6.4 The Biology of Memory
247
What did you do today? Did you have breakfast, brush your teeth, put your clothes on, drive your car, read an assignment, text a friend? Whatever you did, we are sure of one thing: It required a whole lot of memory. You could not send a text message without knowing how to spell, read, and use a cell phone—
If memory is behind all your daily activities, important processes must be occurring in the brain to make this happen: both on the macro (large) and micro (small) scale. But as we learned from Clive’s example, these processes are fragile and can be profoundly disrupted. Exploring the causes of memory failure can help us understand the biological basis of memory.
Amnesia
LO 13 Compare and contrast anterograde and retrograde amnesia.
Clive forgot many things, but not the love he has for his wife. Every time Deborah came to visit, he recognized her but could not recall their last meeting, even if it happened just minutes before. Hugging, kissing, and sometimes twirling Deborah in the air, he would ask how much time had passed (Wearing, 2005).
 In the months and years following Clive’s illness, researchers administered many tests to assess his cognitive functioning. They found his IQ to be within an average range but his ability to remember past events deeply impaired. When prompted to name as many musical composers as possible in 1 minute, Clive—
In the months and years following Clive’s illness, researchers administered many tests to assess his cognitive functioning. They found his IQ to be within an average range but his ability to remember past events deeply impaired. When prompted to name as many musical composers as possible in 1 minute, Clive—
Clive was even more disabled when it came to developing new memories. Initially, he could not hold onto incoming information for more than a blink of an eye. If his wife Deborah left the room, even for a short trip to the restroom, he would welcome her back as if she had been away for years—
Amnesia, or memory loss, can result from either a physical or psychological condition. There are different types and degrees of amnesia, ranging from extreme (losing decades of autobiographical memories) to mild (temporarily forgetting people’s names after a concussion).
anterograde amnesia (an-
ANTEROGRADE AMNESIA According to researchers, Clive suffers from “a more severe anterograde amnesia than any other patient previously reported” (Wilson et al., 1995, p. 680). Anterograde amnesia (an-
248
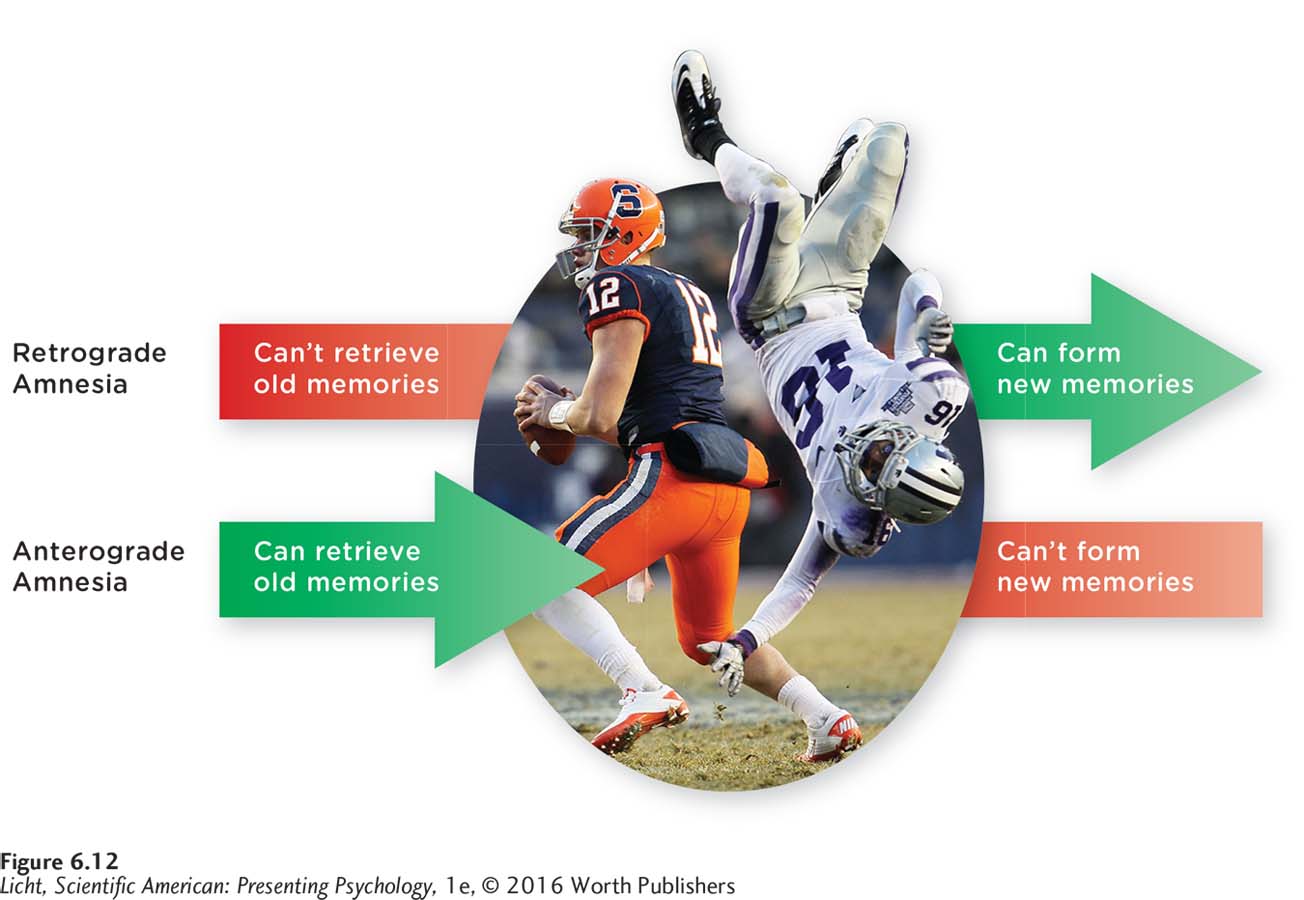
Retro means “before,” so retrograde amnesia is the inability to retrieve memories for events that occurred before an amnesia-
