15.1 Introduction to Therapy and the Psychological Therapies
The long history of efforts to treat psychological disorders has included a bewildering mix of methods, harsh and gentle. Well-
Reformers Philippe Pinel (1745–
Treating Psychological Disorders

15-
Modern Western therapies can be classified into two main categories.
psychotherapy treatment involving psychological techniques; consists of interactions between a trained therapist and someone seeking to overcome psychological difficulties or achieve personal growth.
biomedical therapy prescribed medications or procedures that act directly on the person’s physiology.
In psychotherapy, a trained therapist uses psychological techniques to assist someone seeking to overcome difficulties or achieve personal growth. The therapist may explore a client’s early relationships, encourage the client to adopt new ways of thinking, or coach the client in replacing old behaviors with new ones.
Biomedical therapy offers medication or other biological treatments. For example, a person with severe depression may receive antidepressants, electroconvulsive shock therapy (ECT), or deep brain stimulation.
The care provider’s training and expertise, as well as the disorder itself, influence the choice of treatment. Psychotherapy and medication are often combined. Kay Redfield Jamison received psychotherapy in her meetings with her psychiatrist, and she took medications to control her wild mood swings.
eclectic approach an approach to psychotherapy that uses techniques from various forms of therapy.
Let’s look first at the psychotherapy options for those treated with “talk therapies.” Each is built on one or more of psychology’s major theories: psychodynamic, humanistic, behavioral, and cognitive. Most of these techniques can be used one-
Psychoanalysis and Psychodynamic Therapies
15-
psychoanalysis Sigmund Freud’s therapeutic technique. Freud believed the patient’s free associations, resistances, dreams, and transferences—
The first major psychological therapy was Sigmund Freud’s psychoanalysis. Although few clinicians today practice therapy as Freud did, his work deserves discussion. It helped form the foundation for treating psychological disorders, and it continues to influence modern therapists working from the psychodynamic perspective.

The Goals of Psychoanalysis
Freud believed that in therapy, people could achieve healthier, less anxious living by releasing the energy they had previously devoted to id-
Freud’s therapy aimed to bring patients’ repressed or disowned feelings into conscious awareness. By helping them reclaim their unconscious thoughts and feelings, and by giving them insight into the origins of their disorders, he aimed to help them reduce growth-
The Techniques of Psychoanalysis
Psychoanalysis is historical reconstruction. Psychoanalytic theory emphasizes the power of childhood experiences to mold the adult. Thus, it aims to unearth the past in the hope of loosening its bonds on the present. After discarding hypnosis as an unreliable excavator, Freud turned to free association.
Imagine yourself as a patient using free association. You begin by relaxing, perhaps by lying on a couch. As the psychoanalyst sits out of your line of vision, you say aloud whatever comes to mind. At one moment, you’re relating a childhood memory. At another, you’re describing a dream or recent experience. It sounds easy, but soon you may notice how often you edit your thoughts as you speak. You pause for a second before uttering an embarrassing thought. You omit what seems trivial, irrelevant, or shameful. Sometimes your mind goes blank or you clutch up, unable to remember important details. You may joke or change the subject to something less threatening.
resistance in psychoanalysis, the blocking from consciousness of anxiety-
interpretation in psychoanalysis, the analyst’s noting supposed dream meanings, resistances, and other significant behaviors and events in order to promote insight.
To the analyst, these mental blocks indicate resistance. They hint that anxiety lurks and you are defending against sensitive material. The analyst will note your resistances and then provide insight into their meaning. If offered at the right moment, this interpretation—of, say, your not wanting to talk about your mother—
transference in psychoanalysis, the patient’s transfer to the analyst of emotions linked with other relationships (such as love or hatred for a parent).
Over many such sessions, your relationship patterns surface in your interactions with your therapist. You may find yourself experiencing strong positive or negative feelings for your analyst. The analyst may suggest you are transferring feelings, such as feelings of dependency or mingled love and anger, that you experienced in earlier relationships with family members or other important people. By exposing such feelings, you may gain insight into your current relationships.
Relatively few North American therapists now offer traditional psychoanalysis. Much of its underlying theory is not supported by scientific research (Chapter 13). Analysts’ interpretations do not follow the scientific method—
RETRIEVE IT
Question
In psychoanalysis, when patients experience strong feelings for their therapist, this is called . Patients are said to demonstrate anxiety when they put up mental blocks around sensitive memories, indicating . The therapist will attempt to provide insight into the underlying anxiety by offering a(n) of the mental blocks.
“I haven’t seen my analyst in 200 years. He was a strict Freudian. If I’d been going all this time, I’d probably almost be cured by now.”
Woody Allen, after awakening from suspended animation in the movie Sleeper
Psychodynamic Therapy
psychodynamic therapy therapy deriving from the psychoanalytic tradition; views individuals as responding to unconscious forces and childhood experiences, and seeks to enhance self-
Although influenced by Freud’s ideas, psychodynamic therapists don’t talk much about id, ego, and superego. Instead, they try to help people understand their current symptoms by focusing on themes across important relationships, including childhood experiences and the therapist relationship. “We can have loving feelings and hateful feelings toward the same person,” notes psychodynamic therapist Jonathan Shedler (2009), and “we can desire something and also fear it.” Client-

Therapist David Shapiro (1999, p. 8) illustrates this method with the case of a young man who had told women that he loved them, when he knew that he didn’t. His explanation: They expected it, so he said it. But with his wife, who wished he would say that he loved her, he found he couldn’t do that—
Therapist: Do you mean, then, that if you could, you would like to?
Patient: Well, I don’t know…. Maybe I can’t say it because I’m not sure it’s true. Maybe I don’t love her.
Further interactions revealed that he could not express real love because it would feel “mushy” and “soft” and therefore unmanly. Shapiro noted that this young man was “in conflict with himself, and he [was] cut off from the nature of that conflict.” With such patients, who are estranged from themselves, therapists using psychodynamic techniques “are in a position to introduce them to themselves. We can restore their awareness of their own wishes and feelings, and their awareness, as well, of their reactions against those wishes and feelings.”
Exploring past relationship troubles may help clients understand the origin of their current difficulties. Jonathan Shedler (2010) recalled his patient “Jeffrey’s” complaints of difficulty getting along with his colleagues and wife, who saw him as hypercritical. Jeffrey then “began responding to me as if I were an unpredictable, angry adversary.” Shedler seized this opportunity to help Jeffrey recognize the relationship pattern, and its roots in the attacks and humiliation he experienced from his alcohol-
Humanistic Therapies
15-
insight therapies a variety of therapies that aim to improve psychological functioning by increasing a person’s awareness of underlying motives and defenses.
The humanistic perspective (Chapter 13) emphasizes people’s inherent potential for self-
Humanistic therapists aim to boost people’s self-
fulfillment by helping them grow in self- awareness and self- acceptance. Promoting this growth, not curing illness, is the therapy focus. Thus, those in therapy became “clients” or just “persons” rather than “patients” (a change many other therapists have adopted).
The path to growth is taking immediate responsibility for one’s feelings and actions, rather than uncovering hidden causes.
Conscious thoughts are more important than the unconscious.
