Treatments for Anorexia Nervosa
The immediate aims of treatment for anorexia nervosa are to help people regain their lost weight, recover from malnourishment, and eat normally again. Therapists must then help them to make psychological and perhaps family changes to lock in those gains.
How Are Proper Weight and Normal Eating Restored? A variety of treatment methods are used to help patients with anorexia nervosa gain weight quickly and return to health within weeks. In the past, treatment almost always took place in a hospital, but now it is often offered in day hospitals or outpatient settings (Raveneau et al., 2014; Keel & McCormick, 2010).
In life-threatening cases, clinicians may need to force tube and intravenous feedings on a patient who refuses to eat (Rocks et al., 2014; Touyz & Carney, 2010). Unfortunately, this use of force may cause the client to distrust the clinician. In contrast, clinicians using behavioral weight-restoration approaches offer rewards whenever patients eat properly or gain weight and offer no rewards when they eat improperly or fail to gain weight (Tacón & Caldera, 2001).
Perhaps the most popular weight-restoration technique in recent years has been a combination of supportive nursing care, nutritional counseling, and a relatively high-calorie diet—often called a nutritional rehabilitation program (Leclerc et al., 2013). Here nurses gradually increase a patient’s diet over the course of several weeks to more than 3,000 calories a day (Zerbe, 2010, 2008; Herzog et al., 2004). The nurses educate patients about the program, track their progress, provide encouragement, and help them recognize that their weight gain is under control and will not lead to obesity. In some programs, the nurses also use motivational interviewing, an intervention in which they motivate clients to actively make and follow through on constructive choices regarding their eating behaviors and their lives (Dray et al., 2014). Studies find that patients in nursing-care programs usually gain the necessary weight over 8 to 12 weeks.
Page 299

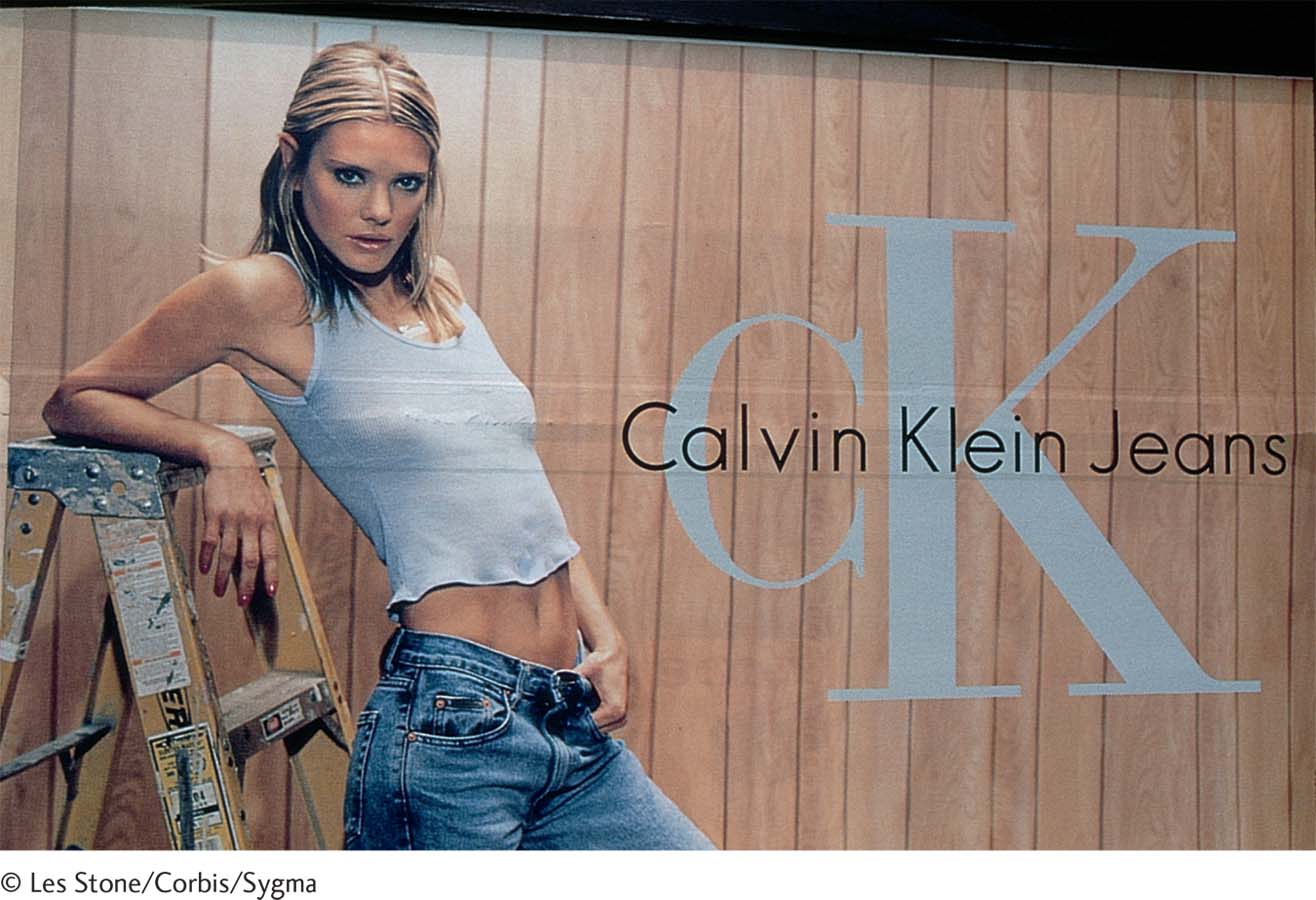
