10.1 Depressants
Depressants slow the activity of the central nervous system. They reduce tension and inhibitions and may interfere with a person’s judgment, motor activity, and concentration. The three most widely used groups of depressants are alcohol, sedative-
Alcohol
alcohol Any beverage containing ethyl alcohol, including beer, wine, and liquor.
The World Health Organization estimates that 2 billion people worldwide consume alcohol. In the United States more than half of all residents at least from time to time drink beverages that contain alcohol (SAMHSA, 2014). Purchases of beer, wine, and liquor amount to tens of billions of dollars each year in the United States alone.
When people consume five or more drinks on a single occasion, it is called a binge-
All alcoholic beverages contain ethyl alcohol, a chemical that is quickly absorbed into the blood through the lining of the stomach and the intestine. The ethyl alcohol immediately begins to take effect as it is carried in the bloodstream to the central nervous system (the brain and spinal cord), where it acts to depress, or slow, functioning by binding to various neurons. One important group of neurons to which ethyl alcohol binds are those that normally receive the neurotransmitter GABA. As you saw in Chapter 4, GABA carries an inhibitory message—

At first ethyl alcohol depresses the areas of the brain that control judgment and inhibition; people become looser, more talkative, and often more friendly. As their inner control breaks down, they may feel relaxed, confident, and happy. When more alcohol is absorbed, it slows down additional areas in the central nervous system, leaving drinkers less able to make sound judgments, their speech less careful and less coherent, and their memory weaker. Many people become highly emotional and perhaps loud and aggressive.
Motor difficulties increase as a person continues drinking, and reaction times slow. People may be unsteady when they stand or walk and clumsy in performing even simple activities. They may drop things, bump into doors and furniture, and misjudge distances. Their vision becomes blurred, particularly their peripheral, or side, vision, and they have trouble hearing. As a result, people who have drunk too much alcohol may have great difficulty driving or solving simple problems.
The extent of the effect of ethyl alcohol is determined by its concentration, or proportion, in the blood. Thus a given amount of alcohol has less effect on a large person than on a small one. Gender also affects the concentration of alcohol in the blood. Women have less of the stomach enzyme alcohol dehydrogenase, which breaks down alcohol in the stomach before it enters the blood. So women become more intoxicated than men on equal doses of alcohol (Hart & Ksir, 2014).
Levels of impairment are closely related to the concentration of ethyl alcohol in the blood. When the alcohol concentration reaches 0.06 percent of the blood volume, a person usually feels relaxed and comfortable. By the time it reaches 0.09 percent, however, the drinker crosses the line into intoxication. If the level goes as high as 0.55 percent, the drinker will likely die. Most people lose consciousness before they can drink enough to reach this level; nevertheless, more than 1,000 people in the United States die each year from too high a blood alcohol level (Hart & Ksir, 2014).
The effects of alcohol subside only when the alcohol concentration in the blood declines. Most of the alcohol is broken down, or metabolized, by the liver into carbon dioxide and water, which can be exhaled and excreted. The average rate of this metabolism is 25 percent of an ounce per hour, but different people’s livers work at different speeds; thus rates of “sobering up” vary. Despite popular belief, only time and metabolism can make a person sober. Drinking black coffee, splashing cold water on one’s face, or “pulling oneself together” cannot hurry the process.
If alcohol is highly addictive and capable of causing so many problems, why does it remain legal in most countries?
Alcohol Use Disorder Though legal, alcohol is actually one of the most dangerous of recreational drugs, and its reach extends across the life span. In fact, around 28 percent of middle school students admit to some alcohol use, while 39 percent of high school seniors drink alcohol each month (most to the point of intoxication) and 2.2 percent report drinking every day (Johnston et al., 2014). Alcohol misuse is also a major problem on college campuses (see PsychWatch below).
Surveys indicate that over a one-

PsychWatch
College Binge Drinking: An Extracurricular Crisis
Drinking large amounts of alcohol in a short time, or binge drinking, is a serious problem on college campuses, as well as in many other settings (SAMHSA, 2014; NSDUH, 2013). Studies show that 40 percent of college students binge-
Alcohol-
related arrests account for 83 percent of all campus arrests. More than half of all sexual assaults on college campuses involve the heavy consumption of alcohol.