The present and future are more important than the past. Therapy thus focuses on exploring feelings as they occur, rather than achieving insight into the childhood origins of those feelings.
client-centered therapy a humanistic therapy, developed by Carl Rogers, in which the therapist uses techniques such as active listening within a genuine, accepting, empathic environment to facilitate clients’ growth. (Also called person-
All these themes are present in the widely used humanistic technique that Carl Rogers (1902-
Believing that most people possess the resources for growth, Rogers (1961, 1980) encouraged therapists to foster that growth by exhibiting genuineness, acceptance, and empathy. By being genuine, therapists hope to encourage clients to likewise express their true feelings. By being accepting, therapists may help clients feel freer and more open to change. By showing empathy—
Hearing has consequences. When I truly hear a person and the meanings that are important to him at that moment, hearing not simply his words, but him, and when I let him know that I have heard his own private personal meanings, many things happen. There is first of all a grateful look. He feels released. He wants to tell me more about his world. He surges forth in a new sense of freedom. He becomes more open to the process of change.
I have often noticed that the more deeply I hear the meanings of the person, the more there is that happens. Almost always, when a person realizes he has been deeply heard, his eyes moisten. I think in some real sense he is weeping for joy. It is as though he were saying, “Thank God, somebody heard me. Someone knows what it’s like to be me.”
active listening empathic listening in which the listener echoes, restates, and clarifies. A feature of Rogers’ client-
“We have two ears and one mouth that we may listen the more and talk the less.”
Zeno, 335–
To Rogers, “hearing” was active listening. The therapist echoes, restates, and clarifies what the client has expressed verbally or nonverbally. The therapist also acknowledges those expressed feelings. Active listening is now an accepted part of counseling practices in many schools, colleges, and clinics. Counselors listen attentively. They interrupt only to restate and confirm feelings, to accept what was said, or to check their understanding of something. In the following brief excerpt, note how Rogers tried to provide a psychological mirror that would help the client see himself more clearly:
Rogers: Feeling that now, hm? That you’re just no good to yourself, no good to anybody. Never will be any good to anybody. Just that you’re completely worthless, huh?—Those really are lousy feelings. Just feel that you’re no good at all, hm?
Client: Yeah. (Muttering in low, discouraged voice) That’s what this guy I went to town with just the other day told me.
Rogers: This guy that you went to town with really told you that you were no good? Is that what you’re saying? Did I get that right?
Client: M-
Rogers: I guess the meaning of that if I get it right is that here’s somebody that meant something to you and what does he think of you? Why, he’s told you that he thinks you’re no good at all. And that just really knocks the props out from under you. (Client weeps quietly.) It just brings the tears. (Silence of 20 seconds)
Client: (Rather defiantly) I don’t care though.
Rogers: You tell yourself you don’t care at all, but somehow I guess some part of you cares because some part of you weeps over it.
(Meador & Rogers, 1984, p. 167)

unconditional positive regard a caring, accepting, nonjudgmental attitude, which Carl Rogers believed would help clients develop self-
Can a therapist be a perfect mirror, critics have asked, without selecting and interpreting what is reflected? Rogers conceded that no one can be totally nondirective. Nevertheless, he said, the therapist’s most important contribution is to accept and understand the client. Given a nonjudgmental, grace-
How can we improve communication in our own relationships by listening more actively? Three Rogers-
Paraphrase. Rather than saying “I know how you feel,” check your understandings by summarizing the person’s words in your own words.
Invite clarification. “What might be an example of that?” may encourage the person to say more.
Reflect feelings. “It sounds frustrating” might mirror what you’re sensing from the person’s body language and intensity.
Behavior Therapies
15-
behavior therapy therapy that applies learning principles to the elimination of unwanted behaviors.
The insight therapies assume that self-

Classical Conditioning Techniques
One cluster of behavior therapies derives from principles developed in Ivan Pavlov’s conditioning experiments (Chapter 7). As Pavlov and others showed, we learn various behaviors and emotions through classical conditioning. If we’re attacked by a dog, we may thereafter have a conditioned fear response when other dogs approach: Our fear generalizes and all dogs become conditioned stimuli.
Could maladaptive symptoms be examples of conditioned responses? If so, might reconditioning be a solution? Learning theorist O. H. Mowrer thought so. He developed a successful conditioning therapy for chronic bed-
counterconditioning behavior therapy procedures that use classical conditioning to evoke new responses to stimuli that are triggering unwanted behaviors; include exposure therapies and aversive conditioning.
Can we unlearn fear responses through new conditioning? Many people have. One example: The fear of riding in an elevator is often a learned fear response to being in a confined space. Counterconditioning pairs the trigger stimulus (in this case, the enclosed space of the elevator) with a new response (relaxation) that is incompatible with fear. Two specific counterconditioning techniques—
RETRIEVE IT
Question
What might a psychodynamic therapist say about Mowrer's therapy for bed-
EXPOSURE THERAPIES Picture this scene: Behavioral psychologist Mary Cover Jones is working with 3-
exposure therapies behavioral techniques, such as systematic desensitization and virtual reality exposure therapy, that treat anxieties by exposing people (in imagination or actual situations) to the things they fear and avoid.
Unfortunately for many who might have been helped by Jones’ procedures, her story of Peter and the rabbit did not enter psychology’s lore when it was reported in 1924. It was more than 30 years before psychiatrist Joseph Wolpe (1958; Wolpe & Plaud, 1997) refined Jones’ counterconditioning technique into the exposure therapies used today. These therapies, in a variety of ways, try to change people’s reactions by repeatedly exposing them to stimuli that trigger unwanted reactions. With repeated exposure to what they normally avoid or escape, people adapt. We all experience this process in everyday life. A person moving to a new apartment may be annoyed by nearby loud traffic noise, but only for a while. With repeated exposure, the person adapts. So, too, with people who have fear reactions to specific events. Exposed repeatedly to the situation that once petrified them, they can learn to react less anxiously (Barrera et al., 2013; Foa et al., 2013).
systematic desensitization a type of exposure therapy that associates a pleasant, relaxed state with gradually increasing anxiety-
One form of exposure therapy widely used to treat phobias is systematic desensitization. You cannot simultaneously be anxious and relaxed. Therefore, if you can repeatedly relax when facing anxiety-

In the next step, the therapist would train you in progressive relaxation. You would learn to relax one muscle group after another, until you achieved a comfortable, complete relaxation. The therapist might then ask you to imagine, with your eyes closed, a mildly anxiety-
The therapist will then move to the next item on your list, again using relaxation techniques to desensitize you to each imagined situation. After several sessions, you will move to actual situations and practice what you had only imagined before. You will begin with relatively easy tasks and gradually move to more anxiety-
“The only thing we have to fear is fear itself.”