A story of two billboards In 1995, the Calvin Klein clothing brand posed young teenagers in sexually suggestive clothing ads (left). A public uproar forced the company to remove the ads from magazines and billboards across the United States, but by then, a point had been made—that extreme thinness was in vogue for female fashion and, indeed, for females of all ages. In contrast, the Nolita clothing brand launched a major ad campaign against excessive thinness in 2007, displaying anti-anorexia billboards throughout Italy (right). Here two young women stare at one such billboard—that of an emaciated naked woman appearing beneath the words “No Anorexia.” The billboard model, Isabelle Caro, died in 2010 of complications from anorexia nervosa.
How Are Lasting Changes Achieved? Clinical researchers have found that people with anorexia nervosa must overcome their underlying psychological problems in order to create lasting improvement. Therapists typically use a combination of education, psychotherapy, and family therapy to help reach this broader goal (Knatz et al., 2015; Wade & Watson, 2012). Psychotropic drugs have also been helpful in some cases, but research has found that such medications are typically of limited benefit over the long-term course of anorexia nervosa (Starr & Kreipe, 2014).
COGNITIVE-BEHAVIORAL THERAPY A combination of behavioral and cognitive interventions is included in most treatment programs for anorexia nervosa. Such techniques are designed to help clients appreciate and change the behaviors and thought processes that help keep their restrictive eating going (Fairburn & Cooper, 2014; Evans & Waller, 2011). On the behavioral side, clients are typically required to monitor (perhaps by keeping a diary) their feelings, hunger levels, and food intake and the ties between these variables. On the cognitive side, they are taught to identify their “core pathology”—the deep-seated belief that they should in fact be judged by their shape and weight and by their ability to control these physical characteristics. The clients may also be taught alternative ways of coping with stress and of solving problems.
In 1968, the average fashion model was 8 percent thinner than the typical woman. Today, models are 23 percent thinner (Tashakova, 2011; Derenne & Beresin, 2006).