Alcohol may be a factor in nearly 40 percent of academic problems and 28 percent of all instances of dropping out of college.
Approximately 700,000 students each year are physically or emotionally traumatized or assaulted by a student drinker.
Half of college students say “drinking to get drunk” is an important reason for drinking.
Binge drinking often has a lingering effect on mood, memory, brain functioning, and heart functioning.
Binge drinking is tied to 1,700 deaths and 500,000 injuries, every year.
The number of female binge drinkers among college students has increased 31 percent over the past decade.
These findings have led some educators to describe binge drinking as “the number one public health hazard” for full-
Efforts to change such patterns have begun. For example, some universities now provide substance-
The current prevalence of alcoholism is around 7.6 percent for white Americans, 5.1 percent for Hispanic Americans, and 4.5 percent for African Americans (NSDUH, 2013). American Indians, particularly men, tend to display a higher rate of alcohol use disorder than any of these groups. Overall, 8.5 percent of them experience the disorder, although specific prevalence rates differ widely across the various American Indian reservation communities. Generally, Asians in the United States and elsewhere have a lower rate of alcoholism (1.7 percent) than do people from other cultures. As many as half of these individuals have a deficiency of alcohol dehydrogenase, the chemical responsible for breaking down alcohol, so they react quite negatively to even a modest intake of alcohol. Such reactions in turn help prevent extended use (Tsuang & Pi, 2011).
BETWEEN THE LINES
DSM-
DSM-
CLINICAL PICTURE Generally speaking, people with alcohol use disorder drink large amounts regularly and rely on it to enable them to do things that would otherwise make them anxious (McCrady, 2014). Eventually the drinking interferes with their social behavior and ability to think and work. They may have frequent arguments with family members or friends, miss work repeatedly, and even lose their jobs. MRI scans of chronic heavy drinkers have revealed damage in various regions of their brains and, correspondingly, impairments in their memory, speed of thinking, attention skills, and balance (Sifferlin, 2014).
Individually, people’s patterns of alcoholism vary. Some drink large amounts of alcohol every day and keep drinking until intoxicated. Others go on periodic binges of heavy drinking that can last weeks or months. They may remain intoxicated for days and later be unable to remember anything about the period. Still others may limit their excessive drinking to weekends, evenings, or both.
TOLERANCE AND WITHDRAWAL For many people, alcohol use disorder includes the symptoms of tolerance and withdrawal reactions (McCrady, 2014). As their bodies build up a tolerance for alcohol, they need to drink ever larger amounts to feel its effects. In addition, they have withdrawal symptoms when they stop drinking. Within hours their hands, tongue, and eyelids begin to shake; they feel weak and nauseated; they sweat and vomit; their heart beats rapidly; and their blood pressure rises. They may also become anxious, depressed, unable to sleep, or irritable (APA, 2013).
delirium tremens (DTs) A dramatic withdrawal reaction that some people who are dependent on alcohol have. It consists of confusion, clouded consciousness, and terrifying visual hallucinations.
A small percentage of people with alcohol use disorder go through a particularly dramatic withdrawal reaction called delirium tremens (“the DTs”). It consists of terrifying visual hallucinations that begin within a few days after they stop or reduce their drinking. Some people see small, frightening animals chasing or crawling on them or objects dancing about in front of their eyes. Like most other alcohol withdrawal symptoms, the DTs usually run their course in two to three days. However, people who have severe withdrawal reactions such as this may also have seizures, lose consciousness, suffer a stroke, or even die. Today certain medical procedures can help prevent or reduce such extreme reactions.

