7.7 POPULATION AND GENDER
GEOGRAPHIC INSIGHT 5
Population and Gender: Of all the world regions, populations are growing fastest in sub-Saharan Africa. However, growth is slowing as the demographic transition takes hold, especially in a few of the more prosperous countries where better health care and lower levels of child mortality, along with more economic and educational opportunities, are encouraging smaller families. In particular, women are better able to pursue careers and to choose to have fewer children.
Page 306
ON THE BRIGHT SIDE
The problem of unsafe water for households may have a solution that is simple, affordable, and may create local jobs. A for-profit group, working with grassroots organizations in Uganda but subsidized by American investors, has designed a simple plastic jug, called the TivaWater jug, with an interior sand and clay filtering device that purifies water (Figure 7.23). The jug is made to be affordable to urban poor people in Ugandan shantytowns. While initially made in the United States, the jug is now manufactured in Uganda, is sold and distributed by small businesses there, and will eventually be exported by Ugandans to other African countries.
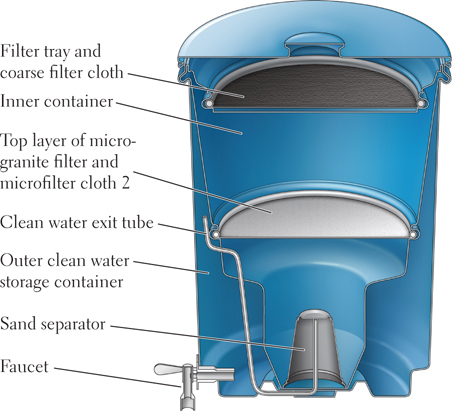
Figure 7.23: The TivaWater jug. This specially designed water-filtering jug, made of unbreakable food-grade plastic, removes dirt, bacteria, and viruses, using a new version of biosand technology. It is affordable through subsidies to the very poor, is easy to maintain, and has a faucet that dispenses the water.
In fewer than 50 years, sub-Saharan Africa’s population has more than quadrupled, growing from about 2003 million in 1960 to 828 million in 2009 to slightly under 1 billion in 2013. By 2050, the population of this region could reach just over 2 billion. Contrary to the perception outsiders often hold, however, Africa as a whole is much less densely populated than most of Europe and Asia—36 people per square kilometer, compared to the global average of 51 people per square kilometer. If fertility rates remain high though, places that are relatively uncrowded now may change dramatically over the next few decades (Figure 7.24; see also Figure 1.26). In some rural areas, the population density may far exceed the carrying capacity of the land, which will lead to the impoverishment of subsistence farmers. Increasingly, however, Africa’s population is becoming concentrated in a few urban areas, such as the cities along the coast of the Gulf of Guinea in West Africa, discussed later.
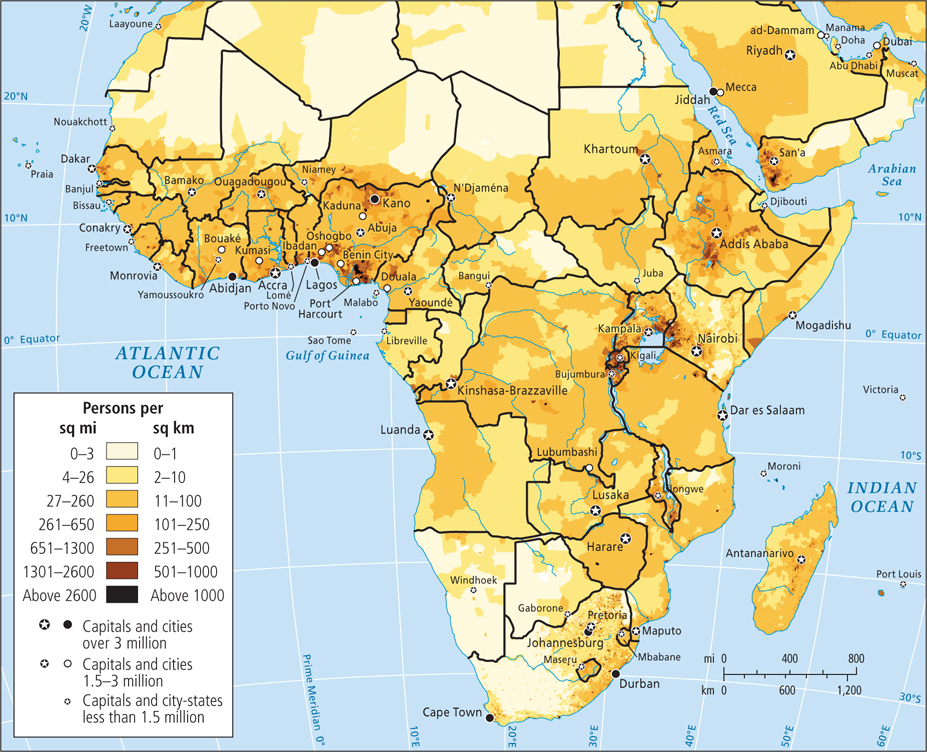
Figure 7.24: Population density in sub-Saharan Africa. Of all the world regions, populations are growing fastest in sub-Saharan Africa. The demographic transition is taking hold in a few of the more prosperous countries. In these countries, better health care and more economic and educational opportunities for women are enabling women to pursue careers and to choose to have fewer children.