The therapists who use these approaches are particularly careful to help patients with anorexia nervosa recognize their need for independence and teach them more appropriate ways to exercise control (Pike et al., 2010). The therapists may also teach them to identify better and trust their internal sensations and feelings (Wilson, 2010). In the following session, a therapist tries to help a 15-year-old client recognize and share her feelings:
Calling for more assertive action According to many people, efforts to change the negative impact of the fashion industry and media on women have been woefully ineffective to date. Thus a feminist movement has emerged to more aggressively fight society’s “obsession with female thinness.” The movement’s slogan, “Riots Not Diets,” has already caught fire and now adorns bags, T-shirts, patches, cookies, glassware, and many other objects around the world.
| Patient: |
I don’t talk about my feelings; I never did. |
| Therapist: |
Do you think I’ll respond like others? |
| Patient: |
What do you mean? |
| Therapist: |
I think you may be afraid that I won’t pay close attention to what you feel inside, or that I’ll tell you not to feel the way you do—that it’s foolish to feel frightened, to feel fat, to doubt yourself, considering how well you do in school, how you’re appreciated by teachers, how pretty you are. |
| Patient: |
(Looking somewhat tense and agitated) Well, I was always told to be polite and respect other people, just like a stupid, faceless doll. (Affecting a vacant, doll-like pose) |
| Therapist: |
Do I give you the impression that it would be disrespectful for you to share your feelings, whatever they may be? |
| Patient: |
Not really; I don’t know. |
| Therapist: |
I can’t, and won’t, tell you that this is easy for you to do…. But I can promise you that you are free to speak your mind, and that I won’t turn away. |
(Strober & Yager, 1985, pp. 368–369)
Page 300
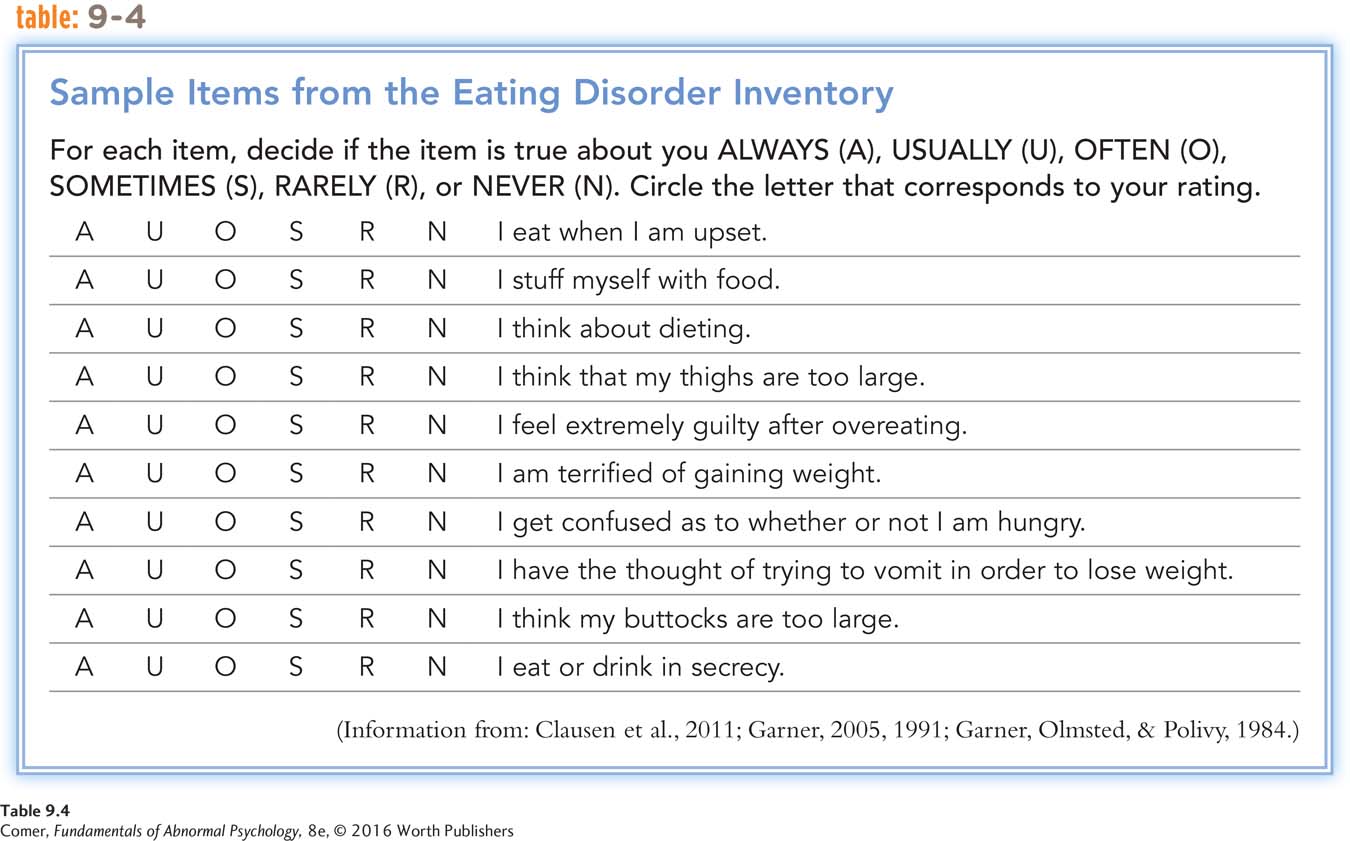
Finally, cognitive-behavioral therapists help clients with anorexia nervosa change their attitudes about eating and weight (Fairburn & Cooper, 2014; Evans & Waller, 2012) (see Table 9.4). The therapists may guide clients to identify, challenge, and change maladaptive assumptions, such as “I must always be perfect” or “My weight and shape determine my value” (Fairburn et al., 2015, 2008). They may also educate clients about the body distortions typical of anorexia nervosa and help them see that their own assessments of their size are incorrect.
Although cognitive-behavioral techniques are often of great help to clients with anorexia nervosa, research suggests that the techniques typically must be supplemented by other approaches to bring about better results (Zerbe, 2010, 2008). Family therapy, for example, is often included in treatment.