Chris McGrath/Getty Image
retrograde amnesia A type of memory loss; an inability to access memories formed prior to damage or injury to the brain, or difficulty retrieving them.
RETROGRADE AMNESIA A second type of memory loss is retrograde amnesia, an inability to access memories created before a brain injury or surgery (Brandt & Benedict, 1993; Figure 6.12). With retrograde amnesia, a person has difficulty retrieving old memories, though how “old” depends on the extent of trauma to the brain. People with retrograde amnesia generally remember who they are and the most important events of their earlier lives (Manns, Hopkins, & Squire, 2003; Squire & Wixted, 2011). Remember that retrograde refers to the inability to access old memories, and anterograde refers to the inability to create new memories.
Clive suffered from retrograde amnesia in addition to his anterograde amnesia. While he appeared to retain a vague outline of his past (hazy information about his childhood, the fact that he had been a choral scholar at Clare College, Cambridge, and so on), he could not retrieve the names of his children unless prompted. And although Clive’s children were all adults when he developed encephalitis, he came out of the illness thinking they were young children. The retrograde amnesia has improved, but only minimally. In 2005, for example, Clive asked his 40-
In spite of the severe retrograde and anterograde amnesia, some of Clive’s memory functions continued to operate quite well. At one point, Deborah arranged for Clive to be reunited with the singers from the London Lassus Ensemble, a group he had conducted for more than a decade before his illness. At first Clive paused and looked at the musicians with uncertainty, but then he raised his hands and began conducting, leading them through the music with precision and grace. Remembering the piece (which he had edited himself), Clive mouthed its words in Latin and employed the same tempo and conducting style he had used in the past (D. Wearing, personal communication, July 11, 2013). After the performance, the musicians left and Clive sat in the empty chapel wondering what had gone on there earlier (Wearing, 2005). When shown a video of himself leading the chorus, he remarked, “I wasn’t conscious then” (Wilson et al., 2008). Clive’s explicit memory of the event vanished in seconds, but his implicit memory—
249
How is it possible that some of Clive’s long-
Where Memories Live in the Brain: A Macro Perspective
LO 14 Identify the brain structures involved in memory.
