11-1 A Hierarchy of Movement Control
Our movements feature at least two categories of action. First we decide on a goal and choose how to achieve it; then we make moves to reach the goal. As we move, we correct movement errors that direct us away from our goal. What are the neural bases of these choices? What neural bases enable the motor system to produce our movements?
The major components of our motor system are the cerebrum (forebrain), the brainstem, and the spinal cord. The cerebrum contributes to our conscious control of movement, while the brainstem and spinal cord direct our movements. In the face of impaired brainstem or spinal cord function, the forebrain can imagine movement but can no longer produce it. Neuroprosthetic devices, described in Research Focus 11-1, can replace the movement production function provided by the brainstem and spinal cord and restore forebrain control.
Getting from decisions to movements involves most of our nervous system. Figure 11-1 illustrates the stepwise sequence your CNS performs in the seemingly simple act of directing your hand to pick up a cup. Once you decide to pick it up, you visually inspect it to determine what part to grasp. The visual cortex relays this information through the cortical somatosensory regions to the motor regions that plan and initiate the movement. Only then does the brain send instructions to the spinal cord segments that control your arm and hand muscles.
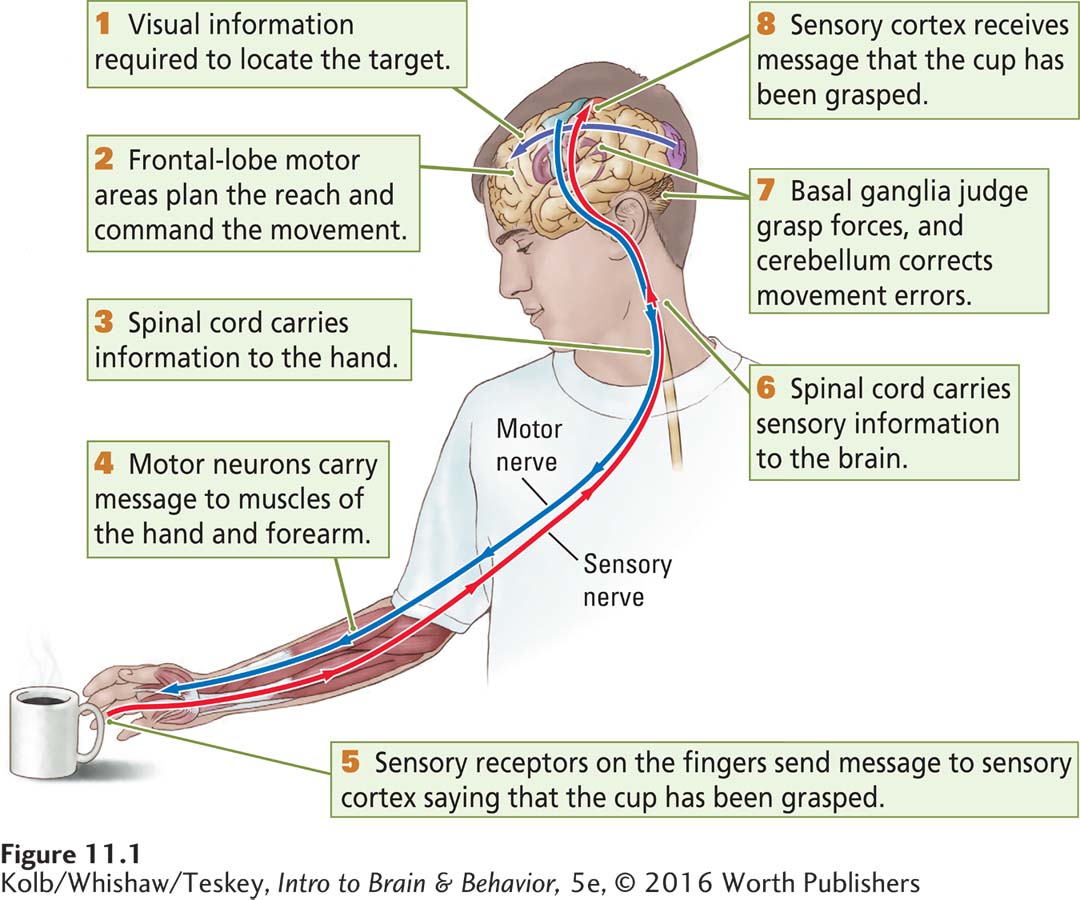
For now, remember that the entire sensorimotor system is organized hierarchically. When you reach the chapter’s end, review Figure 11-1 to reinforce what you’ve learned.
As you grasp the cup’s handle, information from sensory receptors in your fingers aids in adjusting your grip and sends information back through the spinal cord to the somatosensory cortex and from there to the motor cortex to confirm that the act is complete—
Recall the principle from Section 2-6: The CNS functions on multiple levels.