U.S. President Franklin D. Roosevelt, First Inaugural Address, 1933
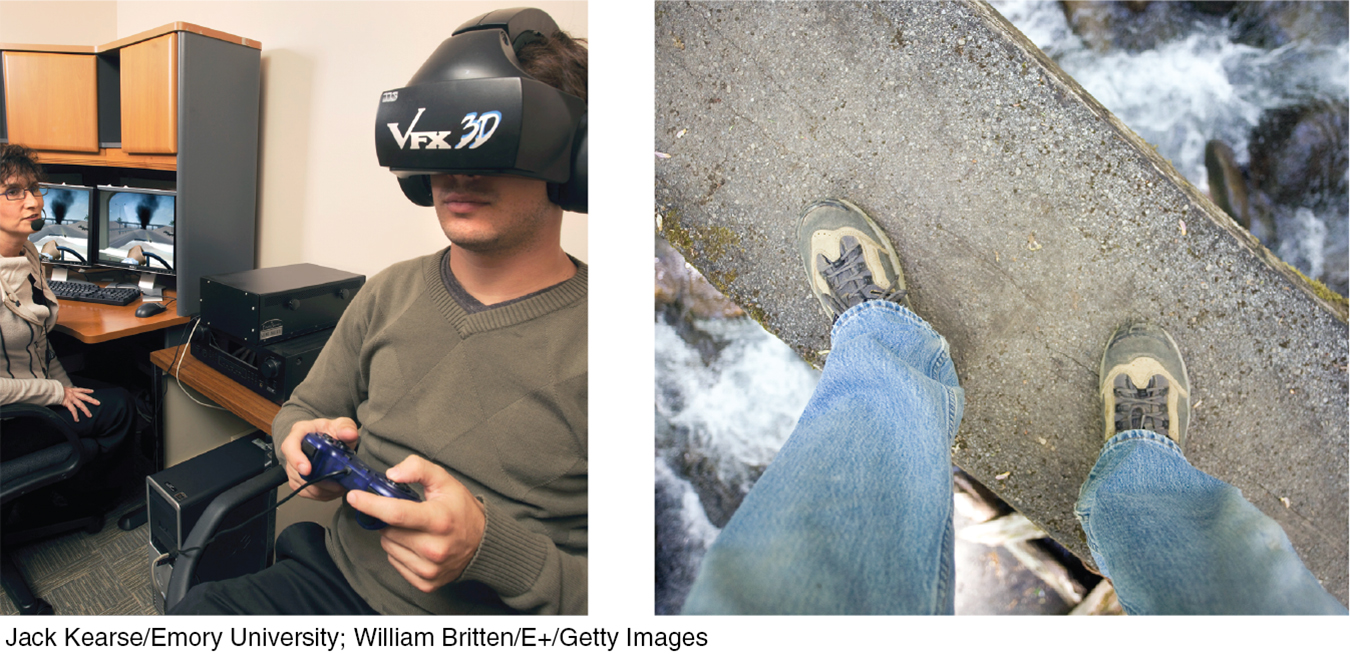
virtual reality exposure therapy an anxiety treatment that progressively exposes people to electronic simulations of their greatest fears, such as airplane flying, spiders, or public speaking.
If an anxiety-
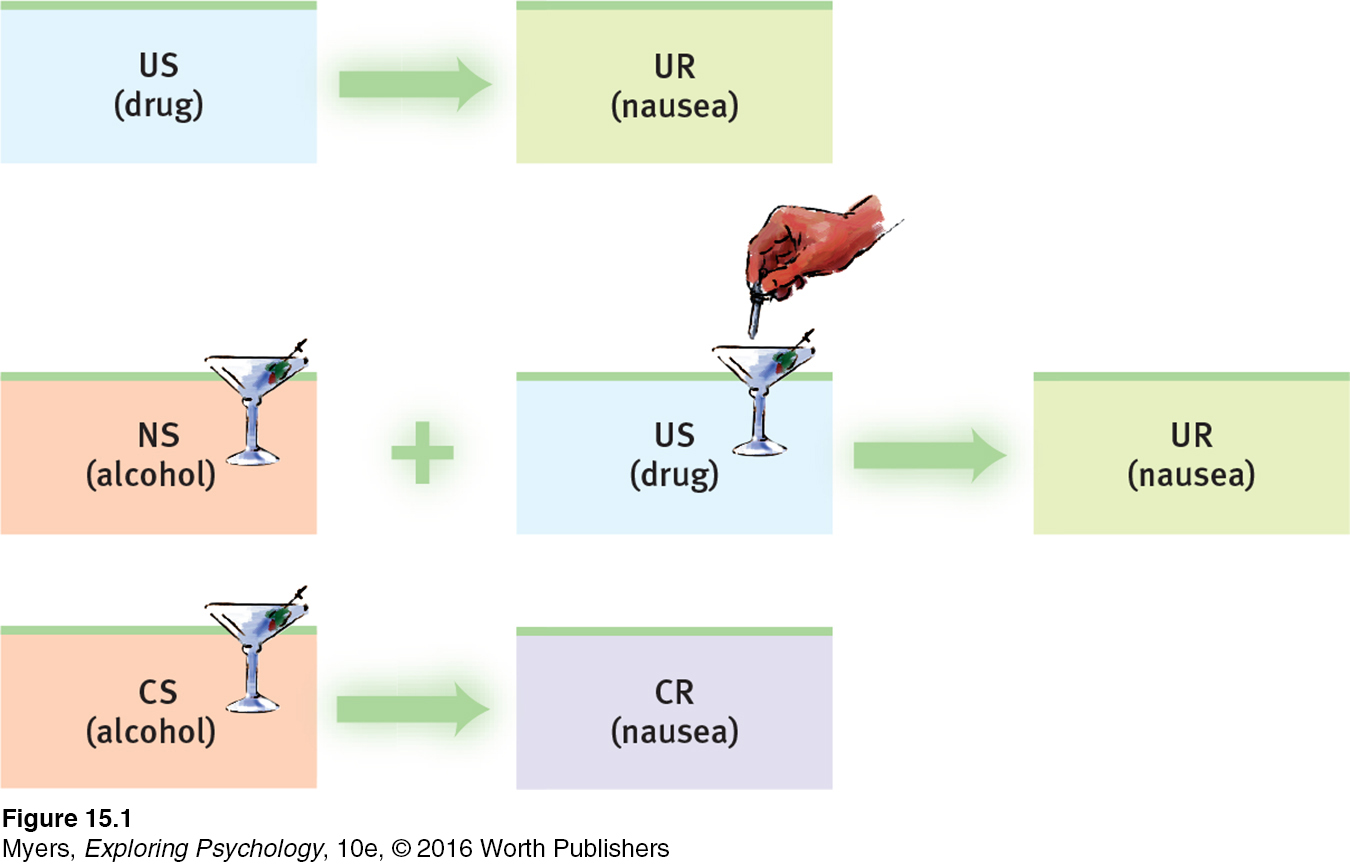
aversive conditioning a type of counterconditioning that associates an unpleasant state (such as nausea) with an unwanted behavior (such as drinking alcohol).
AVERSIVE CONDITIONING Exposure therapies enable a more relaxed, positive response to an upsetting harmless stimulus. Aversive conditioning creates a negative (aversive) response to a harmful stimulus (such as alcohol). Exposure therapies help you accept what you should do. Aversive conditioning helps you to learn what you should not do.
The aversive conditioning procedure is simple: It associates the unwanted behavior with unpleasant feelings. To treat nail biting, one can paint the fingernails with a nasty-
Does aversive conditioning work? In the short run it may. In one classic study, 685 hospital patients with alcohol use disorder completed an aversion therapy program (Wiens & Menustik, 1983). Over the next year, they returned for several booster treatments in which alcohol was paired with sickness. At the end of that year, 63 percent were still successfully abstaining. But after three years, only 33 percent had remained abstinent.
The problem is that in therapy (as in research), cognition influences conditioning. People know that outside the therapist’s office they can drink without fear of nausea. Their ability to discriminate between the aversive conditioning situation and all other situations can limit the treatment’s effectiveness. Thus, therapists often use aversive conditioning in combination with other treatments.
Operant Conditioning
15-
The work of B. F. Skinner and others teaches us a basic principle of operant conditioning: Voluntary behaviors are strongly influenced by their consequences. Knowing this, some behavior therapists practice behavior modification. They reinforce behaviors they consider desirable. And they fail to reinforce—
Using operant conditioning to solve specific behavior problems has raised hopes for some seemingly hopeless cases. Children with intellectual disabilities have been taught to care for themselves. Socially withdrawn children with autism spectrum disorder (ASD) have learned to interact. People with schizophrenia have been helped to behave more rationally in their hospital ward. In such cases, therapists used positive reinforcers to shape behavior. In a step-
 See LaunchPad’s Video: Research Ethics below for a helpful tutorial animation.