CONNECTIONS
In Chapter 2, we described the hippocampus as a pair of curved structures buried deep within the temporal lobes. The hippocampus is primarily responsible for processing and making new memories, but is not where memories are permanently stored. It is also one of the brain areas where neurogenesis occurs, that is, where new neurons are generated.
A few years after the onset of Clive’s illness, doctors evaluated his brain using an MRI scan. A troubling picture emerged; the virus had destroyed many parts of his brain, notably the hippocampus, which plays a vital role in the creation of new memories (Wilson et al., 2008).
memory trace The location where memories are etched in the brain via physiological changes.
Only in the last 50 years have scientists come to appreciate the role of the hippocampus in memory (Infographic 6.3). Back in the 1920s, psychologist Karl Lashley set out to find a memory trace: the physical spot where memories are etched in the brain, also called an engram. Lashley selected a group of rats that had learned the layout of specific mazes, and then made large cuts at different places in their cortices to see how this affected their memory of the mazes. No matter where Lashley sliced, the rats still managed to maneuver their way through the mazes (Costandi, 2009, February 10; Lashley, 1950). These findings led Lashley and other scientists to believe that memory is spread throughout the brain rather than localized in a particular region (Costandi, 2009, February 10; Kandel & Pittenger, 1999). Connectionism is a model that suggests our memories are distributed throughout the brain in a network of interlinked neurons.
Synonyms
connectionism parallel distributed processing (PDP)
INFOGRAPHIC 6.3
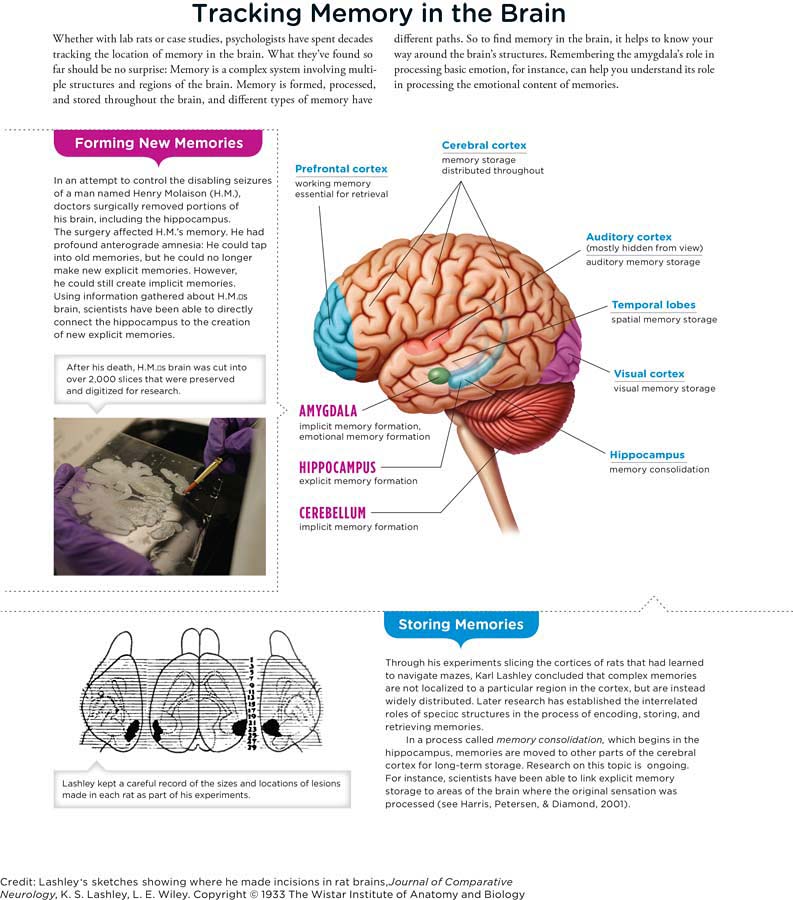
THE CASE OF H.M. Henry Molaison (better known as “H.M.”) forced scientists to completely reevaluate their understanding of the brain’s memory system. From the onset of his amnesia in 1953 until his death in 2008, H.M. served as a research participant for some 100 scientists (Corkin, 2002), making him the most extensively studied amnesic patient.