[Sources consulted: Deborah Balk, Gregory Yetman, et al., Center for International Earth Science Information Network, Columbia University, at
http://www.ciesin.columbia.edu]
At the moment, sub-Saharan Africa’s annual rate of natural increase (2.6 percent) is the highest in the world; even so, overall rates are slowing in nearly every country, especially in urban areas. Nonetheless, people continue to have more children than would be necessary to simply maintain population numbers. Birth rates are as high as they are because many Africans view children as both an economic advantage and a spiritual link between the past and the future. Childlessness is considered a tragedy, as children ensure a family’s genetic and spiritual survival.
Large families are also viewed as having economic value, as children and young adults still perform important work on family farms and in family-scale industries. Moreover, in this region of generally poor health care and resultant high incidence of infant mortality, parents may have extra children in the hope of raising a few to maturity. In all but a few countries, the demographic transition—the sharp decline in births and deaths that usually accompanies economic development (see Figure 1.28)—has barely begun, and more people now survive long enough to reproduce than did in the past. If Africa is on the brink of a development surge, however, fertility rates could decline quite sharply as women choose roles other than motherhood.
At least five countries in the region have gone through the demographic transition. In South Africa, Botswana, Seychelles, Réunion, and Mauritius (the last three being small island countries off Africa’s east coast), circumstances have changed enough to make smaller families desirable and attainable. In all five countries, per capita incomes are five to ten times the sub-Saharan average of U.S.$2000. Advances in health care have cut the infant mortality rate to less than half the regional average of 88 infant deaths per 1000 live births. Because of this, parents can have only two or three children and expect them to live to adulthood. The circumstances of women in these five countries have also improved, as reflected in female literacy rates of about 80 to 90 percent, compared to the regional average of 54 percent. There are more opportunities for women to work outside the home at decent-paying jobs than there are in these countries than in the rest of the region. Thus, many women are choosing to use contraception because they have life options beyond motherhood. Indeed, the percentage of married women using contraception in these five countries is double or even triple the rate for sub-Saharan Africa as a whole, which is only 22 percent (the world average is 61 percent).
The population pyramids in Figure 7.25 show the contrast between countries that are growing rapidly, such as Nigeria, Africa’s most populous country (with 170.1 million people and a natural increase rate of 2.6 percent), and countries that have already gone through the demographic transition, such as South Africa (with 51.1 million people and a natural increase rate of 0.9 percent). Nigeria’s pyramid is very wide at the bottom because over half the population is under the age of 20. In just 15 years, this entire group will be of reproductive age. Only 15 percent of Nigerian women use any sort of birth control.
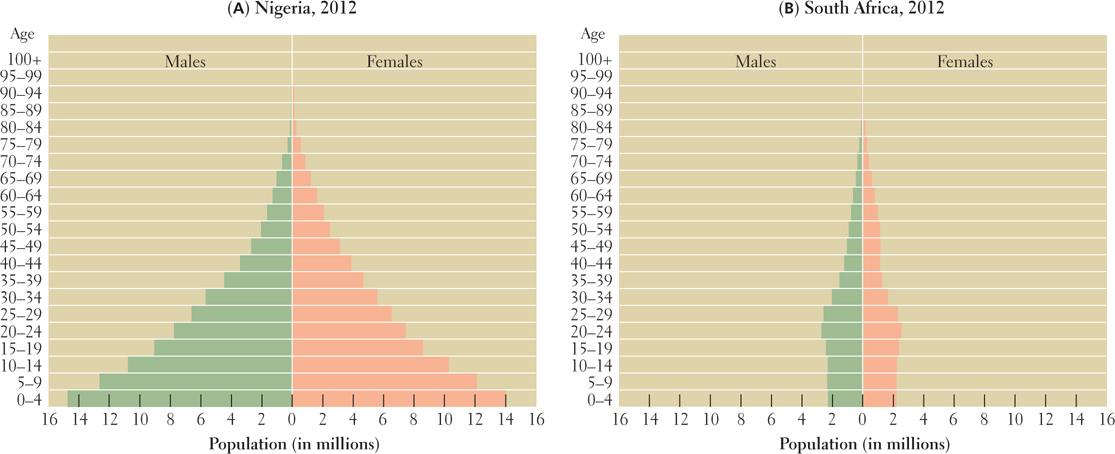
Figure 7.25: Population pyramids for Nigeria and South Africa. Note that the two pyramids are at the same scale. (A) Nigeria had a population of 170.1 million people in 2012 and a growth rate of 2.6 percent, as indicated by its very wide pyramid base. It has the largest population on the continent, nearly twice that of Ethiopia, which has the second-largest population. (B) South Africa, on the other hand, had a population of 51.1 million in 2012 and a growth rate of only 0.9 percent; its population is beginning to decline, as shown by the shrinking of the pyramid base. The decline is in part due to the AIDS epidemic.