CHANGING FAMILY INTERACTIONS Family therapy can be an invaluable part of treatment for anorexia nervosa, particularly for children and adolescents with the disorder. As in other family therapy situations, the therapist meets with the family as a whole, points out troublesome family patterns, and helps the members make appropriate changes. In particular, family therapists may try to help the person with anorexia nervosa separate her feelings and needs from those of other members of her family. Although the role of family in the development of anorexia nervosa is not yet clear, research strongly suggests that family therapy (or at least parent counseling) can be helpful in the treatment of this disorder (Knatz et al., 2015; Ambresin et al., 2014).
Page 301
In 2015, the Oxford Dictionaries also added the word “fat-shame,” a verb meaning to humiliate someone by making mocking or critical comments about their overweight appearance.
| Mother: |
I think I know what [Susan] is going through: all the doubt and insecurity of growing up and establishing her own identity. (Turning to the patient, with tears) If you just place trust in yourself, with the support of those around you who care, everything will turn out for the better. |
| Therapist: |
Are you making yourself available to her? Should she turn to you, rely on you for guidance and emotional support? |
| Mother: |
Well, that’s what parents are for. |
| Therapist: |
(Turning to patient) What do you think? |
| Susan: |
(To mother) I can’t keep depending on you, Mom, or everyone else. That’s what I’ve been doing, and it gave me anorexia…. |
| Therapist: |
Do you think your mom would prefer that there be no secrets between her and the kids—an open door, so to speak? |
| Older sister: |
Sometimes I do. |
| Therapist: |
(To patient and younger sister) How about you two? |
| Susan: |
Yeah. Sometimes it’s like whatever I feel, she has to feel. |
| Younger sister: |
Yeah. |
(Strober & Yager, 1985, pp. 381–382)
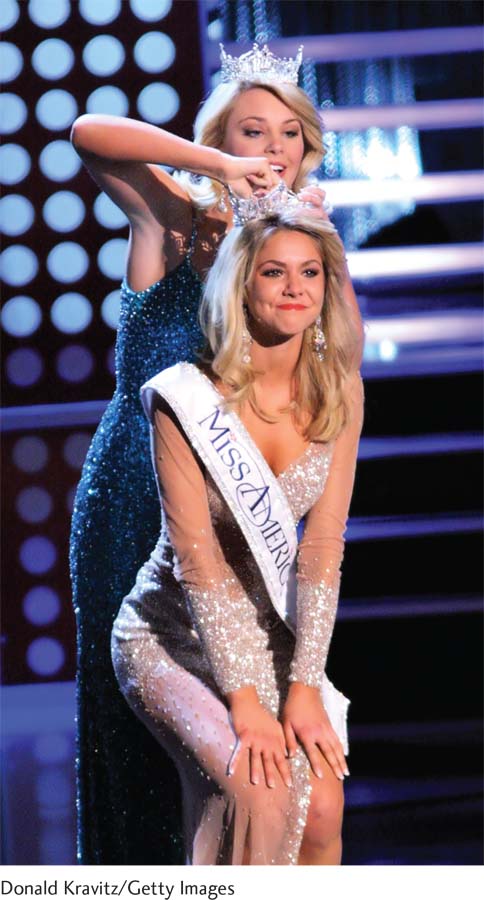
Miss America speaks out Kirsten Haglund is crowned Miss America at the January 2008 pageant. During her one-year reign, Haglund openly acknowledged her past struggles with anorexia nervosa. In recent years, she has continued to travel and speak about body image issues and eating disorders. She also has started a foundation to provide treatment services for women who have eating disorders.
What Is the Aftermath of Anorexia Nervosa? The use of combined treatment approaches has greatly improved the outlook for people with anorexia nervosa, although the road to recovery can be difficult. The course and outcome of this disorder vary from person to person, but researchers have noted certain trends.