H.M.’s brain troubles began at the age of 10, a year or so after being knocked unconscious in a bicycle accident. He began to experience seizures, which worsened with age and eventually became so debilitating that he could no longer hold a steady job. Antiseizure medications were unsuccessful in controlling his seizures, so at the age of 27, H.M. opted for an experimental surgery to remove parts of his brain: the temporal lobes (just beneath the temples), including the hippocampus (Scoville & Milner, 1957).

Dr. Jacopo Annese, director of the Brain Observatory at the University of San Diego, stands in front of a massive digital image rendered from a slice of brain tissue preserved on a slide. Dr. Annese and his team have carved the brain of amnesiac Henry Molaison, or “H.M.,” into 2,401 slices to be digitized and studied (Brain Observatory, 2013).
H.M.’s surgery succeeded in reining in his epilepsy but left his memory in shambles. Upon waking from the operation, he could no longer find his way to the bathroom or recognize the hospital workers caring for him. He played with the same jigsaw puzzles and read the same magazines day after day as if he were seeing them for the first time (Scoville & Milner, 1957). Like Clive, H.M. suffered from profound anterograde amnesia, the inability to encode new long-
250
251
H.M. maintained a working implicit memory, which he demonstrated in an experiment involving the complex task of tracing a pattern reflected in a mirror. With repeated practice sessions (none of which he remembered), H.M. improved his performance on the drawing task, learning it as well as someone without amnesia (Gabrieli, Corkin, Mickel, & Growdon, 1993). Clive can also acquire new implicit memories, but his ability is very limited. According to Deborah, it took years for Clive to learn how to get to his bedroom in the small community residence where he moved after leaving the hospital (Wearing, 2005).
THE ROLE OF THE HIPPOCAMPUS Imagine you are a scientist trying to figure out exactly what role the hippocampus plays in memory. Consider the facts you know about H.M.: (1) He has virtually no hippocampus; (2) he has lost the ability to make new explicit memories, yet can create implicit memories; and (3) he can still tap into memories of the distant past. So what do you think the hippocampus does? Evidence suggests that the hippocampus is essential for creating new explicit memories but not implicit memories. Researchers have also shown that explicit memories are processed and stored in other parts of the brain, including the temporal lobes and areas of the frontal cortex (García-
As in H.M.’s case, Clive’s ability to form explicit memories is profoundly compromised, largely a result of the destruction of his hippocampus. Yet Clive also struggles with the creation of implicit memories—
So although the hippocampus plays a central role in laying down new memories, it does not appear to serve as their ultimate destination. This process of memory formation, which moves a memory from the hippocampus to other areas of the brain, is called memory consolidation (Squire & Bayley, 2007). The consolidation that begins in the hippocampus allows for the long-
This idea that the hippocampus is essential for creating explicit memories (as opposed to implicit memories) is supported by what we know about infantile amnesia, that is, the inability to remember events from our earliest years. Most adults cannot remember events before the age of 3, though it is not clear why. Some researchers suggest that it is because the hippocampus and frontal cortex, both important for the creation of long-
This macrolevel perspective allows us to see the “big picture” of memory, but what’s going on microscopically? The next section focuses on the important changes occurring in and between neurons.
Where Memories Live in the Brain: A Micro Perspective
CONNECTIONS
In Chapter 2, we introduced the synapse: the tiny gap between two neurons. Neurons communicate with each other via chemicals called neurotransmitters, which are released into the synapse. Here, we see how the activities at the neural level are related to the formation and maintenance of memories.