What Is the Personal and Social Impact of Alcoholism? Alcoholism destroys millions of families, social relationships, and careers (see MindTech below). Medical treatment, lost productivity, and losses due to deaths from alcoholism cost society many billions of dollars annually. The disorder also plays a role in more than one-
Alcoholism has serious effects on the 30 million children of people with this disorder. Home life for these children is likely to include much conflict and perhaps sexual or other forms of abuse. In turn, the children themselves have higher rates of psychological problems (Kelley et al., 2014; Watt, 2002). Many have low self-
Long-
MindTech
 Neknomination Goes Viral
Neknomination Goes Viral
Binge drinking and other risky alcohol-

In early 2013, an online drinking game called Neknominate (or Neknomination), believed to have originated in Australia, emerged on Internet sites like YouTube and Facebook (Wilkinson and Soares, 2014). In this game, a person records a video of himself or herself drinking an entire bottle of hard liquor (known in Australia as “necking”) and then challenges (“nominates”) a friend by name to post his or her own drinking video, one that will top the level and danger of the initial drinking act, and to then pass the challenge on to another person (James, 2014).
In most cases, the drink being consumed in the videos has an unusually high alcohol content, to make the “achievement” all the more “impressive.” Some of the videos also involve people exhibiting other dangerous or reckless behavior along with the drinking, such as driving while drinking, stripping in public, shoplifting, or consuming motor oil or even small animals both alive and dead (Wilkinson and Soares, 2014).
What psychological factors, besides peer pressure, might induce a person to participate in an activity as risky as Neknominate?
Given the nature of the game, you may not be surprised that Neknominate was tied with a number of deaths within a very short period after its emergence, as it spread to Great Britain, Canada, the United States, and other parts of the world (James, 2014). In February 2014, for example, five unrelated men, three in England and two in Ireland, died while making videos of themselves completing Neknominate challenges.
A public outcry regarding the practice of Neknominate has emerged, with politicians, doctors, and others calling on Facebook and You Tube to ban discussions or presentations of the game. Facebook, however, has declined to ban discussions or postings associated with it, stating that its policy is only to ban content that is directly harmful, not to censor content that discusses potentially dangerous or offensive behavior (Wilkinson and Soares, 2014). The practice and uproar surrounding Neknominate has begun to die down a bit in recent months—
Korsakoff’s syndrome An alcohol-
Long-
fetal alcohol syndrome A cluster of problems in a child, including low birth weight, irregularities in the head and face, and intellectual deficits, caused by excessive alcohol intake by the mother during pregnancy.
Women who drink during pregnancy place their fetuses at risk (Bakoyiannis et al., 2014; Hart & Ksir, 2014; Gifford et al., 2010). Excessive alcohol use during pregnancy may cause a baby to be born with fetal alcohol syndrome, a pattern of abnormalities that can include intellectual disability disorder, hyperactivity, head and face deformities, heart defects, and slow growth. It has been estimated that in the overall population, around 1 of every 1,000 babies is born with this syndrome. The rate may increase to as many as 29 of every 1,000 babies of women who are problem drinkers. If all alcohol-
Sedative-Hypnotic Drugs
sedative-
barbiturates Addictive sedative-
benzodiazepines The most common group of sedative-
Sedative-
As Chapter 4 noted, benzodiazepines, developed in the 1950s, are the most popular sedative-
When benzodiazepines were first discovered, they seemed so safe and effective that physicians prescribed them generously, and their use spread. Eventually, however, it became clear that in high enough doses the drugs can, like barbiturates, cause intoxication and lead to sedative-
Opioids
opioid Opium or any of the drugs derived from opium, including morphine, heroin, and codeine.
opium A highly addictive substance made from the sap of the opium poppy.
Opioids include opium—
morphine A highly addictive substance derived from opium that is particularly effective in relieving pain.

In 1804 a new substance, morphine, was derived from opium. Named after Morpheus, the Greek god of sleep, this drug relieved pain even better than opium did and initially was considered safe. However, wide use of the drug eventually revealed that it, too, could lead to addiction. So many wounded soldiers in the United States received morphine injections during the Civil War that morphine addiction became known as “soldiers’ disease.”
heroin One of the most addictive substances derived from opium.
In 1898, morphine was converted into yet another new pain reliever, heroin. For several years heroin was viewed as a wonder drug and was used as a cough medicine and for other medical purposes. Eventually, however, physicians learned that heroin is even more addictive than the other opioids. By 1917, the U.S. Congress had concluded that all drugs derived from opium were addictive, and it passed a law making opioids illegal except for medical purposes.