Clearly, the movement involved in picking up a cup involves widespread CNS regions. The action also requires that higher-
THE BASICS
Relating the Somatosensory and Motor Systems
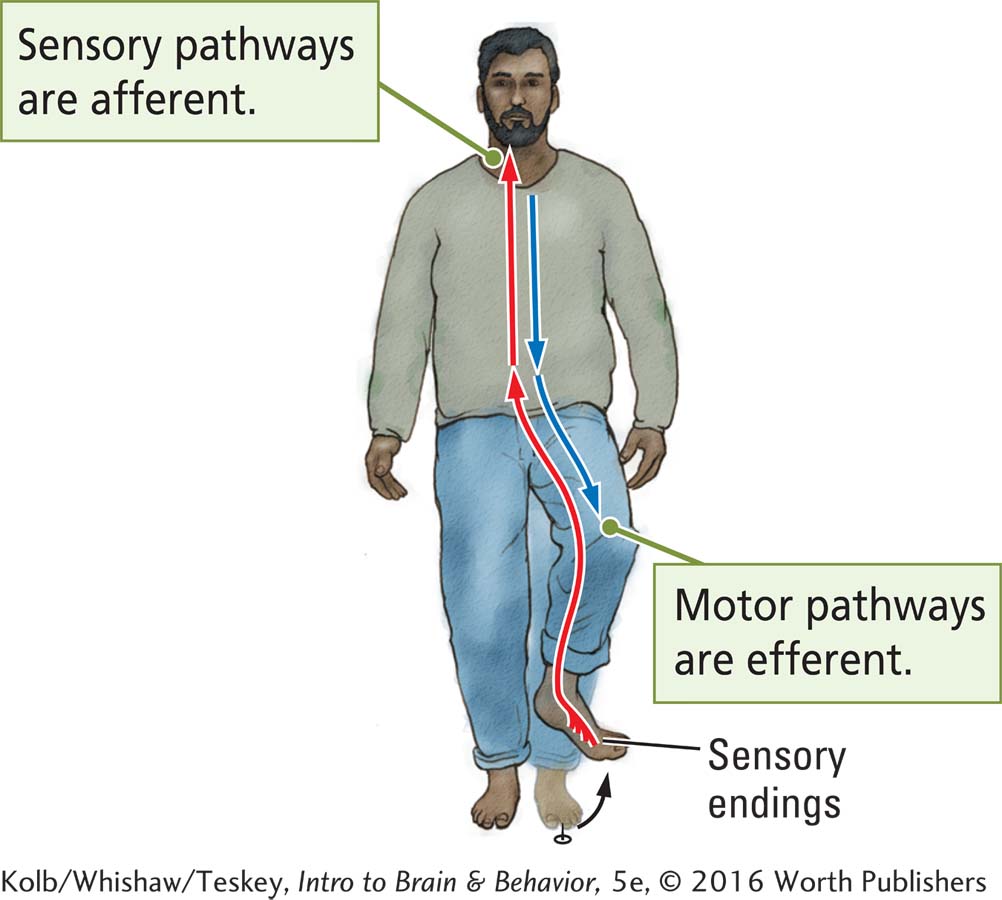
The intimate relationship between the motor and somatosensory systems is apparent in their close anatomical relationships. Afferent somatosensory information travels from the body inward via the somatic nervous system. Movement information travels out of the central nervous system via a parallel efferent motor system.
As diagrammed in Information Flow, when you step on a tack, the sensory signals transmitted by the SNS from the body through the spinal cord and into the brain are afferent. Efferent signals from the CNS trigger a motor response: you lift your foot.
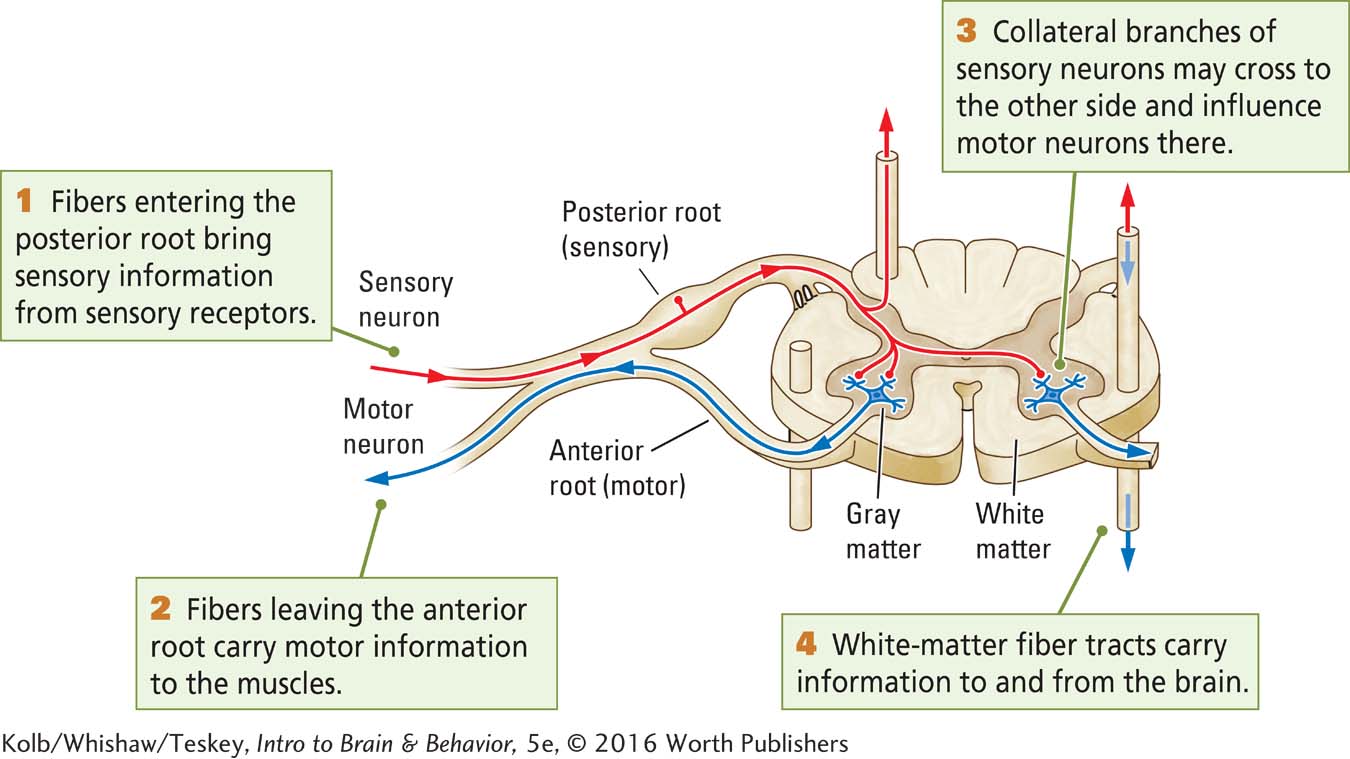
The spinal cord connects the somatosensory and motor systems throughout the CNS. Connections Between the Nerves and the Spine shows the spinal cord in cross section. In the outer part, which consists of white matter, posterior tracts are sensory and anterior tracts are motor, with some exceptions. The inner cord is gray matter composed largely of cell bodies and shaped like a butterfly.