On the positive side, weight is often quickly restored once treatment for the disorder begins, and treatment gains may continue for years (Isomaa & Isomaa, 2014; Haliburn, 2005). As many as 85 percent of patients continue to show improvement—either full or partial—when they are interviewed several years or more after their initial recovery (Isomaa & Isomaa, 2014; Brewerton & Costin, 2011).
Another positive note is that most females with anorexia nervosa menstruate again when they regain their weight, and other medical improvements follow (Mitchell & Crow, 2010). Also encouraging is that the death rate from anorexia nervosa seems to be falling (van Son et al., 2010). Earlier diagnosis and safer and faster weight-restoration techniques may account for this trend. Deaths that do occur are usually caused by suicide, starvation, infection, gastrointestinal problems, or electrolyte imbalance.
Page 302
Celebrities Who Acknowledge Having Had Eating Disorders
Nicole “Snooki” Polizzi, reality star
Alanis Morissette, singer
Lady Gaga, singer/songwriter
Paula Abdul, dancer/entertainer
Daniel Johns, rock singer (Silverchair)
Princess Diana, British royalty
Zina Garrison, tennis star
On the negative side, as many as 25 percent of persons with anorexia nervosa remain seriously troubled for years (Isomaa & Isomaa, 2014; Steinhausen, 2009). Furthermore, recovery, when it does occur, is not always permanent. At least one-third of recovered patients have recurrences of anorexic behavior, usually triggered by new stresses, such as marriage, pregnancy, or a major relocation (Stice et al., 2013; Fennig et al., 2002). Even years later, many who have recovered continue to express concerns about their weight and appearance. Some still restrict their diets to a degree, feel anxiety when they eat with other people, or hold some distorted ideas about food, eating, and weight (Isomaa & Isomaa, 2014; Fairburn et al., 2008).
About half of those who have suffered from anorexia nervosa continue to have certain emotional problems—particularly depression, obsessiveness, and social anxiety—years after treatment. Such problems are particularly common in those who had not reached a fully normal weight by the end of treatment (Bodell & Mayer, 2011; Steinhausen, 2002).
The more weight persons have lost and the more time that passes before they enter treatment, the poorer the recovery rate (Fairburn et al., 2008). People who had psychological or sexual problems before the onset of the disorder tend to have a poorer recovery rate than those without such a history (Zerwas et al., 2013; Amianto et al., 2011). People whose families are dysfunctional have less positive treatment outcomes (Holtom-Viesel & Allan, 2014). Teenagers seem to have a better recovery rate than older patients (Richard, 2005).