Still other drugs have been derived from opium, and synthetic (laboratory-
Can you think of other substances or activities that, like opioids, can be helpful in controlled portions but dangerous when used excessively?
Most narcotics are smoked, inhaled, snorted, injected by needle just beneath the skin (“skin popped”), or injected directly into the bloodstream (“mainlined”), the most powerful form of intake. An injection quickly brings on a rush—a spasm of warmth and ecstasy that is sometimes compared with orgasm. The brief spasm is followed by several hours of a pleasant feeling called a high or nod. During a high, the drug user feels relaxed, happy, and unconcerned about food, sex, or other bodily needs.
endorphins Neurotransmitters that help relieve pain and reduce emotional tension. They are sometimes referred to as the body’s own opioids.
Opioids create these effects by depressing the central nervous system, particularly the centers that help control emotion. The drugs attach to brain receptor sites that ordinarily receive endorphins—neurotransmitters that help relieve pain and reduce emotional tension. When neurons at these receptor sites receive opioids, they produce pleasurable and calming feelings just as they would do if they were receiving endorphins. In addition to reducing pain and tension, opioids cause nausea, narrowing of the pupils (“pinpoint pupils”), and constipation.

Opioid Use Disorder Heroin use exemplifies the kinds of problems posed by opioids. After taking heroin repeatedly for just a few weeks, users may develop opioid use disorder. Their use of heroin interferes significantly with their social and occupational functioning, and their lives center around the drug. They may also build a tolerance for heroin and experience a withdrawal reaction when they stop taking it (Hart & Ksir, 2014). At first the withdrawal symptoms are anxiety, restlessness, sweating, and rapid breathing; later they include severe twitching, aches, fever, vomiting, diarrhea, loss of appetite, high blood pressure, and weight loss of up to 15 pounds (due to loss of bodily fluids). These symptoms usually peak by the third day, gradually subside, and disappear by the eighth day. A person in heroin withdrawal can either wait out the symptoms or end withdrawal by taking the drug again.
Such people soon need heroin just to avoid going into withdrawal, and they must continually increase their doses in order to achieve even that relief. The temporary high becomes less intense and less important. Heroin users may spend much of their time planning their next dose, in many cases turning to criminal activities, such as theft and prostitution, to support the expensive “habit” (Cadet et al., 2014; Koetzle, 2014).
Surveys suggest that more than 1 percent of adults in the United States display an opioid use disorder within a given year (SAMHSA, 2014; NSDUH, 2013). Most of these persons (80 percent) are addicted to the pain-
What Are the Dangers of Opioid Use? Once again, heroin provides a good example of the dangers of opioid use. The most immediate danger of heroin use is an overdose, which closes down the respiratory center in the brain, almost paralyzing breathing and in many cases causing death (Christensen, 2014). Death is particularly likely during sleep, when a person is unable to fight this effect by consciously working to breathe. People who resume heroin use after having avoided it for some time often make the fatal mistake of taking the same dose they had built up to before. Because their bodies have been without heroin for some time, however, they can no longer tolerate this high level (Gray, 2014). Each year approximately 2 percent of those addicted to heroin and other opioids die under the drug’s influence, usually from an overdose.
Heroin users run other risks as well. Drug dealers often mix heroin with a cheaper drug or even a deadly substance such as cyanide or battery acid. In addition, dirty needles and other unsterilized equipment spread infections such as AIDS, hepatitis C, and skin abscesses (NIDA, 2014; Dilts & Dilts, 2011). In some areas of the United States, the HIV infection rate among active heroin users is reported to be as high as 60 percent.