SNS nerves entering the spinal cord’s posterior side carry information inward from the body’s sensory receptors and merge into a posterior root as the fibers enter a spinal cord segment of the CNS. Fibers leaving the spinal cord’s anterior side carry information out from the spinal cord to the muscles. They, too, bundle together as the fibers exit the spinal cord, forming an anterior root. (Bundles of nerve fibers within the CNS are called tracts; outside the CNS they are called nerves.)
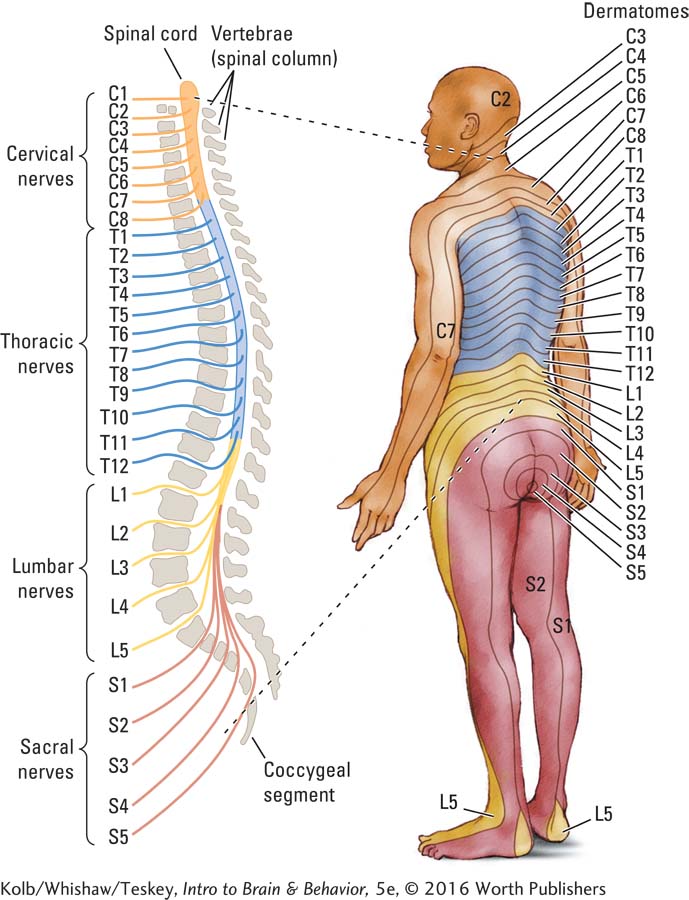
The spinal cord lies within a series of small bones called vertebrae categorized into the five anatomical regions diagrammed on the left in Spinal Segments and Dermatomes. Each spinal segment corresponds to a region of body surface called a dermatome (literally, skin cut), shown on the right. From top to bottom, the cervical, thoracic, lumbar, sacral, and coccygeal regions are identified by spinal segment number: C5 (cervical segment 5) at the base of the neck, for example, and L2 in the lower back.
Body and nervous system segmentation has a long evolutionary history that can be seen in spineless worms as well as in vertebrates. The cervical and lumbar dermatomes represent the human forelimbs and hind limbs. Their arrangement is sequential if you imagine a human on all fours.
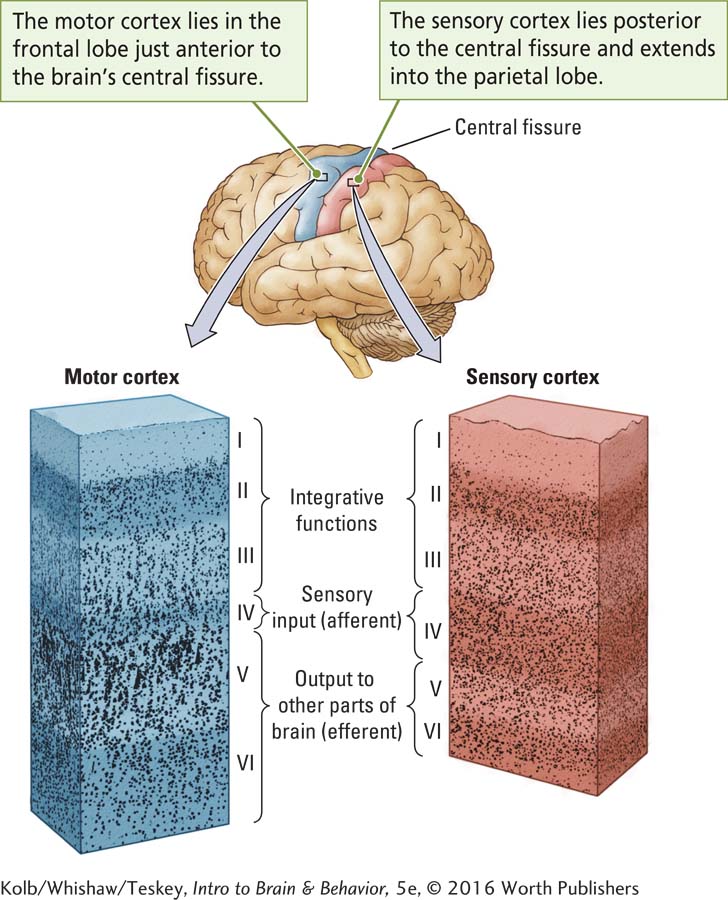
Layering in the Neocortex plumbs the depths of the primary motor cortex (shown in blue) and adjacent sensory (red) cortical regions. Viewed through a microscope, the six cortical layers differ in appearance, characteristics, and functions. Layer IV is relatively thick in the sensory cortex but relatively thin in the motor cortex. Layer V is relatively thick in the motor cortex and relatively thin in the sensory cortex. Cortical layer IV is afferent and layer V is efferent, and that makes sense: sensory regions have a large input layer and motor regions, a large output layer.