252
LO 15 Describe long-
How does your brain change when you learn a new driving route to school? If we could peer into your skull, we might see a change in your hippocampus. As one study found, London taxicab drivers with greater time spent on the job had structural changes in some regions of the hippocampus, particularly to an area that processes “spatial knowledge” (Maguire, Woollett, & Spiers, 2006). Zooming in for a closer look, we might actually see changes at the level of the neuron. If you are looking for a memory imprint, the best place to look is the synapse.
long-

Studying the neurons of sea slugs, researchers have observed the synaptic changes that underlie memory. Long-
LONG-
CONNECTIONS
In Chapter 5, we discussed classical conditioning and how a neutral stimulus can be paired with an unconditioned stimulus, ultimately leading to a conditioned stimulus resulting in a conditioned response. In the case of the sea slug, the squirt of water is the conditioned stimulus and its involuntary response of retracting its gills is the conditioned response.
APLYSIA Amazingly, we have learned much about long-
ALZHEIMER’S DISEASE On a less positive note, disruptions in long-
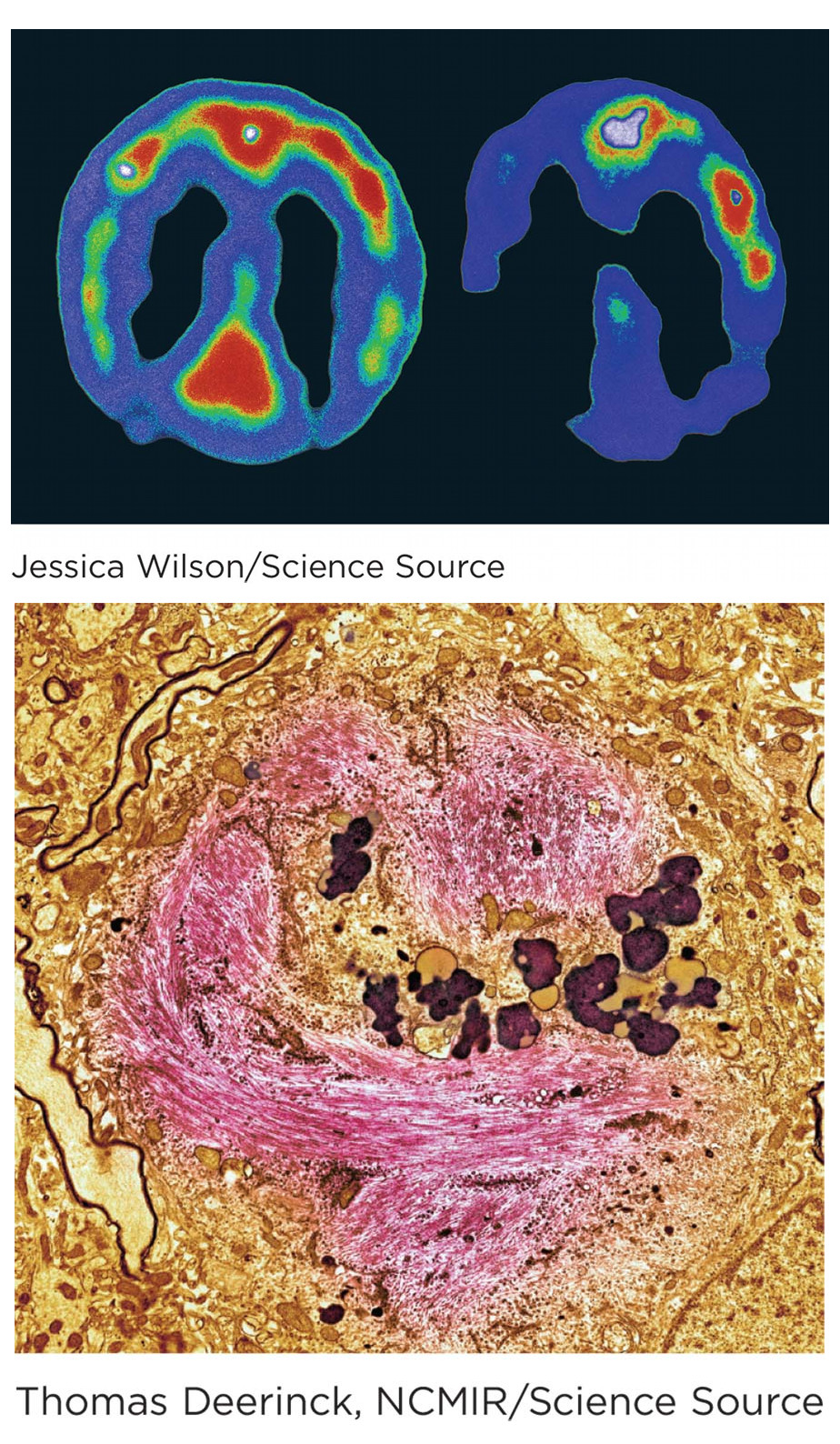
The PET scan (top left) depicts the brain of a normal person, while the scan to its right shows that of a person with Alzheimer’s. Studies using PET suggest a slowing of brain activity in certain regions of the Alzheimer’s brain (Alzheimer’s Association, 2013). The neurofibrillary tangles (bottom image, with tangles in pink) result from twisted protein fibers accumulating inside brain cells.