Treatments for Bulimia Nervosa
Treatment programs for bulimia nervosa are often offered in eating disorder clinics (Henderson et al., 2014). Such programs share the immediate goals of helping clients to eliminate their binge-purge patterns and establish good eating habits and the more general goal of eliminating the underlying causes of bulimic patterns. The programs emphasize education as much as therapy (Fairburn & Cooper, 2014). Cognitive-behavioral therapy is particularly helpful in cases of bulimia nervosa—perhaps even more helpful than in cases of anorexia nervosa (Fairburn & Cooper, 2014; Wonderlich et al., 2014). And antidepressant drug therapy, which is of limited help to people with anorexia nervosa, appears to be quite effective in many cases of bulimia nervosa (Starr & Kreipe, 2014).
Cognitive-Behavioral Therapy When treating clients with bulimia nervosa, cognitive-behavioral therapists employ many of the same techniques that they use to help treat people with anorexia nervosa. However, they tailor the techniques to the unique features of bulimia (for example, bingeing and purging behavior) and to the specific beliefs at work in bulimia nervosa.
BEHAVIORAL TECHNIQUES Therapists often instruct clients with bulimia nervosa to keep diaries of their eating behavior, changes in sensations of hunger and fullness, and the ebb and flow of other feelings (Stewart & Williamson, 2008). This helps the clients to observe their eating patterns more objectively and recognize the emotions and situations that trigger their desire to binge.
One team of researchers studied the effectiveness of an online version of the diary technique (Shapiro et al., 2010). They had 31 clients with bulimia nervosa, each an outpatient in a 12-week cognitive-behavioral therapy program, send nightly texts to their therapists, reporting on their bingeing and purging urges and episodes. The clients received feedback messages, including reinforcement and encouragement for the treatment goals they had been able to reach that day. The clinical researchers reported that by the end of therapy, the clients showed significant decreases in binges, purges, other bulimic symptoms, and feelings of depression.

New efforts at prevention A number of innovative educational programs have been developed to help promote healthy body images and prevent eating disorders. Here, a first-year Winona State University student swings a maul over her shoulder and into bathroom scales as part of Eating Disorders Awareness Week. The scale smashing is an annual event.
Cognitive-behavioral therapists may also use the behavioral technique of exposure and response prevention to help break the binge-purge cycle. As you read in Chapter 4, this approach consists of exposing people to situations that would ordinarily raise anxiety and then preventing them from performing their usual compulsive responses until they learn that the situations are actually harmless and their compulsive acts unnecessary. For bulimia nervosa, the therapists require clients to eat particular kinds and amounts of food and then prevent them from vomiting to show that eating can be a harmless and even constructive activity that needs no undoing (Wilson, 2010). Typically the therapist sits with the client while the client eats the forbidden foods and stays until the urge to purge has passed. Studies find that this treatment often helps reduce eating-related anxieties, bingeing, and vomiting.
Page 303
COGNITIVE TECHNIQUES Beyond such behavioral techniques, a primary focus of cognitive-behavioral therapists is to help clients with bulimia nervosa recognize and change their maladaptive attitudes toward food, eating, weight, and shape (Waller et al., 2014; Wonderlich et al., 2014). The therapists typically teach the clients to identify and challenge the negative thoughts that regularly precede their urge to binge—”I have no self-control”; “I might as well give up”; “I look fat” (Fairburn & Cooper, 2014; Fairburn, 1985). They may also guide clients to recognize, question, and eventually change their perfectionistic standards, sense of helplessness, and low self-concept (see PsychWatch below). Cognitive-behavioral approaches seem to help as many as 65 percent of patients stop bingeing and purging (Poulsen et al., 2014; Eifert et al., 2007).