Forebrain: Initiating Movement
Complex movements consist of many acts. Consider playing basketball. At every moment, players must make decisions and perform actions. Dribble, pass, and shoot are different movement categories, and each can be performed in many ways. Skilled players choose among the categories effortlessly and blend them together seemingly without thought.
Lashley experimented for three decades to find the location of memory in the brain. He failed.
An early explanation for control of such complex movements centered on feedback: after we act, we wait for feedback about how well the action has succeeded, then make the next movement. The pioneering neuroscience researcher Karl Lashley (1951), in the article “The Problem of Serial Order in Behavior,” found fault with this explanation.
Lashley realized that we perform skilled movements too quickly to rely on feedback about one movement before shaping the next. The time required to receive feedback about the first movement combined with the time needed to develop a plan for the subsequent movement and send a corresponding message to muscles is simply too long for effective action. Lashley argued that movements must be performed as motor sequences, with the next sequence held in readiness while the ongoing one is under way.
All complex behaviors, including speaking, piano playing, and playing basketball, require selecting and executing multiple movements as sequences. Most of our motor learning is mastering sequences of action. As one sequence is being executed, the next sequence is being prepared to follow the first smoothly. The act of speaking illustrates this activity. When people use complex rather than simple word sequences, they are more likely to pause and make umm and ahh sounds, suggesting that it is taking them more time than usual to organize their speech sequences.
Initiating a Motor Sequence
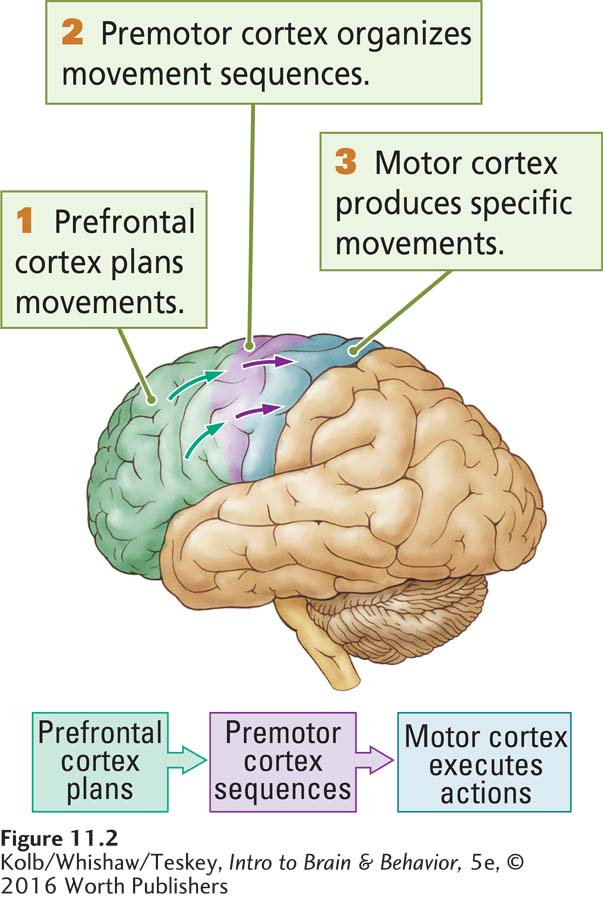
The frontal lobes are responsible for planning and initiating motor sequences. Each frontal lobe is divided into several hierarchically arranged motor regions, including the three illustrated in Figure 11-2. From front to back, they are prefrontal cortex, premotor cortex, and primary motor cortex.
Sections 12-4 and 15-2 explore cognitive deficits caused by frontal lobe injury.
PREFRONTAL CORTEX Atop the hierarchy, the prefrontal cortex (PFC) plans our behavior. Deciding to get up at a certain hour to arrive at work on time, to stop at the library to return a book, even whether a behavior is right or wrong and whether it should be performed at all are examples. Humans with PFC injury often break social and legal rules not because they do not know the rules or the consequences of breaking them but because their decision making is faulty. The PFC does not specify the precise movements to be made. It simply specifies the goal.
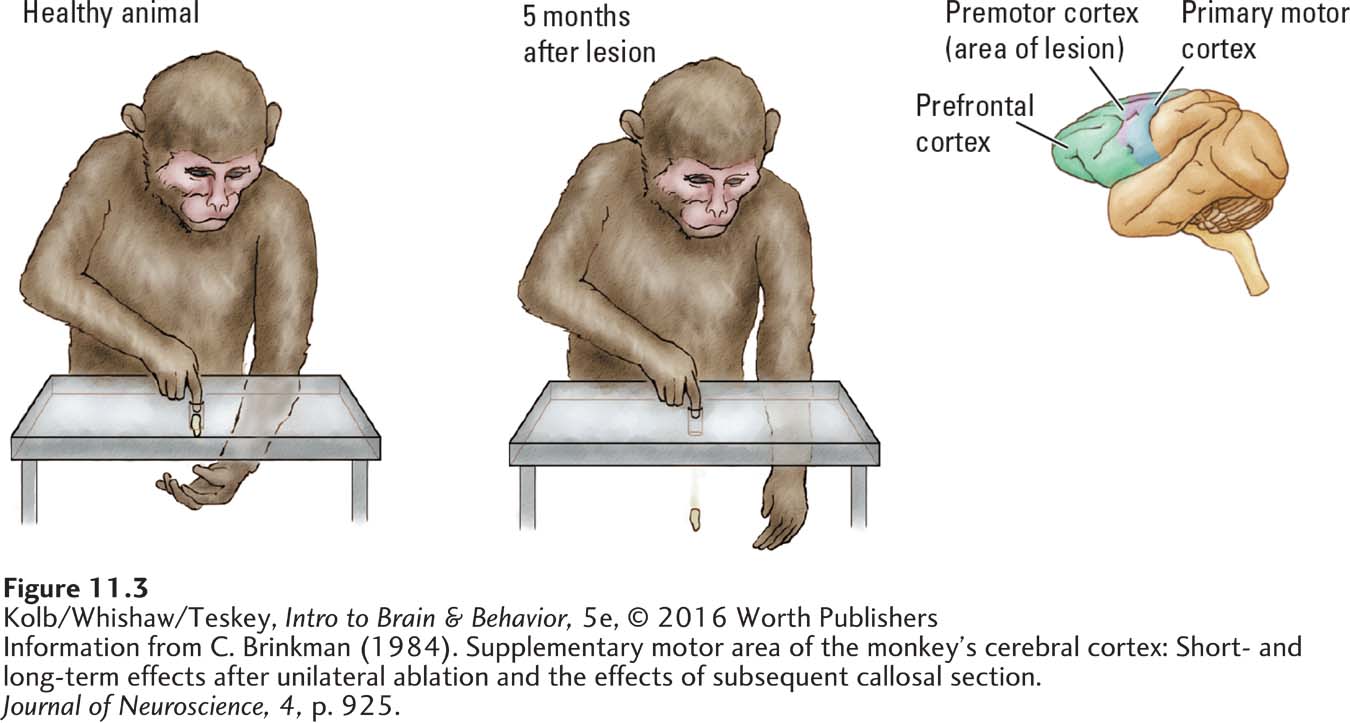
PREMOTOR CORTEX To bring a plan to completion, the prefrontal cortex sends instructions to the premotor cortex, which produces movements coordinating many body parts. If the premotor cortex is damaged, sequences cannot be coordinated and goals cannot be accomplished. For example, the monkey on the right in Figure 11-3 has a lesion in the dorsal premotor cortex. The monkey has been given the task of extracting a piece of food wedged in a hole in a table (Brinkman, 1984).