253
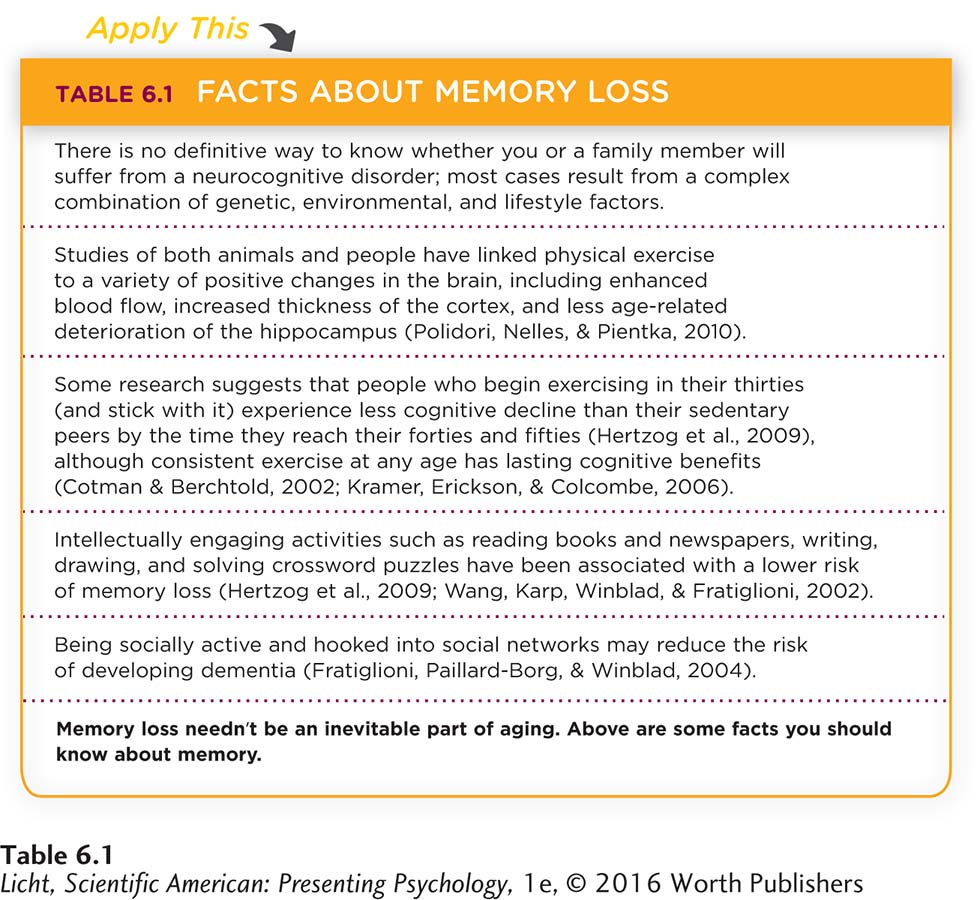
There is no cure for Alzheimer’s disease, and current treatments focus only on reducing the severity of symptoms rather than correcting the brain damage responsible. But there is also reason to be hopeful. Promising new drugs are coming down the pipeline, and there is some preliminary evidence suggesting that simple lifestyle changes, like becoming more physically active and pursuing intellectually and socially stimulating activities, may actually decrease the speed and severity of cognitive decline (Hertzog, Kramer, Wilson, & Lindenberger, 2009, July/August; Wilson & Bennett, 2003). Additional good news comes from research suggesting that we should not think of cognitive decline as inevitable in aging. We have more control of aging than previously thought, especially when we focus on the lifelong possibilities of learning and autonomy (Hertzog et al., 2009). Furthermore, it’s not only the strengthening of synapses that makes for enduring memories, but also the activation of new ones (Yu, Ponomarev, & Davis, 2004), and this process could offset cognitive decline (Table 6.1).