BETWEEN THE LINES
Nonmedical Use of Pain Relievers
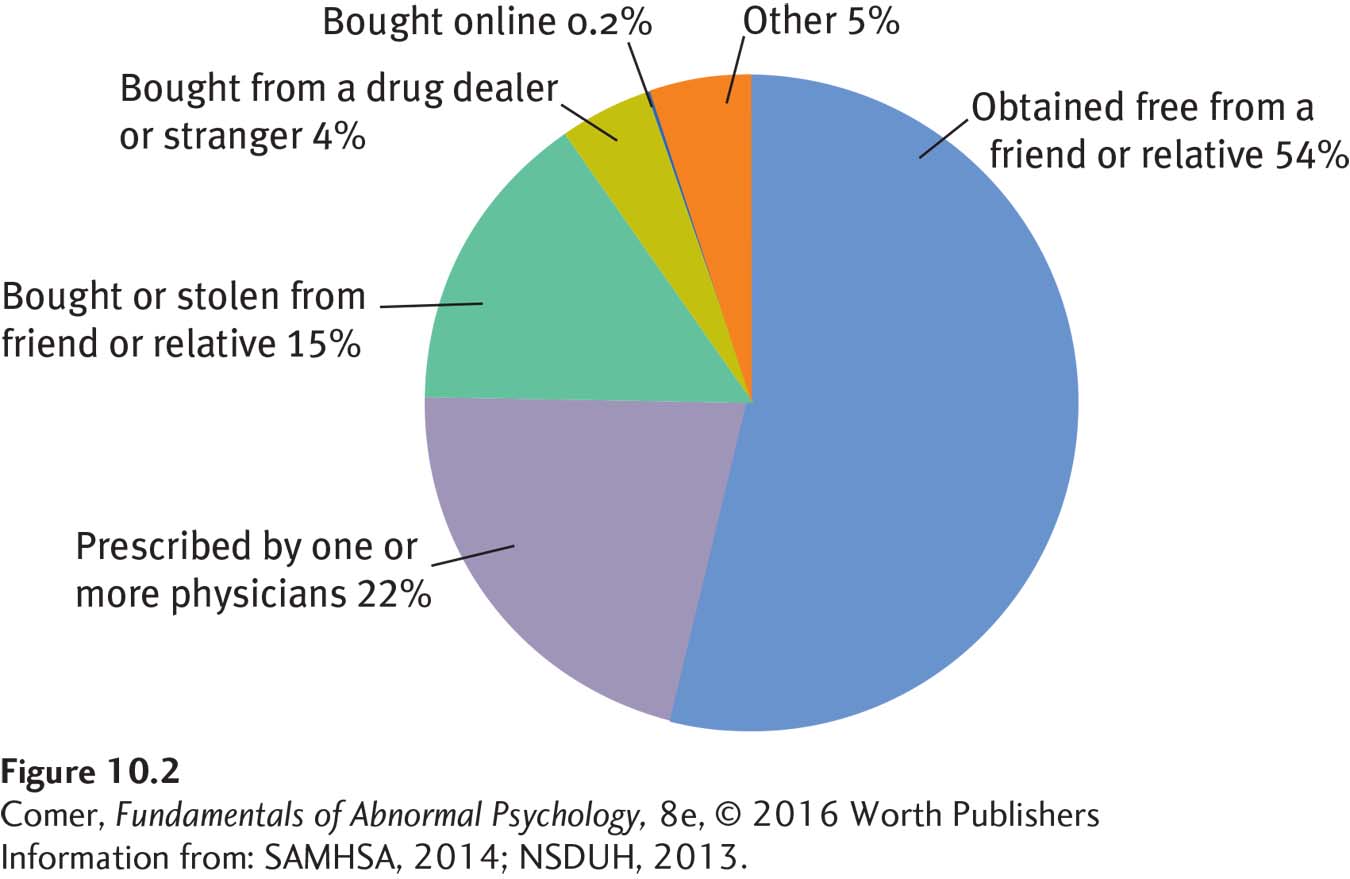
In the United States, the largest increase in illicit drug use during the past few years has been the nonmedical use of medications, mostly pain relievers (SAMHSA, 2014).
Summing Up
SUBSTANCE MISUSE AND DEPRESSANTS Repeated and excessive use of certain substances (or drugs) can lead to substance use disorders. Many people with such disorders also develop a tolerance for the substance in question and/or have unpleasant withdrawal symptoms when they abstain from it.
Depressants are substances that slow the activity of the central nervous system. Repeated and excessive use of these substances can lead to problems such as alcohol use disorder, sedative-