep ourselves, and our families, alive (see the discussion of evolutionary psychology in the Psychology: Evolution of a Science chapter). One of the most extreme manifestations of abnormal human behaviour is when a person acts in direct opposition to this drive for self-preservation and engages in intentionally self-destructive behaviour. Accounts of people intentionally harming themselves date back to the beginning of recorded history. However, it is only over the past several decades that we have begun to gain an understanding of why people purposely do things to hurt themselves. DSM–5 includes two self-destructive behaviours in its Section III (disorders in need of further study): suicide behaviour disorder and non-suicidal self-injury disorder.
15.10.1 Suicidal Behaviour

We all have an innate desire to keep ourselves alive. So why do some people purposely do things to harm themselves?
PIOTR POWIETRZYNSKI/GETTY IMAGES
Tim, a 35-year-old accountant, had by all appearances been living a pretty happy, successful life. He was married to his high school sweetheart and had two young children. Over the past several years, though, his workload had increased and he started to experience severe job-related stress. At around the same time, he and his wife began to experience some financial problems, and his alcohol consumption increased, all of which put significant strain on the family and began to affect his work. Tim’s co-workers noted that he had become pretty angry and agitated lately—even yelling at co-workers on a few occasions. One evening Tim and his wife got into a heated argument about the family’s finances and Tim’s excessive alcohol use; Tim went into the bathroom and swallowed a bottle full of prescription medicine in an effort to end his life. He was taken to the hospital and kept there to be treated for suicidal behaviour.
Suicide, which refers to intentional self-inflicted death, is the second most common cause of death for people aged 15 to 34 in Canada, claiming 18 out of every 100 000 males, and 5 out of every 100 000 females aged 10 and older (Statistics Canada, 2014). There are large demographic differences in the suicide rate: For instance, in Canada, 75 percent of suicides occur among men, and immigrants are only about half as likely as those born in Canada to commit suicide (Malenfant, 2004). Rates of suicide in Canadian Aboriginal populations are much higher: 56 out of 100 000 for males, and almost 12 out of 100 000 for females (Society, the Individual, and Medicine [SIM], 2013). Unfortunately, we currently do not have a good understanding of why these enormous sociodemographic differences exist.
Nonfatal suicide attempt, in which a person engages in potentially harmful behaviour with some intention of dying, occurs much more frequently than suicide deaths. Across a range of countries, approximately 9 percent of adults report that they have seriously considered suicide at some point in their lives, 5 percent have made a plan to kill themselves, and 5 percent have actually made a suicide attempt (Nock et al., 2008). As these numbers suggest, only one third of those who think about suicide actually go on to make a suicide attempt. Although many more men than women die by suicide, women experience suicidal thoughts and (nonfatal) suicide attempts at significantly higher rates than do men (Nock et al., 2008). Moreover, the rates of suicidal thoughts and attempts increase dramatically during adolescence and young adulthood. A recent study of a representative sample of approximately 10 000 adolescents in the United States revealed that suicidal thoughts and behaviours are virtually nonexistent before age 10, but then increase dramatically from age 12 to 18 years (see FIGURE 15.7) before leveling off during early adulthood (Nock et al., 2013).
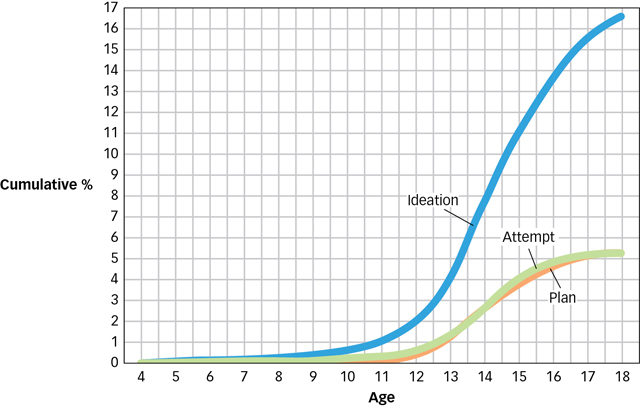
Figure 15.7: Age of Onset of Suicidal Behaviour During Adolescence A recent survey of adolescents in the United States shows that although suicidal thoughts and behaviours are quite rare among children (the rate was 0.0 for ages 1 to 4), they increase dramatically starting at age 12 and continuing to climb throughout adolescence.