Like many topics psychologists study, the biological mechanisms that give rise to memory remain somewhat mysterious. We know we have memories; we know they are formed in the brain; and we know the brain is a physical entity, yet we still don’t know exactly how we go from a bunch of firing neurons to a vivid recollection of your 21st birthday bash, your high school prom, or the image of Bruno Mars banging on his drums at the Super Bowl halftime show. Studies attempting to test the various theories of memory formation are inconclusive, often generating more questions than answers. But one thing seems certain: Memory researchers have plenty of exciting work ahead.
show what you know
254
Question 1
1. __________ refers to the inability to lay down new long-
Anterograde amnesia
Retrograde amnesia
Infantile amnesia
Long-
term potentiation
a. Anterograde amnesia
Question 2
2. The __________ is a pair of curved structures in the brain that play a central role in memory.
engram
temporal lobe
hippocampus
aplysia
c. hippocampus
Question 3
3. __________ is the process of memory formation, which moves a memory from the hippocampus to other areas of the brain.
Long-
term potentiation Memory consolidation
Priming
The memory trace
b. Memory consolidation
Question 4
4. Infantile amnesia makes it difficult for people to remember events that occurred before the age of 3. What is your earliest memory and how old were you when that event occurred?
Answers will vary, but can be based on the following information. Infantile amnesia is the inability to remember events from one’s earliest years. Most adults cannot remember events before the age of 3.
FINAL THOUGHTS At this point, you may be wondering what became of the two people featured in this chapter, Clive Wearing and Dorothea Seitz. After living in the hospital for 7 years, Clive moved to a country residence specially designed for people suffering from brain injuries. As he left the hospital, some of the staff members offered him a farewell and said they would miss him. Addressing them with a polite bow, Clive exclaimed, “You’re the first people I’ve seen!” When Deborah would visit Clive in his new home, she found him happy and relaxed, spending much of his time on walks through gardens and the local village (Wearing, 2005, p. 293). In 2002 Clive and Deborah renewed their marriage vows. Clive participated fully in the service, reciting scripture he had memorized during his career as a professional singer decades before (D. Wearing, personal communication, June 10, 2013). After the ceremony, he had no recollection of what had taken place but nevertheless was very happy, laughing and devouring sponge cake (Wearing, 2005).