See LaunchPad’s Video: Research Ethics below for a helpful tutorial animation.
In extreme cases, treatment must be intensive. One study worked with 19 withdrawn, uncommunicative 3-
token economy an operant conditioning procedure in which people earn a token of some sort for exhibiting a desired behavior and can later exchange their tokens for various privileges or treats.
The rewards used to modify behavior vary because people differ in what they find reinforcing. For some, the reinforcing power of attention or praise is enough. Others require concrete rewards, such as food. In institutional settings, therapists may create a token economy. When people display desired behavior, such as getting out of bed, washing, dressing, eating, talking meaningfully, cleaning their rooms, or playing cooperatively, they receive a token or plastic coin. Later, they can exchange a number of these tokens for rewards, such as candy, TV time, day trips, or better living quarters. Token economies have been used successfully in various settings (homes, classrooms, hospitals, institutions for juvenile offenders) and among members of various populations (including disturbed children and people with schizophrenia and other mental disabilities).
Behavior modification critics express two concerns. The first is practical: How durable are the behaviors? Will people become so dependent on extrinsic rewards that the desired behaviors will stop when the reinforcers stop? Behavior modification advocates believe the behaviors will endure if therapists wean people from the tokens by shifting them toward other, real-
The second concern is ethical: Is it right for one human to control another’s behavior? Those who set up token economies deprive people of something they desire and decide which behaviors to reinforce. To critics, this whole process has an authoritarian taint. Advocates reply that control already exists; people’s destructive behavior patterns are already being maintained and perpetuated by natural reinforcers and punishers in their environments. Isn’t using positive rewards to reinforce adaptive behavior more humane than institutionalizing or punishing people? Advocates also argue that the right to effective treatment and an improved life justifies temporary deprivation.
RETRIEVE IT
Question
What are the insight therapies, and how do they differ from behavior therapies?
Question
Some maladaptive behaviors are learned. What hope does this fact provide?
Question
Exposure therapies and aversive conditioning are applications of conditioning. Token economies are an application of conditioning.
Cognitive Therapies
15-
People with specific fears and problem behaviors may respond to behavior therapy. But how would you modify the wide assortment of behaviors that accompany depressive disorders? And how would you treat generalized anxiety disorders, where unfocused anxiety doesn’t lend itself to a neat list of anxiety-
“Life does not consist mainly, or even largely, of facts and happenings. It consists mainly of the storm of thoughts that are forever blowing through one’s mind.”
Mark Twain, 1835–
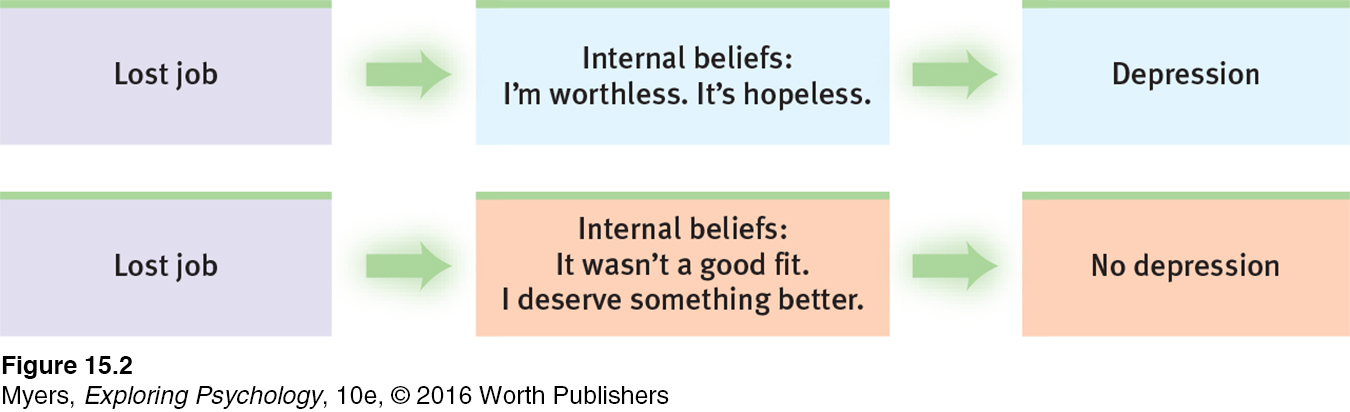
cognitive therapy therapy that teaches people new, more adaptive ways of thinking; based on the assumption that thoughts intervene between events and our emotional reactions.
The cognitive therapies assume that our thinking colors our feelings (FIGURE 15.2). Between an event and our response lies the mind. Self-
Beck’s Therapy for Depression
Cognitive therapist Aaron Beck believes that changing people’s thinking can change their functioning. Depressed people, he found, often reported dreams with negative themes of loss, rejection, and abandonment. These thoughts extended into their waking thoughts, and even into therapy, as clients recalled and rehearsed their failings and worst impulses (Kelly, 2000). With cognitive therapy, Beck and his colleagues (1979) sought to reverse clients’ negativity about themselves, their situations, and their futures. With this technique, gentle questioning seeks to reveal irrational thinking, and then to persuade people to remove the dark glasses through which they view life (Beck et al., 1979, pp. 145-
Client: I agree with the descriptions of me but I guess I don’t agree that the way I think makes me depressed.
Beck: How do you understand it?
Client: I get depressed when things go wrong. Like when I fail a test.
Beck: How can failing a test make you depressed?
Client: Well, if I fail I’ll never get into law school.
Beck: So failing the test means a lot to you. But if failing a test could drive people into clinical depression, wouldn’t you expect everyone who failed the test to have a depression? … Did everyone who failed get depressed enough to require treatment?
Client: No, but it depends on how important the test was to the person.
Beck: Right, and who decides the importance?
Client: I do.
Beck: And so, what we have to examine is your way of viewing the test (or the way that you think about the test) and how it affects your chances of getting into law school. Do you agree?
Client: Right.
Beck: Do you agree that the way you interpret the results of the test will affect you? You might feel depressed, you might have trouble sleeping, not feel like eating, and you might even wonder if you should drop out of the course.
Client: I have been thinking that I wasn’t going to make it. Yes, I agree.
Beck: Now what did failing mean?
Client: (tearful) That I couldn’t get into law school.
Beck: And what does that mean to you?
Client: That I’m just not smart enough.
Beck: Anything else?
Client: That I can never be happy.
Beck: And how do these thoughts make you feel?
Client: Very unhappy.