Recall the principle from Section 2-6: Brain circuits process information hierarchically and in parallel.
The monkey simply pushes the food with a finger. The food drops to the floor and is lost. The monkey has to catch the food by holding a palm beneath the hole as the food is being pushed out. But this brain-
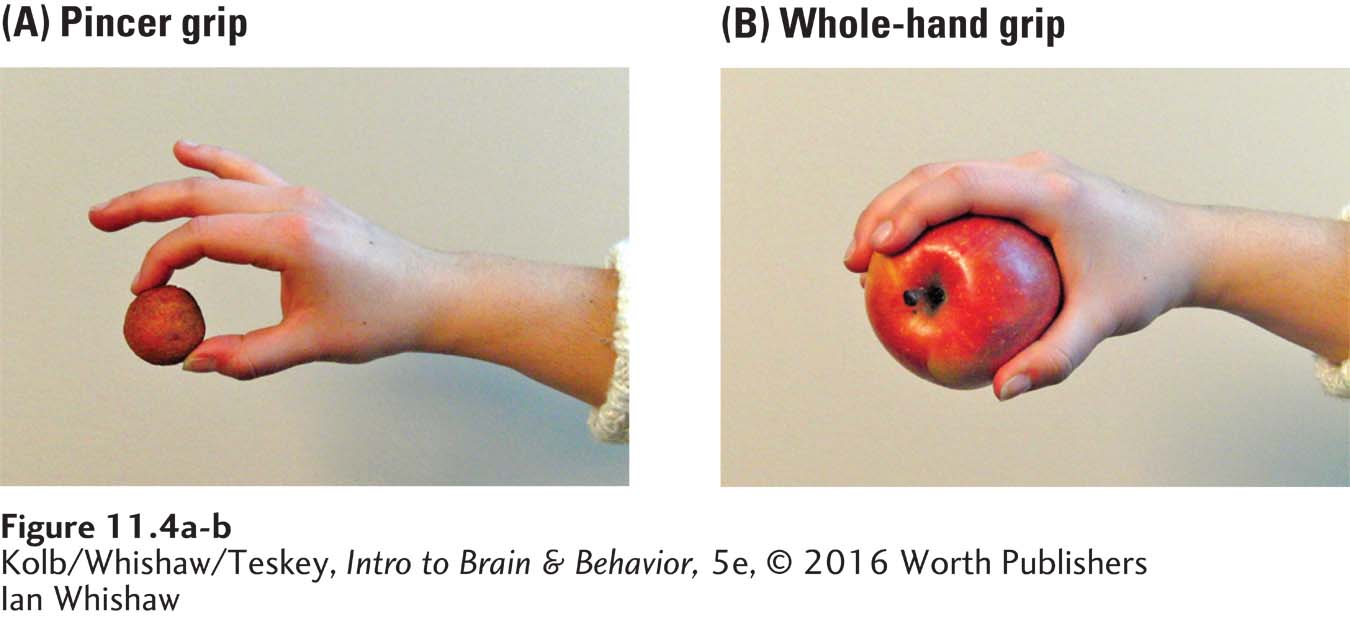
PRIMARY MOTOR CORTEX The primary motor cortex (area M1) specializes in producing focal skilled movements, such as those involving our arms, hands, and mouth. To understand its role, consider the rich array of movements we can use to grasp objects. We can hold them in one hand, with two hands, or between a hand and another part of the body, for example.
In using the precision pincer grip (Figure 11-4A), we hold an object between the thumb and index finger. We can perform many precision grips using the thumb and other fingers in opposition. The pincer grip not only allows us to pick up small objects easily but also allows us to use them with considerable skill. In contrast, when using a power grip (Figure 11-4B), we hold an object with all our fingers and with more power but fewer skilled options.
People with damage to M1 have difficulty performing reaching movements and shaping their fingers correctly to perform various hand grasps. They also have difficulty performing many skilled hand, arm, and trunk movements, bringing the hand to the mouth to feed themselves, and in talking (Lang & Schieber, 2004).
Experimental Evidence for a Movement Hierarchy
Section 7-4 describes imaging methods that record and measure blood flow in the brain.