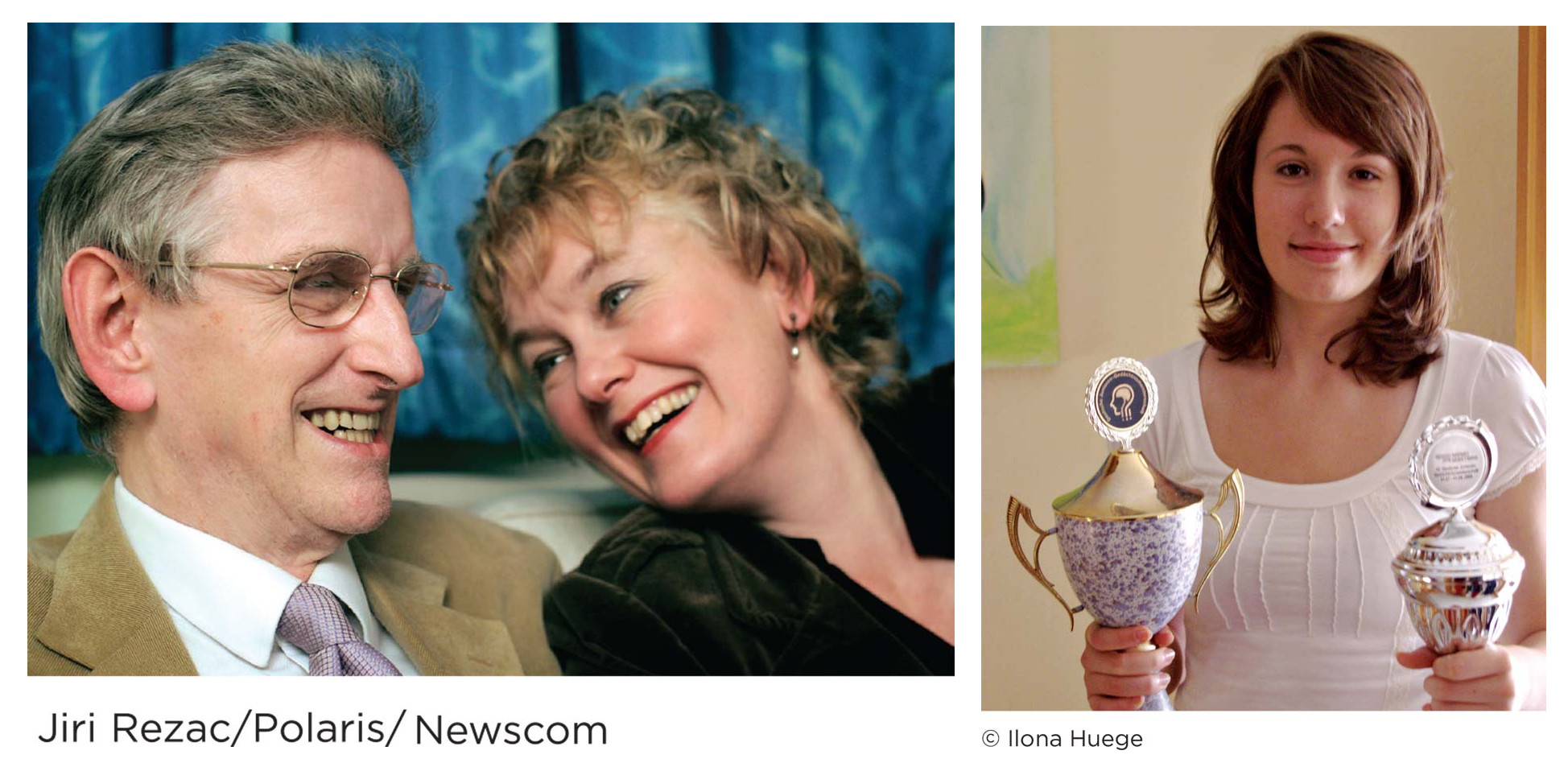
(left) Nearly two decades after falling ill, Clive renewed his wedding vows with Deborah. Now in his seventies, Clive lives in a country residence for people suffering from brain injuries (Vennard, 2011, November 21). (right) Dorothea became the Junior World Memory Champion for the second time in 2009. Although she no longer competes in memory sport, she continues to exercise her intellect as a student of political science and sociology.
 As for Dorothea, she succeeded in defending her title of Junior World Memory Champion in 2009 and finished the competition in 11th place overall. After completing high school, Dorothea spent a year doing volunteer work in Peru. She is currently studying political science and sociology in Freiburg, Germany.
As for Dorothea, she succeeded in defending her title of Junior World Memory Champion in 2009 and finished the competition in 11th place overall. After completing high school, Dorothea spent a year doing volunteer work in Peru. She is currently studying political science and sociology in Freiburg, Germany.