(Adapted from Nock et al., 2013.)
What are some of the factors that contribute to suicidal behaviour?
The numbers are staggering, but why do people try to kill themselves? The short answer is: We do not yet know, and it is complicated. When interviewed in the hospital following their suicide attempt, most people who have tried to kill themselves report that they did so in order to escape from an intolerable state of mind or impossible situation (Boergers, Spirito, & Donaldson, 1998). Consistent with this explanation, research has documented that the risk of suicidal behaviour is significantly increased if a person experiences factors that can create severely distressing states such as the presence of multiple mental disorders (more than 90 percent of people who die by suicide have at least one mental disorder); the experience of significant negative life events during childhood and adulthood (e.g., physical and sexual assault); and the presence of severe medical problems (Nock, Borges, & Ono, 2012). The search is ongoing for a more comprehensive understanding of how and why some people respond to negative life events with suicidal thoughts and behaviours, as well as on methods of better predicting and preventing these devastating outcomes.
15.10.2 Non-suicidal Self-Injury
Louisa, an 18-year-old university student, secretly cuts her lower waist and upper thighs about once per week, typically when she is in the midst of feeling intense anger and hatred, either toward herself or someone else. She has always had a bit of a “hot streak” as she calls it, but it was not until she turned 14 that she started to use self-injury as a way to calm herself down. Louisa says that she actually feels a little ashamed after each episode of cutting, but she does not know how else to calm down when she gets really upset and so she has no plans of stopping this behaviour.
Louisa is engaging in a behaviour called non-suicidal self-injury (NSSI), the direct, deliberate destruction of body tissue in the absence of any intent to die. NSSI has been reported since the beginning of recorded history; however, it is a behaviour that appears to be on the rise over the past few decades. Recent studies suggest that as many as 15 to 20 percent of adolescents and 3 to 6 percent of adults report engaging in NSSI at some point in their lifetime (Klonsky, 2011; Muehlenkamp et al., 2012). The rates appear to be even between males and females, and for people of different races and ethnicities. Like suicidal behaviour, NSSI is virtually absent during childhood, increases dramatically during adolescence, and then appears to decrease across adulthood.

Although in Canada self-injury is considered to be pathological, in some parts of the world scarification of the skin is viewed as a rite of passage into adulthood and a symbol of one’s tribe, as in the case of this young man from the Republic of Benin in West Africa.
JEAN-MICHEL CLAJOT/AURORA PHOTOS
What is known so far about why people engage in self-injury?
In some parts of the world, cutting or scarification of the skin is socially accepted, and in some cases encouraged as a rite of passage (Favazza, 2011). In parts of the world where self-cutting is not socially encouraged, why would a person purposely hurt him- or herself if not to die? Recent studies suggest that people who engage in self-injury have very strong emotional and physiological responses to negative events, that they perceive this response as intolerable, and that NSSI serves to diminish the intensity of this response (Nock, 2009). There also is some evidence that in many instances, people engage in self-injury as a means to communicate distress or elicit help from others (Nock, 2010). Although we are beginning to get an understanding of why some people engage in NSSI, there are many aspects of this behaviour that we do not yet understand, and the study of NSSI is an increasingly active area of research.
Unfortunately, like suicidal behaviour, our understanding of the genetic and neurobiological influences on NSSI is limited, and there currently are no effective medications for these problems. There also is very limited evidence for behavioural interventions or prevention programs (Mann et al., 2005). So, whereas suicidal behaviour and NSSI are some of the most disturbing and dangerous mental disorders, they also, unfortunately, are among the most perplexing. The field has made significant strides in our understanding of these behaviour problems in recent years, but there is a long way to go before we are able to predict and prevent them accurately and effectively.
Suicide is among the leading causes of death. Most people who die by suicide have a mental disorder, and suicide attempts are most often motivated by an attempt to escape intolerable mental states or situations.
NSSI, like suicidal behaviour, increases dramatically during adolescence, but for many is a persistent problem throughout adulthood. Although NSSI is performed without suicidal intent, like suicidal behaviour, it is most often motivated by an attempt to escape from painful mental states.