The frontal lobe regions in each hemisphere that plan, coordinate, and execute different kinds of movements are hierarchically related. After the prefrontal cortex formulates a plan of action, it instructs the premotor cortex to organize the appropriate movement sequence, which the primary motor cortex executes. This hierarchy is supported by findings from studies of cerebral blood flow, which serves as an indicator of neural activity. Figure 11-5 shows the brain regions that were active as the participants in one such study performed various tasks (Roland, 1993).
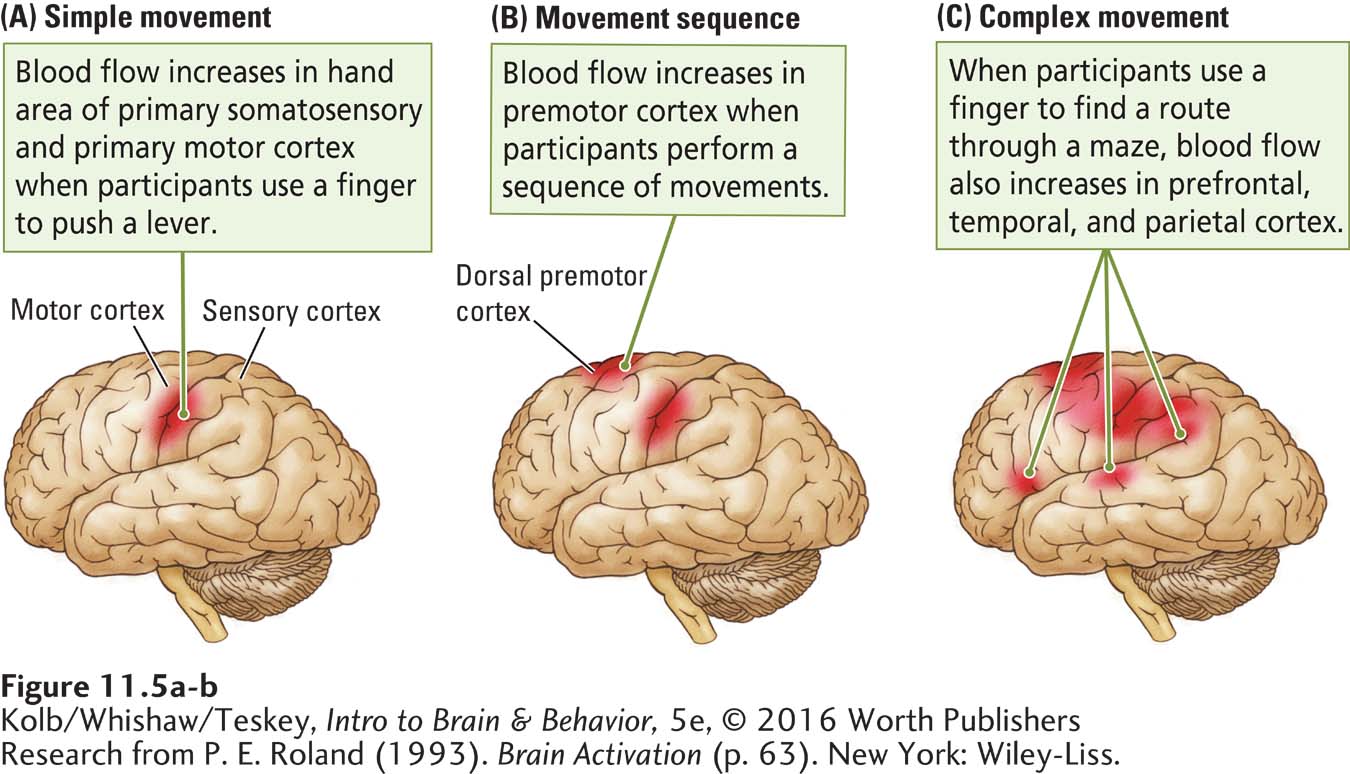
As the participants use a finger to push a lever, increased blood flow is limited to the primary somatosensory and primary motor cortex (Figure 11-5A). As the participants execute a sequence of finger movements, blood flow also increases in the premotor cortex (Figure 11-5B). And as the participants use a finger to trace their way through a maze, a task that requires coordinated movements in relation to a goal, blood flow increases in the prefrontal cortex as well (Figure 11-5C). Notice that as the participants were performing these tasks, relative blood flow increased most in the regions taking part in the required movements rather than throughout the frontal lobe.
Brainstem: Species-Typical Movement
Section 1-5 introduces species-
In a series of studies, the Swiss neuroscientist Walter Hess (1957) found that the brainstem controls species-
EXPERIMENT
Question: What are the effects of brainstem stimulation under different conditions?
By stimulating the brainstem, Hess elicited the innate movements that the animal might be expected to make. A resting cat could be induced to suddenly leap up with an arched back and erect hair as though frightened, for example, by an approaching dog. The elicited movements began abruptly when the stimulating current was turned on and ended equally abruptly when it was turned off. An animal performed such species-
The actions varied, depending on the brainstem site that was stimulated. Stimulating some sites produced head turning; others, walking or running; and still others elicited displays of aggression or fear. The animal’s response to a particular stimulus could be modified accordingly. For instance, when shown a stuffed toy, a cat responded to electrical stimulation of some brainstem sites by stalking it and to stimulation of other sites by showing fear and withdrawing.