Other Forms of Psychotherapy Because of its effectiveness in the treatment of bulimia nervosa, cognitive-behavioral therapy is often tried first, before other therapies are considered. If clients do not respond to it, other approaches with promising but less impressive track records may then be tried. A common alternative is interpersonal psychotherapy, the treatment described in Chapter 6 that is used to help improve interpersonal functioning (Fairburn et al., 2015; Kass et al., 2013). Psychodynamic therapy has also been used in cases of bulimia nervosa, but only a few research studies have tested and supported its effectiveness (Poulsen et al., 2014; Tasca et al., 2014). The various forms of psychotherapy—cognitive-behavioral, interpersonal, and psychodynamic—are often supplemented by family therapy (Ambresin et al., 2014; Starr & Kreipe, 2014).
Cognitive-behavioral, interpersonal, and psychodynamic therapy may each be offered in either an individual or a group therapy format, including self-help groups. Research suggests that group formats are at least somewhat helpful for as many as 75 percent of people with bulimia nervosa (Valbak, 2001).
“Girls should be encouraged to take an interest in their appearance when they are very young.”
Ladies’ Home Journal, 1940
Antidepressant Medications During the past 15 years, antidepressant drugs—all forms of antidepressant drugs—have been used to help treat bulimia nervosa (Starr & Kreipe, 2014). In contrast to people with anorexia nervosa, those with bulimia nervosa are often helped considerably by these drugs. According to research, the drugs help as many as 40 percent of patients, reducing their binges by an average of 67 percent and vomiting by 56 percent. Once again, drug therapy seems to work best in combination with other forms of therapy, particularly cognitive-behavioral therapy (Stewart & Williamson, 2008). Alternatively, some therapists wait to see whether cognitive-behavioral therapy or another form of psychotherapy is effective before trying antidepressants (Wilson, 2010, 2005).
Page 304

PsychWatch
Unfair critique Ballet dancer Jenifer Ringer performs with partner Jared Angle in The Nutcracker.
In a November 2010 review of the New York City Ballet production of The Nutcracker, New York Times critic Alastair Macauley wrote that Jenifer Ringer, the 37-year-old dancer who played the part of the Sugar Plum Fairy, “looked as if she’d eaten one sugar plum too many” (Macauley, 2010). That harsh critique of the dancer’s weight and body set off a storm of protest throughout the country. Many regarded the reviewer’s comments as cruel, an example of the absurd aesthetic standards by which women are judged in our society—even a lithe and graceful ballet artist. The reviewer defended his position, arguing, “If you want to make your appearance irrelevant to criticism, do not choose ballet as a career” (Macauley, 2010). But, in the eyes of most observers, he had gone too far.
About the only person who reacted calmly in the face of this uproar was the dancer herself, Jenifer Ringer. She even noted that “as a dancer, I do put myself out there to be criticized, and my body is part of my art form” (Ringer, 2010). It turns out that the 2010 flak was hardly the first time that Ringer’s weight and appearance had been described in unflattering terms. In a 2014 autobiography, she has revealed that her body had been an object of criticism throughout much of her professional life.
Ringer began with the City Ballet as a teenager in 1989, and by 1995 she was soloing. According to her memoir, she was also developing bulimia nervosa while her career was on the rise. She fell into a pattern of overeating and overexercising to compensate. As she puts it, “I had lost any sense of a center for self-esteem and self-worth” (Ringer, 2014).
Decades before Macauley’s 2010 critique, many of Ringer’s dance mentors were urging her to lose weight. She recalls how legendary choreographer Jerome Robbins exhorted her, “Come on. You just need to get the weight off. Just do it. We need you” (Ringer, 2014). In fact, after a warning from a ballet master that she must “stop eating cheesecake,” Ringer’s contract with the ballet company was not renewed in 1997 (Ringer, 2014). She left dance at that time for a brief stint as an office worker.
After overcoming her eating disorder and regaining her self-esteem, Ringer rejoined the City Ballet in 1998. The next 16 years of dance represented a personal and professional triumph for her—a triumph that those harsh and unfair words in 2010 could not penetrate. By then, she was no longer an insecure person who judged herself and her body by the standards of others. Rather, as she states in her memoir, “I didn’t feel I was heavy, and someone else’s opinion of me had no power over me unless I allowed it” (Ringer, 2014).