Beck: So it is the meaning of failing a test that makes you very unhappy. In fact, believing that you can never be happy is a powerful factor in producing unhappiness. So, you get yourself into a trap—
We often think in words. Therefore, getting people to change what they say to themselves is an effective way to change their thinking. Perhaps you can identify with the anxious students who, before an exam, make matters worse with self-
To change such negative self-
Selected Cognitive Therapy Techniques
| Aim of Technique | Technique | Therapists’ Directives |
|---|---|---|
| Reveal beliefs | Question your interpretations | Explore your beliefs, revealing faulty assumptions such as “I must be liked by everyone.” |
| Rank thoughts and emotions | Gain perspective by ranking your thoughts and emotions from mildly to extremely upsetting. | |
| Test beliefs | Examine consequences | Explore difficult situations, assessing possible consequences and challenging faulty reasoning. |
| Decatastrophize thinking | Work through the actual worst- |
|
| Change beliefs | Take appropriate responsibility | Challenge total self- |
| Resist extremes | Develop new ways of thinking and feeling to replace maladaptive habits. For example, change from thinking “I am a total failure” to “I got a failing grade on that paper, and I can make these changes to succeed next time.” |
It’s not just depressed people who can benefit from positive self-
Cognitive-Behavioral Therapy
cognitive-behavioral therapy (CBT) a popular integrative therapy that combines cognitive therapy (changing self-
“The trouble with most therapy,” said therapist Albert Ellis (1913–
Anxiety, depressive disorders, and bipolar disorder share a common problem: emotion regulation (Aldao & Nolen-
CBT may also be useful with obsessive-
A newer CBT variation, dialectical behavior therapy (DBT), helps change harmful and even suicidal behavior patterns (Linehan et al., 2015; Valentine et al., 2015). DBT combines cognitive tactics for tolerating distress and regulating emotions with social skills training and mindfulness meditation. Individual therapy aims to teach both acceptance and change—
RETRIEVE IT
Question
How do the humanistic and cognitive therapies differ?
Question
An influential cognitive therapy for depression was developed by .
Question
What is cognitive-behavioral therapy, and what sorts of problems does this therapy best address?
Group and Family Therapies
15-
Group Therapy
group therapy therapy conducted with groups rather than individuals, permitting therapeutic benefits from group interaction.
Except for traditional psychoanalysis, most therapies may also occur in small groups. Group therapy does not provide the same degree of therapist involvement with each client. However, it offers many benefits:
It saves therapists’ time and clients’ money, often with no less effectiveness than individual therapy (Fuhriman & Burlingame, 1994).
It offers a social laboratory for exploring social behaviors and developing social skills. Therapists frequently suggest group therapy for people experiencing frequent conflicts or whose behavior distresses others. For up to 90 minutes weekly, the therapist guides people’s interactions as they discuss issues and try out new behaviors.
It enables people to see that others share their problems. It can be a relief to discover that you are not alone—
to learn that others, despite their composure, experience some of the same troublesome feelings and behaviors. It provides feedback as clients try out new ways of behaving. Hearing that you look poised, even though you feel anxious and self-
conscious, can be reassuring.
Family Therapy
family therapy therapy that treats the family as a system. Views an individual’s unwanted behaviors as influenced by, or directed at, other family members.
One special type of group interaction, family therapy, assumes that no person is an island. We live and grow in relation to others, especially our families, yet we also work to find an identity outside of our family. These two opposing tendencies can create stress for both the individual and the family.

Unlike most psychotherapy, which focuses on what happens inside the person’s own skin, family therapists work with multiple family members to heal relationships and to mobilize family resources. They tend to view the family as a system in which each person’s actions trigger reactions from others, and they help family members discover their role within their family’s social system. A child’s rebellion, for example, affects and is affected by other family tensions. Therapists also attempt—
Self-Help Groups
More than 100 million Americans belong to small religious, interest, or support groups that meet regularly—
The grandparent of support groups, Alcoholics Anonymous (AA), reports having 2.1 million members in 115,000 groups worldwide. Its famous 12-
With more than 2 million members worldwide, AA is said to be “the largest organization on Earth that nobody wanted to join” (Finlay, 2000).
To review the aims and techniques of different psychotherapies, and assess your ability to recognize excerpts from each, visit LaunchPad’s PsychSim 6: Mystery Therapist.
In an individualist age, with more and more people living alone or feeling isolated, the popularity of support groups—
* * *
For a synopsis of these modern psychotherapies, see TABLE 15.2.
Comparing Modern Psychotherapies
| Therapy | Presumed Problem | Therapy Aim | Therapy Technique |
|---|---|---|---|
| Psychodynamic | Unconscious conflicts from childhood experiences | Reduce anxiety through self- |
Interpret patients’ memories and feelings. |
| Client- |
Barriers to self- |
Enable growth via unconditional positive regard, genuineness, acceptance, and empathy. | Listen actively and reflect clients’ feelings. |
| Behavior | Dysfunctional behaviors | Learn adaptive behaviors; extinguish problem ones. | Use classical conditioning (via exposure or aversion therapy) or operant conditioning (as in token economies). |
| Cognitive | Negative, self- |
Promote healthier thinking and self- |
Train people to dispute negative thoughts and attributions. |
| Cognitive- |
Self- |
Promote healthier thinking and adaptive behaviors. | Train people to counter self- |
| Group and family | Stressful relationships | Heal relationships. | Develop an understanding of family and other social systems, explore roles, and improve communication. |
RETRIEVE IT
Question
Which therapeutic technique focuses more on the present and future than the past, and involves unconditional positive regard and active listening?
Question
Which of the following is NOT a benefit of group therapy?
| A. |
| B. |
| C. |
| D. |
Evaluating Psychotherapies
Many Americans have great confidence in psychotherapy’s effectiveness. “Seek counseling” or “Ask your mate to find a therapist,” advice columnists often advise. Before 1950, psychiatrists were the primary providers of mental health care. Today’s providers include clinical and counseling psychologists; clinical social workers; pastoral, marital, abuse, and school counselors; and psychiatric nurses. With such an enormous outlay of time as well as money and effort, it is important to ask: Are the millions of people worldwide justified in placing their hopes in psychotherapy?

Is Psychotherapy Effective?
15-
Asking whether psychotherapy has worked is not as simple as asking whether antibiotics have worked to treat an infection. So how can we assess psychotherapy’s effectiveness? By how we feel about our progress? By how our therapist feels about it? By how our friends and family feel about it? By how our behavior has changed?
CLIENTS’ PERCEPTIONS If clients’ testimonials were the only measuring stick, we could strongly assert psychotherapy’s effectiveness. Consider the 2900 Consumer Reports readers who reported on their experiences with mental health professionals (1995; Kotkin et al., 1996; Seligman, 1995). How many were at least “fairly well satisfied”? Almost 90 percent (as was Kay Redfield Jamison, as we saw at this chapter’s beginning). Among those who recalled feeling fair or very poor when beginning therapy, 9 in 10 now were feeling very good, good, or at least so-
But client testimonials don’t persuade everyone. Critics note reasons for skepticism:
People often enter therapy in crisis. When, with the normal ebb and flow of events, the crisis passes, people may assume their improvement was a result of the therapy. Depressed people often get better no matter what they do.
Clients believe that treatment will be effective. The placebo effect is the healing power of positive expectations.
Clients generally speak kindly of their therapists. Even if the problems remain, clients “work hard to find something positive to say. The therapist had been very understanding, the client had gained a new perspective, he learned to communicate better, his mind was eased, anything at all so as not to have to say treatment was a failure” (Zilbergeld, 1983, p. 117).
Clients want to believe the therapy was worth the effort. People may feel the need to justify their investment of money, time, and hope.