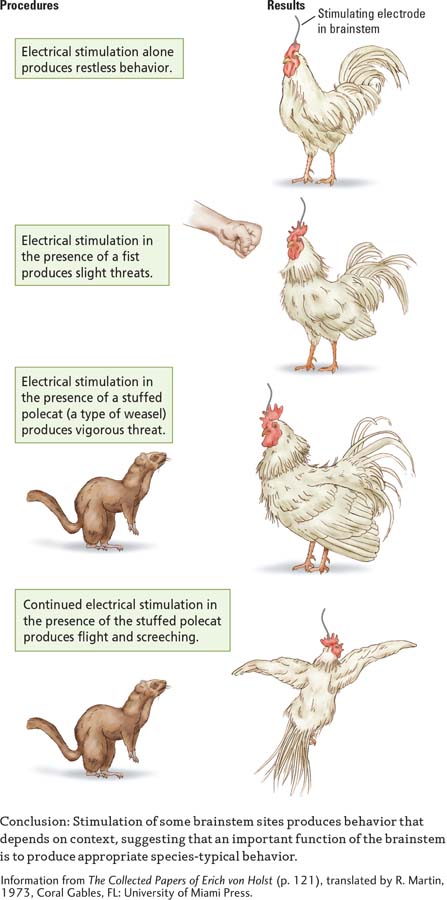
Hess’s experiments have been confirmed and expanded on by other researchers using many animal species. Experiment 11-1 shows the effects of brainstem stimulation on a chicken under various conditions (von Holst, 1973). Notice the effect of context: how the neural site stimulated interacts both with the object presented and with the stimulation’s duration.
With stimulation at a certain site alone, the chicken displays only restless behavior. When a fist is displayed, the same stimulation elicits slightly threatening behavior. When the display switches from a fist to a stuffed polecat, the chicken responds with vigorous threats. Finally, with continued stimulation in the presence of the polecat, the chicken flees, screeching.
Such experiments show that producing complex patterns of adaptive behavior is an important brainstem function. These adaptive patterns include movements used in eating and drinking and in sexual behavior. Animals can be induced to display survival-
Grooming illustrates how the brainstem coordinates complex action patterns (Kalueff et al., 2007). A grooming rat sits back on its haunches, licks its paws, wipes its nose with its paws, then wipes its paws across its face, and finally turns to lick the fur on its body. These movements are always performed in the same order, from the face to the shoulders and then toward the rear of the body. The next time you dry off after a shower or swimming, note the grooming sequence you use. Humans’ grooming sequence is very similar to the one rats use.
Focus 4-4 details ALS.
The brainstem is also important for maintaining posture, standing upright, coordinating limb movements, swimming and walking, grooming the fur, and making nests. The effects of damage to brainstem regions that organize many adaptive movements can be seen in the effects of locked-
The effects of brainstem damage on behavior can also be seen in cerebral palsy (CP), a disorder primarily of motor function: making voluntary movements becomes difficult, whereas many aspects of conscious behavior controlled by the cortex may remain intact. CP is often caused by brainstem trauma before or shortly after birth. As described in Clinical Focus 11-2, Cerebral Palsy, trauma leading to cerebral palsy can sometimes happen in early infancy as well. Advances in neuroprosthetic technology, touch-
11-2
Cerebral Palsy
E. S. had a cold and infection when he was about 6 months old. Subsequently, he had great difficulty coordinating his movements. As he grew up, his hands and legs were almost useless and his speech was extremely difficult to understand. E. S. was considered intellectually disabled and spent most of his childhood in a custodial school.
When E. S. was 13 years old, the school bought a computer. One teacher attempted to teach E. S. to use it by pushing the keys with a pencil held in his mouth. Within a few weeks, the teacher realized that E. S. was extremely intelligent and could communicate and complete school assignments on the computer. He eventually received a motorized wheelchair that he could control with finger movements of his right hand.
Assisted by the computer and the wheelchair, E. S. soon became almost self-
William Little, an English physician, first noticed in 1853 that difficult or abnormal births could lead to later motor difficulties in children. The disorder that Little described was cerebral palsy (also called Little disease), a group of disorders that result from brain damage acquired perinatally (at or near birth). Cerebral palsy is common worldwide, with an incidence estimated to be 1.5 in every 1000 births. Among surviving babies who weigh less than 2.5 kilograms at birth, the incidence is much higher—
The most common causes of cerebral palsy are birth injury, especially due to anoxia, a lack of oxygen, and genetic defects. Anoxia may result from a defect in the placenta, the organ that allows oxygen and nutrients to pass from mother to child in utero, or it may be caused by a tangled umbilical cord that reduces the oxygen supply to the infant during birth. Other causes include infections, hydrocephalus, seizures, and prematurity. All may produce a defect in the immature brain before, during, or just after birth.
Most children with cerebral palsy appear healthy in the first few months of life, but as the nervous system develops, motor disturbances become progressively more noticeable. Common symptoms include spasticity, an exaggerated contraction of muscles when they are stretched; dyskinesia, involuntary extraneous movements such as tremors and uncontrollable jerky twists (athetoid movements); and rigidity, or resistance to passive movement. Everyday movements are abnormal, and the affected person may be confined to a wheelchair.
As a means for investigating the relationship between brain development and susceptibility to brain injury, investigators can use an MRI-

Spinal Cord: Executing Movement
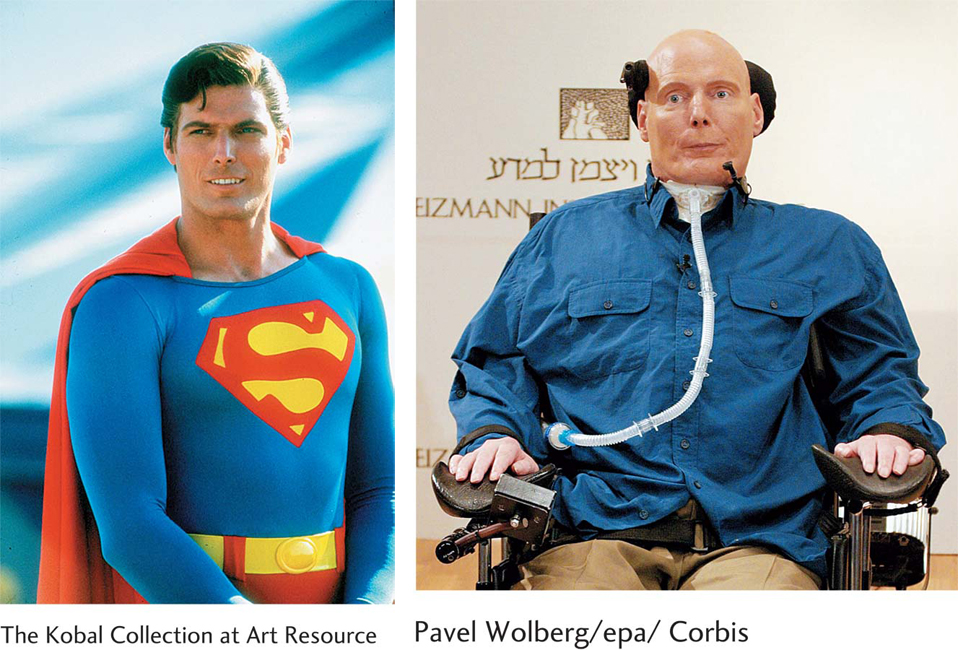
The late actor Christopher Reeve, who portrayed Superman in three 1980s films, was thrown from a horse during a riding competition in 1995. Reeve’s spinal cord was severed near its upper end, at the C1–
Other than head movements and slight movement in his shoulders, Reeve’s body was completely paralyzed. He was even unable to breathe without assistance. A century ago such a severe injury would have been fatal, but modern and timely medical treatment allowed Reeve to survive for nearly a decade.
