13-6 Sleep Disorders
Occasional sleep disturbances are annoying and may impair performance the following day. About 15 percent of people complain of ongoing sleep problems; an additional 20 percent complain of occasional sleep problems. As people age, the incidence of complaints increases.
In the extreme, a rare genetic condition, fatal familial insomnia, causes individuals to stop sleeping altogether. Their insomnia contributes to death after a number of months without sleep. Prions (misfolded proteins) are proposed to cause the condition. A proposed treatment is doxycycline, an antibiotic with antiprion activity (Forloni et al., 2015). In this section we consider more common dysfunctions of NREM sleep and REM sleep (for more about prion disorders, see Chapter 16).
Disorders of NREM Sleep
Narcolepsy derives from the Greek words for numbness and to be seized.
The two most common sleep disorders occur during NREM sleep are insomnia, prolonged inability to sleep, and narcolepsy, uncontrollably falling asleep at inappropriate times. Insomnia and narcolepsy are related, as anyone who has stayed up late at night can confirm: a night without sleep is often accompanied by a tendency to fall asleep at inconvenient times the next day.
Insomnia
Our understanding of insomnia is complicated by the wide variation among people in how much time they spend asleep. Some short sleepers may think they should sleep more, and some long sleepers may think they should sleep less. Yet the sleeping pattern may be appropriate for each.
People’s sleep is disrupted by lifestyle choices such as those described in Clinical Focus 13-1. Staying up late, for example, may set a person’s circadian rhythm forward, encouraging a cascade of late sleep followed by staying up still later. Indoor and outdoor light pollution contributes to sleep disorders by disrupting circadian rhythms. Some sleep problems are brought on by shift work or by jet lag, as described in Section 13-1. Other common causes of sleep disorders are stress, long work hours, and an irregular lifestyle. Just worrying about insomnia is estimated to play a major role in 15 percent of cases.
Depressed people may sleep too much or too little. Anxiety and depression account for about 35 percent of insomnias. Quantitative differences also exist in depressed patients’ sleep because they enter REM sleep very quickly, as do people who are sleep-
Section 6-4 presents theories of drug tolerance and dependence.
Insomnia is brought on by sedative-
Narcolepsy
Like many people, you may suddenly have been overcome by an urge to sleep at an inconvenient time, perhaps while attending a lecture. For some people such experiences with narcolepsy are common and disruptive. J. S., a junior in college, sat in the front row for his course on the brain. Within a few minutes after each class began, he dropped off to sleep. The instructor became concerned and asked J. S. to stay after class to discuss his sleeping behavior.
J. S. reported that sleeping in classes was a chronic problem. Not only did he sleep in class, he fell asleep whenever he tried to study. He even fell asleep at the dinner table and in other inappropriate locations. His sleeping problem had made getting through high school a challenge and was making it difficult for J. S. to pass his college courses.
About 1 percent of people have narcolepsy, which takes surprisingly varied forms. J. S. fell asleep while sitting still, and his sleeping bouts consisted of brief spurts of NREM sleep lasting 5 to 10 minutes. This pattern is similar to napping and to dropping off to sleep in class after a late night but is distinguishable as narcolepsy by its frequency and disruptive effect. J. S. eventually discussed his problem with his physician and received a prescription for Ritalin, an amphetaminelike drug that stimulates dopamine transmission. The treatment proved helpful.
Apnea from Latin a, not, and pnea, breathing.
Studies of narcoleptic people in sleep clinics resulted in a surprising discovery concerning one cause of narcolepsy: sleep apnea, an inability to breathe during sleep. Clinical Focus 13-5, Sleep Apnea, describes a person who spent all night every night waking up to breathe. This nighttime behavior left him extremely tired and caused him to nod off in the daytime. Being overweight contributes to sleep apnea as well as to metabolic syndrome. Clearly the relationship between sleep and health is both complex and interconnected.