CLINICIANS’ PERCEPTIONS If clinicians’ perceptions were proof of therapy’s effectiveness, we would have even more reason to celebrate. Case studies of successful treatment abound. Furthermore, therapists are like the rest of us. They treasure compliments from clients saying good-
OUTCOME RESEARCH How, then, can we objectively assess psychotherapy’s effectiveness? What outcomes can we expect—
To test your own therapeutic listening skills, visit LaunchPad’s Assess Your Strengths self-
In search of answers, psychologists have turned to controlled research. This is a well-
In the twentieth century, psychology, with its many different therapy options, faced a similar challenge. British psychologist Hans Eysenck (1952) launched a spirited debate when he summarized 24 studies of psychotherapy outcomes. He found that two-
Why, then, are we still debating psychotherapy’s effectiveness? Because Eysenck also reported similar improvement among untreated persons, such as those who were on waiting lists for treatment. With or without psychotherapy, he said, roughly two-
An avalanche of criticism greeted Eysenck’s conclusions. Some pointed out errors in his analyses. Others noted that he based his ideas on only 24 studies. Now, more than a half-
Therapists welcomed the first meta-
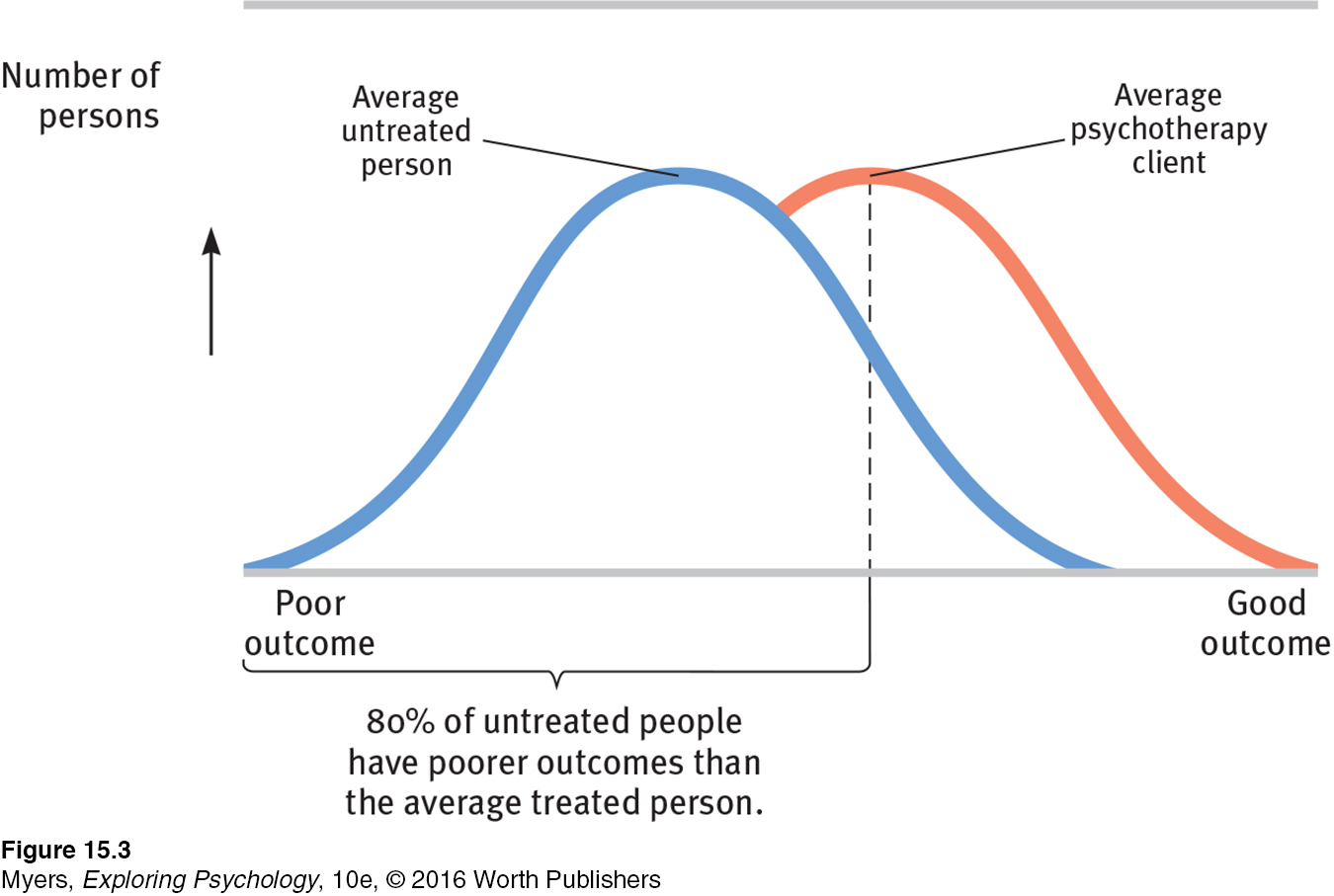
Dozens of subsequent summaries have now examined psychotherapy’s effectiveness. Their verdict echoes the results of the earlier outcome studies: Those not undergoing therapy often improve, but those undergoing therapy are more likely to improve, and to improve more quickly and with less risk of relapse. Moreover, between the treatment sessions for depression and anxiety, many people experience sudden symptom reductions. Those “sudden gains” bode well for long-
Is psychotherapy also cost-
But note that the claim—
RETRIEVE IT
Question
How might the placebo effect bias clients' and clinicians' appraisals of the effectiveness of psychotherapies?
Which Psychotherapies Work Best?
15-
The early statistical summaries and surveys did not find that any one type of psychotherapy is generally better than others (Smith et al., 1977, 1980). Later studies have similarly found little connection between clients’ outcomes and their clinicians’ experience, training, supervision, and licensing (Luborsky et al., 2002; Wampold, 2007). A Consumer Reports survey illustrated this point by asking: Were clients treated by a psychiatrist, psychologist, or social worker? Were they seen in a group or individual context? Did the therapist have extensive or relatively limited training and experience? It didn’t matter. Clients seemed equally satisfied (Seligman, 1995).
“Whatever differences in treatment efficacy exist, they appear to be extremely small, at best.”
Bruce Wampold et al. (1997)
So, was the dodo bird in Alice in Wonderland right: “Everyone has won and all must have prizes”? Not quite. Some forms of therapy get prizes for effectively treating particular problems. Behavioral conditioning therapies have had especially good results with specific behavior problems, such as bed-
Moreover, we can say that therapy is most effective when the problem is clear-
“Different sores have different salves.”
English proverb
But no prizes—
As with some medical treatments, it’s possible for psychological treatments to be not only ineffective but also harmful—
The evaluation question—
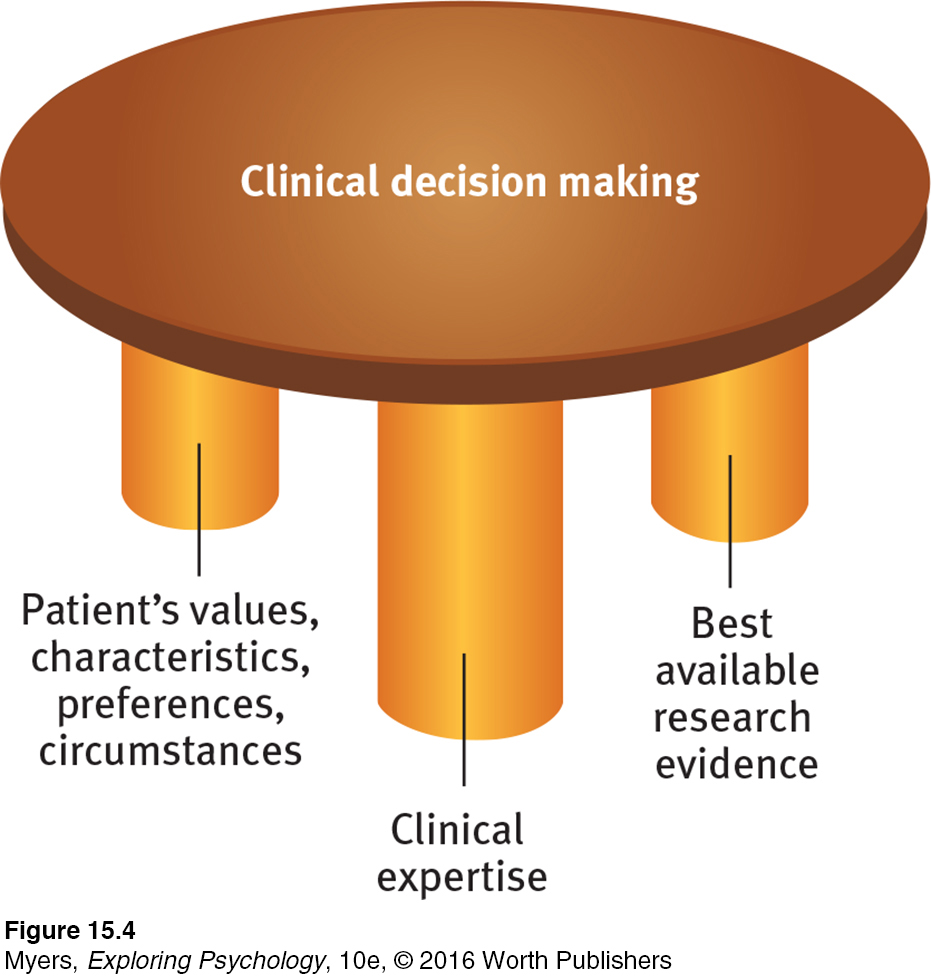
evidence-based practice clinical decision making that integrates the best available research with clinical expertise and patient characteristics and preferences.