A cut high on the spinal cord, such as Christopher Reeve survived, entails paralysis and loss of sensation in the arms and legs, a condition called quadriplegia. If the cut is low, paraplegia results: paralysis and loss of sensation are confined to the legs and lower body, as described in Clinical Focus 11-3, Spinal Cord Injury, on page 365. Christopher Reeve and his late wife Dana founded the Christopher and Dana Reeve Foundation for spinal cord research. It is dedicated to improving the life and function of spinal cord–
Far from being a mere relay between the body and brain, the spinal cord contains complex motor programs. A spinal cord patient can walk on a conveyor belt if the body is supported. Indeed, Christopher Reeve was able to walk in a swimming pool, where his body was supported by water.
When a spinal cord patient’s leg is moved backward on a conveyor belt, causing the foot to lose support, the limb reflexively lifts off the belt and swings forward underneath the body. As the foot touches the surface of the belt again, tactile receptors initiate the reflex that causes the foot to push against the surface and support the body’s weight. In this way, several spinal reflexes work together to facilitate the complex movement of walking. Walking’s reflexive organization can even be obtained in a premature or newborn baby: when held upright, the baby will perform stepping movements.
Among the complex reflexes observed in other vertebrates is the scratch reflex. Here, an animal reflexively scratches a part of its body in response to a stimulus from the body surface. The complexity of the scratch reflex is revealed in the movement’s accuracy. Absent the brain’s direction, the tip of a limb, usually a hind limb in a quadruped, can be correctly directed to the irritated body part. Typically, itching is the sensation that elicits scratching; it is likely that the sensory receptors on the skin that produce itch evolved for detecting parasites and other foreign objects. We return to itching sensations in Section 11-4.
In humans and other animals with a severed spinal cord, spinal reflexes still function, even though the spinal cord is cut off from communication with the brain. As a result, the paralyzed limbs may display spontaneous movements or spasms. But the brain can no longer guide the timing of these movements. Consequently, reflexes related to bladder and bowel control may have to be artificially stimulated by caregivers.
11-3
Spinal Cord Injury
Each year, on average, about 11,000 people in the United States and 1000 people in Canada undergo spinal cord injury (as reported by the Foundation for Spinal Cord Injury). Nearly 40 percent of these injuries occur in traffic accidents and another 40 percent occur as a result of falls. Often the spinal cord is completely severed, leaving an individual with no sensation or movement from the site of the cut downward.
Although 12,000 annual spinal cord injuries may seem like a large number, it is small relative to the number of people in the United States and Canada who undergo other kinds of nervous system damage each year. To increase public awareness of their condition and promote research into possible treatments, some, like Christopher Reeve and Canadian Rick Hansen, have been especially active.
Hansen’s paraplegia resulted from a lower thoracic spinal injury in 1975. Twelve years later, to raise public awareness of the potential of people with disabilities, he wheeled himself 40,000 kilometers around the world to raise funds for the Man in Motion Legacy Trust Fund. The fund contributes to rehabilitation, wheelchair sports, and public awareness programs. In 2008 it sponsored the Blusson Spinal Cord Centre in Vancouver, Canada, the largest institution in the world dedicated to spinal cord research, housing over 300 investigators.
Spinal cord injury is usually due to trauma to the cord that results in a number of secondary degenerative processes. These processes increase the size of the lesion. Thereafter, the formation of scar tissue, a cavity, and cysts block communication between the two severed sides. Research on spinal cord injury is directed at minimizing the acute changes that take place after the insult, devising ways to facilitate neural communication across the injury, and improving mobility and home care.
Nanotechnology, the science of making and using molecular-
Nanotubes, or nanovesicles, can be engineered to transport drugs, RNA, or new stem cells into the area of injury, where they can arrest degenerative changes and help form neural bridges across the injury (Sharma & Sharma, 2012). Nanotubes that can carry chemicals or conduct electrical impulses can be threaded into the injury through blood vessels and then into the very small capillaries within the spinal cord. Or they can be injected as molecules that self-
Nanoscaffolding, introduced into the injury to form a bridge, can aid the regrowth of axons across the injury (Imani et al., 2015). Nanoaxons can be introduced into the region of injury to synapse with neurons on both sides of the injury and to carry messages across the injury. Because they are small, nanomedicinal substances can interface with spinal cord cells on both sides of an injury.

11-1 REVIEW
A Hierarchy of Movement Control
Before you continue, check your understanding.
Question 1
The motor system is organized as a ____________.
Question 2
The ____________ cortex plans movements, the ____________ cortex organizes movement sequences to carry out the plan, and the ____________ cortex executes precise movements.
Question 3
The ____________ is responsible for species-
Question 4
In addition to serving as a pathway between the brain and the rest of the body, ____________ the independently produces reflexive movements.
Question 5
Explain what happens when the brain is disconnected from the spinal cord and why.
Answers appear in the Self Test section of the book.