13-5
Sleep Apnea
The first time I went to a doctor for my insomnia, I was twenty-
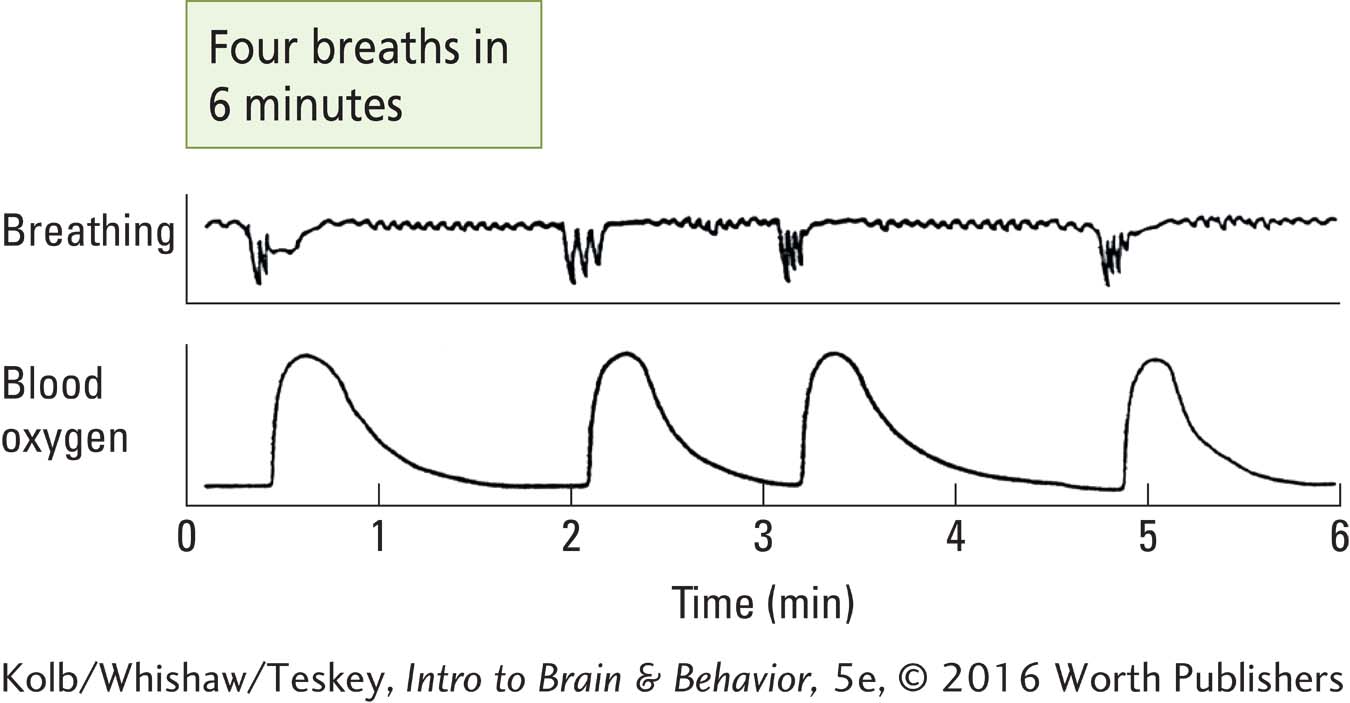
When this patient entered the Stanford University Sleep Disorders Clinic in 1972, recording electrodes monitored his brain, muscle, eye, and breathing activity while he slept (see Figure 13-11). The attending researchers were amazed to find that he had to wake up to breathe. They observed that he would go more than a minute without breathing before he woke up, gasped for breath, and returned to sleep. Then the sequence began again.
Sleep apnea may be produced by a CNS problem, such as weak neural command to the respiratory muscles, or it may be obstructive, caused by collapse of the upper airway. When people with sleep apnea stop breathing, they either wake up completely and have difficulty getting back to sleep or they partially awaken repeatedly throughout the night to gasp for breath.
Sleep apnea affects people of all ages and both sexes, and 30 percent of those older than 65 may have some form of it. Sleep apnea can even occur in children; it may be related to some cases of sudden infant death syndrome (SIDS), or crib death, in which otherwise healthy infants inexplicably die in their sleep. Sleep apnea is thought to be more common among overweight people and those who snore, two conditions in which airflow is restricted.
Treatments for sleep apnea include surgery or an appliance to expand the upper airway, weight loss, and a face mask to deliver negative pressure to open the airway. Untreated sleep apnea can cause high blood pressure and other cardiovascular disease, memory problems, weight gain, impotence, headaches, and brain damage due to oxygen insufficiency (Corrêa Cde et al., 2015).
Disorders of REM Sleep
Several sleep disorders are associated with the unexpected onset of atonia and dreams, two main features of REM sleep. We describe three: sleep paralysis, cataplexy, and REM sleep behavioral disorder.
Sleep Paralysis
In sleep paralysis both atonia and dreaming can occur when a person is awake, usually just falling asleep or waking up. L. M., a college senior, recounted the following experience.
She had just gone to sleep when her roommate came into their room. L. M. woke up and intended to ask her roommate if she wanted to go skating the next morning but found herself unable to speak. She tried to turn her head to follow her roommate’s movements across the room but found that she was paralyzed. She had the terrifying feeling that some creature was hiding in the bathroom waiting for her roommate. She tried to cry out but produced only harsh gurgling noises. In response to these peculiar noises the roommate knocked her out of her paralysis by hitting her with a pillow.