Between these two factions stand the science-
RETRIEVE IT
Question
Therapy is most likely to be helpful for those with problems that (are/are not) well-defined.
Evaluating Alternative Therapies
15-10 How do alternative therapies fare under scientific scrutiny?
The tendency of many abnormal states of mind to return to normal, combined with the placebo effect (the healing power of mere belief in a treatment), creates fertile soil for pseudotherapies. Bolstered by anecdotes, boosted by the media, and broadcast on the Internet, alternative therapies—
Proponents of alternative therapies often feel that their personal testimonials are evidence enough. But how well do these therapies stand up to scientific scrutiny? There is little evidence for or against most of them. Some, however, have been the subject of controlled research. Let’s consider two. As we do, remember that sifting sense from nonsense requires the scientific attitude: being skeptical but not cynical, open to surprises but not gullible.
EYE MOVEMENT DESENSITIZATION AND REPROCESSING DR EMDR (eye movement desensitization and reprocessing) is a therapy adored by thousands and dismissed by thousands more as a sham—
Psychologist Francine Shapiro (1989, 2007, 2012) developed EMDR while walking in a park and observing that anxious thoughts vanished as her eyes spontaneously darted about. Back in the clinic, she had people imagine traumatic scenes while she triggered eye movements by waving her finger in front of their eyes, supposedly enabling them to unlock and reprocess previously frozen memories. Tens of thousands of mental health professionals from more than 75 countries have since undergone training (EMDR, 2011). No new therapy has attracted so many devotees so quickly since Franz Anton Mesmer introduced hypnosis (then called animal magnetism) more than two centuries ago (also after feeling inspired by an outdoor experience).
Does EMDR work? Shapiro believes it does, and she cites four studies in which it worked for 84 to 100 percent of single-trauma victims (Shapiro, 1999, 2002). Moreover, the treatment need take no more than three 90-
“Studies indicate that EMDR is just as effective with fixed eyes. If that conclusion is right, what’s useful in the therapy (chiefly behavioral desensitization) is not new, and what’s new is superfluous.”
Harvard Mental Health Letter, 2002
Why, wonder the skeptics, would rapidly moving one’s eyes while recalling traumas be therapeutic? Some argue that the eye movements relax or distract patients, thus allowing memory-
LIGHT EXPOSURE THERAPY Have you ever found yourself oversleeping, gaining weight, and feeling lethargic during the dark mornings and overcast days of winter? Slowing down and conserving energy during the cold, barren winters likely gave our distant ancestors a survival advantage. For people today, however—

Was light exposure a bright idea, or another dim-
RETRIEVE IT
Question
What is evidence-
Question
Which of the following alternative therapies HAS shown promise as an effective treatment?
| A. |
| B. |
| C. |
| D. |
How Do Psychotherapies Help People?
15-
How can it be that therapists’ training and experience do not seem to influence clients’ outcomes? The answer seems to be that all psychotherapies offer three basic benefits (Frank, 1982; Goldfried & Padawer, 1982; Strupp, 1986; Wampold 2001, 2007).
To test your own levels of hopefulness, visit LaunchPad’s Assess Your Strengths self-
HOPE FOR DEMORALIZED PEOPLE People seeking therapy typically feel anxious, depressed, self-
A NEW PERSPECTIVE LEADING TO NEW BEHAVIORS Every psychotherapy offers people an explanation of their symptoms. Therapy is a new experience that can help people change their behaviors and their views of themselves. Armed with a believable fresh perspective, they may approach life with new energy.
therapeutic alliance a bond of trust and mutual understanding between a therapist and client, who work together constructively to overcome the client’s problem.
AN EMPATHIC, TRUSTING, CARING RELATIONSHIP No matter what technique they use, effective psychotherapists are empathic. They seek to understand people’s experience. They communicate care and concern. And they earn trust through respectful listening, reassurance, and guidance. These qualities were clear in recorded therapy sessions from 36 recognized master therapists (Goldfried et al., 1998). Some took a cognitive-
That all psychotherapies offer hope through a fresh perspective provided by a caring person is what also enables paraprofessionals (briefly trained caregivers) to assist so many troubled people so effectively (Christensen & Jacobson, 1994). These three common elements are also part of what the growing numbers of self-
* * *
To recap, people who seek help usually improve. So do many of those who do not undergo psychotherapy, and that is a tribute to our human resourcefulness and our capacity to care for one another. Nevertheless, though the therapist’s orientation and experience appear not to matter much, people who receive some psychotherapy usually improve more than those who do not. People with clear-
RETRIEVE IT
Question
Those who undergo psychotherapy are (more/less) likely to show improvement than those who do not undergo psychotherapy.
Culture and Values in Psychotherapy
15-
All psychotherapies offer hope. Nearly all psychotherapists attempt to enhance their clients’ sensitivity, openness, personal responsibility, and sense of purpose (Jensen & Bergin, 1988). But therapists also differ from one another and may differ from their clients (Delaney et al., 2007; Kelly, 1990).
These differences can create a mismatch when a therapist from one culture interacts with a client from another. In North America, Europe, and Australia, for example, many therapists reflect the majority culture’s individualism, which often gives priority to personal desires and identity. Clients with a collectivist perspective, as with many from Asian cultures, may assume people will be more mindful of others’ expectations. These clients may have trouble relating to therapies that require them to think only of their own well-
Such differences help explain minority populations’ reluctance to use mental health services, and their tendency to prematurely terminate therapy (Chen et al., 2009; Sue, 2006). In one experiment, Asian-
Therapist and client may also have differing religious perspectives. Highly religious people may prefer and benefit from religiously similar therapists (Masters, 2010; Smith et al., 2007; Wade et al., 2006). They may have trouble establishing an emotional bond with a therapist who does not share their values. People living in “cultures of honor”—which prize being strong and tough—
Finding a Mental Health Professional
15-
Life for everyone is marked by a mix of serenity and stress, blessing and bereavement, good moods and bad. So, when should we seek a mental health professional’s help? The American Psychological Association offers these common trouble signals:
Feelings of hopelessness
Deep and lasting depression
Self-
destructive behavior, such as substance abuse Disruptive fears
Sudden mood shifts
Thoughts of suicide
Compulsive rituals, such as hand washing
Sexual difficulties
Hearing voices or seeing things that others don’t experience
In looking for a therapist, you may want to have a preliminary consultation with two or three. College health centers are generally good starting points, and may offer some free services. You can describe your problem and learn each therapist’s treatment approach. You can ask questions about the therapist’s values, credentials (TABLE 15.3), and fees. And you can assess your own feelings about each of them. The emotional bond between therapist and client is perhaps the most important factor in effective therapy.