In contrast to Nigeria, South Africa’s pyramid has contracted at the bottom because its birth rate has dropped from 35 per 1000 to 21 per 1000 over the last 20 years. This decrease is primarily an effect of economic and educational improvements as well as social changes that have come about since the end of apartheid (1994). It is likely to persist as the advantages of smaller families, become clear, especially to women. The birth rate decrease is all the more remarkable because contraception is used by only 60 percent of South African women. Part of the birth rate decrease in South Africa is probably a consequence of the high rate of HIV among young adults there.
Page 307
Population and Public Health Infectious diseases, including HIV-AIDS, are by far the largest killers in sub-Saharan Africa and are responsible for about 50 percent of all deaths. Some diseases are linked to particular ecological zones. For example, people living between the 15th parallels north and south of the equator are most likely to be exposed to sleeping sickness (trypanosomiasis), which is spread among people and cattle by the bites of tsetse flies. The disease attacks the central nervous system and results in death if untreated. Several hundred thousand Africans suffer from sleeping sickness, and most of them are not treated because they cannot afford the expensive drug therapy.
Africa’s most common chronic tropical diseases, schistosomiasis and malaria, are linked to standing fresh water. Their incidence has thus increased with the construction of dams and irrigation projects. Schistosomiasis is a debilitating, though rarely fatal, disease that affects about 170 million sub-Saharan Africans. It develops when a parasite carried by a particular freshwater snail enters the skin of a person standing in water. Malaria, spread by the anopheles mosquito (which lays its eggs in standing water), is more deadly. The disease kills at least 1 million sub-Saharan Africans annually, most of them children under the age of 5. Malaria also infects millions of adult Africans who are left feverish, lethargic, and unable to work efficiently because of the disease.
Until recently, relatively little funding was devoted to controlling the most common chronic tropical diseases. Now, however, major international donors are funding research in Africa and elsewhere. More than 60 research groups in Africa are working on a vaccine that will prevent malaria in most people.
Page 308
The distribution of simple, low-cost, and effective mosquito nets is also reducing the transmission rates of malaria.
HIV-AIDS in Sub-Saharan Africa A leading cause of death in Africa, and the leading cause of death for women of reproductive age, is acquired immunodeficiency syndrome (AIDS), caused by the human immunodeficiency virus (HIV) (Figure 7.26). As of 2010, more than 16 million sub-Saharan Africans had died of the disease, and as many as 80 million more AIDS-related deaths are expected by 2025. In 2010, sub-Saharan Africa had two-thirds of the estimated worldwide total of 33 million people living with HIV. In Botswana, one of the richest countries in Southern Africa, nearly 29.2 percent of the adult female population is infected. The Southern Africa region alone accounted for 31 percent of global AIDS deaths in 2010. While the epidemic is subsiding a bit, it has significantly constrained economic development.
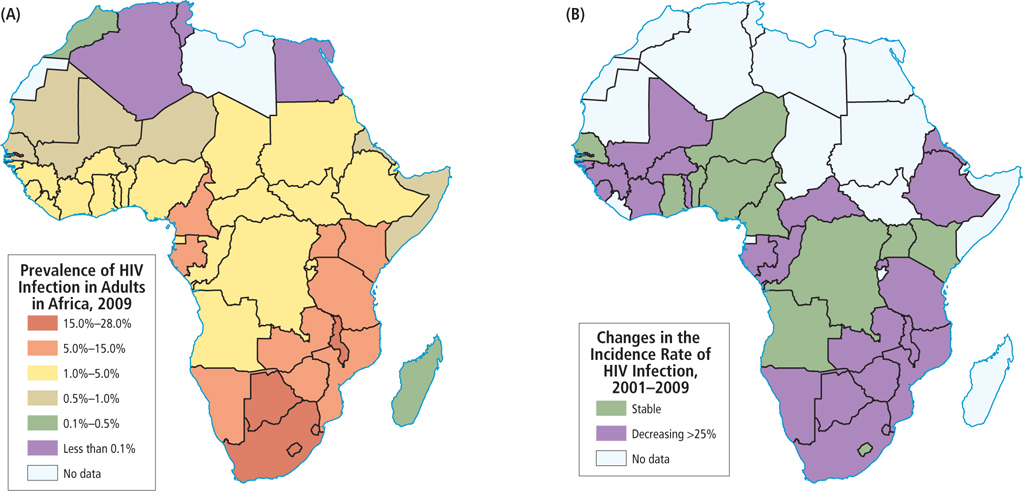
Figure 7.26: HIV-AIDS in Africa. New HIV infections fell in sub-Saharan Africa from 2.2 million in 2001 to 1.8 million in 2009. In this period, rates declined more than 25 percent in 22 of the countries. The rate has remained stable elsewhere in the region. The number of deaths from AIDS has declined in sub-Saharan Africa, in large part because of the increased availability of antiretroviral medications.