Sleep paralysis is common. In informal class surveys almost a third of students report having had such an experience, as do some war veterans during group therapy sessions. The atonia is typically accompanied by dread or fear. It seems likely that in sleep paralysis a person has entered REM sleep partially. He or she is dreaming, atonia has occurred, but the sleeper remains “awake.” When sleep paralysis occurs as a person wakes up, the paralysis and dreaming characteristic of a REM episode continue.
Cataplexy
The word cataplexy comes from the Greek word kataplessein, meaning to strike down. Hypnogogic comes from the Greek hypnos, sleep and agogos, leading into.
The atonia of REM sleep can also occur while a person is awake and active, a condition called cataplexy. The person loses muscle tone and gradually or even quickly falls to the floor, atonic. The collapse can be so sudden that injury is a real risk. Cataplexy can be triggered by excitement or laughing. While in an atonic condition, the person sees imaginary creatures or hears imaginary voices. People who fall into a state of cataplexy with these hypnogogic hallucinations give every appearance of having fallen into REM sleep while remaining “awake.”
Figure 3-21 explains inheritance patterns for genetic disorders.
Cataplexy can have a genetic basis. In 1970 William Dement was given a litter of Doberman pinscher dogs and later a litter of Labrador retrievers. These dogs displayed cataplexy. The disease is transmitted as a recessive trait: to develop it, a dog must inherit the gene from both its mother and its father. The descendants of those dogs continue to provide animal models for investigating the neural basis of the disease as well as its treatment.
View a researcher working with narcoleptic dogs at https://www.youtube.com/watch?v=R6_hwbp97eU.
Jerome Siegel (2004) investigated the cause of narcolepsy in dogs. He found that neurons in the subcoerulear nucleus become inactive and neurons in the magnocellular nucleus of the medulla become active during attacks of cataplexy, just as they do during REM sleep. On the basis of anatomical examinations of the brains of narcoleptic dogs, Siegel suggested that the death of neurons in the amygdala and adjacent forebrain areas is a one-
A remarkable discovery that came from this line of investigation is that a subset of these affected neurons produces a peptide called orexin (also called hypocretin) that serves as a signaling molecule to maintain wakefulness. Orexin cells, which are located in the hypothalamus, send projections to many other brain regions, as do the nonspecific activating systems using acetylcholine and serotonin. This suggests that orexin plays a role in maintaining activity during waking.
Section 3-3 investigates knockout technology and other genetic engineering techniques.
View a dancer experiencing narcolepsy with cataplexy at https://www.youtube.com/watch?v=1PuvXpv0yDM.
To test the idea that orexin loss is related to cataplexy, investigators have bred knockout mice that lack orexin. When these mice become active, such as at feeding time, they collapse into cataplexy, supporting the idea that an orexin system contributes to healthy waking behavior. Research with mice also suggests that lifestyle may contribute to orexin cell loss. Mice fed a high-
REM Sleep Behavioral Disorder
In Section 13-4 we described REM sleep behavioral disorder (REM without atonia), a symptom displayed by some people who take antidepressant drugs. They wake up seemingly acting out dream activity. In Section 13-5 we described Jouvet’s experiment: he reported that cats with lesions to the subcoerulear region of the brainstem entered REM sleep without accompanying atonia and so apparently acted out their dreams.
A similar condition reported in people may have either a genetic basis or a neurological cause associated with aging. People who display REM sleep behavioral disorder behave as though they are acting out their dreams (Mahowald & Schenck, 2015). Following is the account of a 67-
I had a dream where someone was shooting at me with a rifle and it was in a field that had ridges in it, so I decided to crawl behind a ridge—
In the dream the patient saw vivid images but heard nothing and felt afraid. Although many patients have described such experiences, most are elderly and suffer from brain injury or other brain-
13-6 REVIEW
Sleep Disorders
Before you continue, check your understanding.
Question 1
Disorders of NREM sleep include ____________, in which a person has difficulty falling asleep at night, and ____________, in which a person falls asleep involuntarily in the daytime.
Question 2
Treating insomnia with sleeping pills, usually sedative-
Question 3
Disorders of REM sleep include ____________, in which a person awakens but cannot move and is afraid, and ____________, in which a person may lose all muscle tone and collapse while awake.
Question 4
The people who act out their dreams, a condition termed ____________, may have damage to the ____________ nucleus.
Question 5
Is orexin the substance that produces waking?
Answers appear in the Self Test section of the book.