Therapists and Their Training
| Type | Description |
|---|---|
| Clinical psychologists | Most are psychologists with a Ph.D. (includes research training) or Psy.D. (focuses on therapy) supplemented by a supervised internship and, often, postdoctoral training. About half work in agencies and institutions, half in private practice. |
| Psychiatrists | Psychiatrists are physicians who specialize in the treatment of psychological disorders. Not all psychiatrists have had extensive training in psychotherapy, but as M.D.s or D.O.s they can prescribe medications. Thus, they tend to see those with the most serious problems. Many have their own private practice. |
| Clinical or psychiatric social workers | A two- |
| Counselors | Marriage and family counselors specialize in problems arising from family relations. Clergy provide counseling to countless people. Abuse counselors work with substance abusers and with spouse and child abusers and their victims. Mental health and other counselors may be required to have a two- |
REVIEW Introduction to Therapy and the Psychological Therapies
Learning Objectives
Test Yourself by taking a moment to answer each of these Learning Objective Questions (repeated here from within the chapter). Research suggests that trying to answer these questions on your own will improve your long-
Question
15-
Question
15-
Question
15-
Question
15-
Question
15-
Question
15-
Question
15-
Question
15-
Question
15-
Question
15-
Question
15-
Question
15-
Question
15-
Terms and Concepts to Remember
Test yourself on these terms.
Question
psychotherapy (p. 570) biomedical therapy (p. 570) eclectic approach (p. 570) psychoanalysis (p. 570) resistance (p. 571) interpretation (p. 571) transference (p. 571) psychodynamic therapy (p. 572) insight therapies (p. 572) client- active listening (p. 573) unconditional positive regard (p. 574) behavior therapy (p. 574) counterconditioning (p. 575) exposure therapies (p. 575) systematic desensitization (p. 575) virtual reality exposure therapy (p. 576) aversive conditioning (p. 576) token economy (p. 577) cognitive therapy (p. 578) cognitive- group therapy (p. 582) family therapy (p. 582) evidence- therapeutic alliance (p. 589) | a type of counterconditioning that associates an unpleasant state (such as nausea) with an unwanted behavior (such as drinking alcohol). in psychoanalysis, the patient's transfer to the analyst of emotions linked with other relationships (such as love or hatred for a parent). therapy conducted with groups rather than individuals, permitting therapeutic benefits from group interaction. a type of exposure therapy that associates a pleasant, relaxed state with gradually increasing anxiety- in psychoanalysis, the blocking from consciousness of anxiety- a variety of therapies that aim to improve psychological functioning by increasing a person's awareness of underlying motives and defenses. a bond of trust and mutual understanding between a therapist and client, who work together constructively to overcome the client's problem. behavior therapy procedures that use classical conditioning to evoke new responses to stimuli that are triggering unwanted behaviors; include exposure therapies and aversive conditioning. an operant conditioning procedure in which people earn a token of some sort for exhibiting a desired behavior and can later exchange their tokens for various privileges or treats. an approach to psychotherapy that uses techniques from various forms of therapy. in psychoanalysis, the analyst's noting supposed dream meanings, resistances, and other significant behaviors and events in order to promote insight. a humanistic therapy, developed by Carl Rogers, in which the therapist uses techniques such as active listening within a genuine, accepting, empathic environment to facilitate clients' growth. (Also called person- therapy that treats the family as a system. Views an individual's unwanted behaviors as influenced by, or directed at, other family members. empathic listening in which the listener echoes, restates, and clarifies. A feature of Rogers' client- behavioral techniques, such as systematic desensitization and virtual reality exposure therapy, that treat anxieties by exposing people (in imagination or actual situations) to the things they fear and avoid. therapy that applies learning principles to the elimination of unwanted behaviors. prescribed medications or procedures that act directly on the person's physiology. therapy that teaches people new, more adaptive ways of thinking; based on the assumption that thoughts intervene between events and our emotional reactions. a caring, accepting, nonjudgmental attitude, which Carl Rogers believed would help clients develop self- a popular integrative therapy that combines cognitive therapy (changing self- Freud's therapeutic technique used in treating psychological disorders. Freud believed the patient's free associations, resistances, dreams, and transferences— therapy deriving from the psychoanalytic tradition; views individuals as responding to unconscious forces and childhood experiences, and seeks to enhance self- treatment involving psychological techniques; consists of interactions between a trained therapist and someone seeking to overcome psychological difficulties or achieve personal growth. an anxiety treatment that progressively exposes people to electronic simulations of their greatest fears, such as airplane flying, spiders, or public speaking. clinical decision making that integrates the best available research with clinical expertise and patient characteristics and preferences. |
Experience the Testing Effect
Test yourself repeatedly throughout your studies. This will not only help you figure out what you know and don’t know; the testing itself will help you learn and remember the information more effectively thanks to the testing effect.
Question 15.1
1. A therapist who helps patients search for the unconscious roots of their problem and offers interpretations of their behaviors, feelings, and dreams is drawing from
| A. |
| B. |
| C. |
| D. |
Question 15.2
2. therapies are designed to help individuals discover the thoughts and feelings that guide their motivation and behavior.
Question 15.3
3. Compared with psychoanalysts, humanistic therapists are more likely to emphasize
| A. |
| B. |
| C. |
| D. |
Question 15.4
4. A therapist who restates and clarifies the client's statements is practicing .
Question 15.5
5. The goal of behavior therapy is to
| A. |
| B. |
| C. |
| D. |
Question 15.6
6. Behavior therapies often use techniques, such as systematic desensitization and aversive conditioning, to encourage clients to produce new responses to old stimuli.
Question 15.7
7. The technique of teaches people to relax in the presence of progressively more anxiety-provoking stimuli.
Question 15.8
8. After a near-fatal car accident, Rico developed such an intense fear of driving on the freeway that he takes lengthy alternative routes to work each day. Which psychological therapy might best help Rico overcome his phobia, and why?
Question 15.9
9. At a treatment center, people who display a desired behavior receive coins that they can later exchange for other rewards. This is an example of a(n) .
Question 15.10
10. Cognitive therapy has been especially effective in treating
| A. |
| B. |
| C. |
| D. |
Question 15.11
11. therapy helps people to change their self-defeating ways of thinking and to act out those changes in their daily behavior.
Question 15.12
12. In family therapy, the therapist assumes that
| A. |
| B. |
| C. |
| D. |
Question 15.13
13. The most enthusiastic or optimistic view of the effectiveness of psychotherapy comes from
| A. |
| B. |
| C. |
| D. |
Question 15.14
14. Studies show that ________ therapy is the most effective treatment for most psychological disorders.
| A. |
| B. |
| C. |
| D. |
Question 15.15
15. What are the three components of evidence-based practice?
Question 15.16
16. How does the placebo effect bias patients' attitudes about the effectiveness of various therapies?
Use  to create your personalized study plan, which will direct you to the resources that will help you most in
.
to create your personalized study plan, which will direct you to the resources that will help you most in
.