Worldwide, women account for half of all people living with HIV, but in Africa, HIV-AIDS affects women more than men: 59 percent of the region’s HIV-infected adults are women. The reasons for this pattern are related to the social status of women in sub-Saharan Africa and elsewhere.
The rapid urbanization of Africa has hastened the spread of HIV, which is much more prevalent in urban areas. It is not uncommon for poor, new urban migrants removed from their village support systems to become involved in the sex industry in order to survive economically. In some cities, virtually all sex workers are infected. Meanwhile, many urban men, especially those with families back in rural villages, visit prostitutes on a regular basis. These men often bring HIV back to their rural homes. As transportation between cities and the countryside has improved, bus and truck drivers have also become major carriers of HIV to rural villages.
A number of myths and social taboos surround HIV-AIDS, exacerbating the problem of controlling the spread of the disease and making education a key component in combating the epidemic. For example, some men think that only sex with a mature woman can result in infection, so very young girls are increasingly sought as sex partners (sometimes referred to as “the virgin ‘cure’”). Elsewhere, infection is considered such a disgrace that even those who are severely ill refuse to get tested, yet they remain sexually active.
The Social Costs of HIV-AIDS Across the continent, the consequences of the HIV-AIDS epidemic are enormous. Children contract HIV primarily in utero or from nursing; just over 400 children under the age of 15 die each day from AIDS-related causes. Millions of parents, teachers, skilled farmers, craftspeople, and trained professionals have been lost. More than 15 million children have been orphaned and many have no family left to care for them or to pass on vital knowledge and life skills. The disease has severely strained the health-care systems of most countries. Demand for treatment is exploding, drugs are prohibitively expensive, and many health-care workers themselves are infected. Because so many young people are dying of AIDS, decades of progress in improving the life expectancy of Africans have been erased. For example, in 1990, adult life expectancy in South Africa was 63 years, but in 2012 it was 54 years.
Page 309
HIV-AIDS Education and Medication The most effective means of prevention are the massive education programs that lower rates of infection among those who can read and understand explanations about how HIV is spread. For example, Senegal started HIV-AIDS education in the 1980s, and levels of infection there have so far remained low. Major education campaigns in Uganda lowered the incidence of new HIV infections from 15 percent to just 4.1 percent between 1990 and 2004. By contrast, infection rates have soared in areas such as South Africa, where a few top politicians have put forth untenable theories about the causes of HIV infection or have denied that HIV-AIDS is a problem.
HIV-AIDS medications (known as antiretroviral therapy) are prohibitively expensive for most families in sub-Saharan Africa. The United Nations and a number of private philanthropies cover some of the costs. The medications are not a cure and must be taken daily for the rest of one’s life, but they do make it possible to live with the disease. Pharmaceutical firms in India, China, and elsewhere have come out with generic antiretroviral versions that have reduced the cost to about $350 per year, about one-sixth of the average annual income in the region. Approximately five out of every six recipients worldwide are in sub-Saharan Africa, and most of those are in Southern Africa. As yet, only half of those who need the medicines are receiving them; the goal is for all of those with HIV-AIDS to be covered by 2015. The cost to the world of keeping parents alive with antiret-roviral therapy is far less than that of dealing with the social effects of millions of orphans.
THINGS TO REMEMBER
Population and Gender Of all the world regions, populations are growing fastest in sub-Saharan Africa. However, growth is slowing as the demographic transition takes hold, especially in a few of the more prosperous countries where better health care and lower levels of child mortality, along with more economic and educational opportunities, are encouraging smaller families. In particular, women are better able to pursue careers and to choose to have fewer children.
In fewer than 50 years, sub-Saharan Africa’s population has more than quadrupled, growing from about 200 million in 1960 to 828 million in 2009, to slightly under 1 billion in 2013. By 2050, the population of this region could reach just over 2 billion.
The overall low population density figures in sub-Saharan Africa—36 people per square kilometer, compared to the global average of 51 people per square kilometer—can be misleading. Densities are extremely high in some places and very low in less habitable areas.
Sub-Saharan Africa has higher rates of infectious diseases than any other region in the world, with the world’s worst epidemics of malaria, schistosomiasis, sleeping sickness, and HIV-AIDS.