What Is the Aftermath of Bulimia Nervosa? Left untreated, bulimia nervosa can last for years, sometimes improving temporarily but then returning. Treatment, however, produces immediate, significant improvement in approximately 40 percent of clients: they stop or greatly reduce their bingeing and purging, eat properly, and maintain a normal weight (Isomaa & Isomaa, 2014; Richard, 2005). Another 40 percent show a moderate response—at least some decrease in binge eating and purging. As many as 20 percent show little immediate improvement. Follow-up studies, conducted years after treatment, suggest that as many as 85 percent of people with bulimia nervosa have recovered, either fully or partially (Isomaa & Isomaa, 2014; Brewerton & Costin, 2011).
Page 305
Why do some people who recover from anorexia nervosa and bulimia nervosa remain vulnerable to relapse after recovery?
Relapse can be a problem even among people who respond successfully to treatment (Stice et al., 2013; Olmsted et al., 2005). As with anorexia nervosa, relapses are usually triggered by a new life stress (Liu, 2007; Abraham & Llewellyn-Jones, 1984). One study found that close to one-third of those who had recovered from bulimia nervosa relapsed within two years of treatment, usually within six months (Olmsted et al., 1994). Relapse is more likely among people who had longer histories of bulimia nervosa before treatment, had vomited more frequently during their disorder, continued to vomit at the end of treatment, had histories of substance abuse, and continue to be lonely or to distrust others after treatment (Vall & Wade, 2015; Brewerton & Costin, 2011; Fairburn et al., 2004).
Treatments for Binge-Eating Disorder

The Biggest Loser phenomenon Contestant Hannah Curlee proudly observes the results of her weigh-in on the 2011 season finale of the popular reality show The Biggest Loser. In this TV series, overweight contestants compete to lose the most weight for cash prizes. Most overweight people do not display binge-eating disorder, but most people with the disorder are overweight.
Given the key role of binges in both bulimia nervosa and binge-eating disorder (bingeing without purging), today’s treatments for binge-eating disorder are often similar to those for bulimia nervosa. In particular, cognitive-behavioral therapy, other forms of psychotherapy, and antidepressant medications have been provided—with some success—to help reduce or eliminate the binge-eating patterns and to change disturbed thinking such as being overly concerned with weight and shape (Fischer et al., 2014; Fairburn, 2013). Of course, many people with binge-eating disorder also are overweight, a problem that requires additional kinds of intervention and is often resistant to long-term improvement (Grilo et al., 2014; Claudino & Morgan, 2012).
Now that binge-eating disorder has been identified and is receiving considerable study, it is likely that specialized treatment programs that target the disorder’s unique issues will emerge in the coming years (Grilo et al., 2014). In the meantime, relatively little is known about the aftermath of this disorder (Claudino & Morgan, 2012). In one follow-up study of hospitalized patients with severe symptoms, one-third of those who had been treated still displayed the disorder 12 years after hospitalization, and 36 percent were still significantly overweight (Fichter et al., 2008). As with the other eating disorders, many of those who initially recover from binge-eating disorder continue to have a relatively high risk of relapse (ANAD, 2014).
Summing Up
HOW ARE EATING DISORDERS TREATED? The first step in treating anorexia nervosa is to increase calorie intake and quickly restore the person’s weight, using a strategy such as supportive nursing care. The second step is to deal with the underlying psychological and family problems, often using a combination of education, cognitive-behavioral approaches, and family therapy. As many as 90 percent of people who are successfully treated for anorexia nervosa continue to show full or partial improvements years later. However, some of them relapse along the way.
Treatments for bulimia nervosa focus first on stopping the binge-purge pattern and then on addressing the underlying causes of the disorder. Often several treatment strategies are combined, including education, psychotherapy (particularly cognitive-behavioral therapy), and antidepressant medications. As many as 75 percent of those who receive treatment eventually improve either fully or partially. Relapse can be a problem and may be precipitated by a new stress. Similar treatments are used to help people with binge-eating disorder. These individuals, however, may also require interventions to address their excessive weight.