Chapter Introduction
How Do We Learn
and Remember?
CLINICAL FOCUS 14-
STUDYING LEARNING AND MEMORY IN THE LABORATORY
EXPERIMENT 14-
TWO CATEGORIES OF MEMORY
WHAT MAKES EXPLICIT AND IMPLICIT MEMORY DIFFERENT?
WHAT IS SPECIAL ABOUT PERSONAL MEMORIES?
DISCONNECTING EXPLICIT MEMORY
DISCONNECTING IMPLICIT MEMORY
CLINICAL FOCUS 14-
NEURAL CIRCUIT FOR EXPLICIT MEMORIES
CLINICAL FOCUS 14-
CLINICAL FOCUS 14-
CONSOLIDATION OF EXPLICIT MEMORIES
NEURAL CIRCUIT FOR IMPLICIT MEMORIES
NEURAL CIRCUIT FOR EMOTIONAL MEMORIES
LONG-
MEASURING SYNAPTIC CHANGE
ENRICHED EXPERIENCE AND PLASTICITY
SENSORY OR MOTOR TRAINING AND PLASTICITY
EXPERIMENT 14-
RESEARCH FOCUS 14-
EXPERIENCE-
EPIGENETICS OF MEMORY
PLASTICITY, HORMONES, TROPHIC FACTORS, AND DRUGS
EXPERIMENT 14-
SOME GUIDING PRINCIPLES OF BRAIN PLASTICITY
DONNA’S EXPERIENCE WITH TRAUMATIC BRAIN INJURY
THREE-
NEW-
EXPERIMENT 14-
LOST NEURON REPLACEMENT SOLUTION

14-1
Remediating Dyslexia
As children absorb their society’s culture, acquiring language skills seems virtually automatic. Yet some people face lifelong challenges in mastering language-
Dyslexia, impairment in learning to read, may be the most common learning disability. Children with dyslexia (from Greek words suggesting bad and reading) have difficulty learning to write as well as to read.
In 1895, James Hinshelwood, an eye surgeon, examined some schoolchildren who were having reading problems, but he could find nothing wrong with their vision. Hinshelwood was the first to suggest that children with reading problems were impaired in brain areas associated with language use. Norman Geshwind and Albert Galaburda (1985) proposed how such impairment might come about.
Struck by the finding that dyslexia is far more common in boys than in girls, they reasoned that hormones influence early brain development. They examined postmortem the brains of a small sample of people who had dyslexia and found abnormal collections of neurons, or warts, in and around the brain’s language areas.
This relation between structural abnormalities in the brain and learning disabilities is further evidence that an intact brain is necessary for healthy human functioning. Geshwind and Galaburda also found abnormalities in the auditory thalamus, suggesting a deficit in auditory processing. More recently, brain imaging has determined that, relative to the brains of healthy participants, activity is reduced in the left temporoparietal cortex of people with dyslexia.
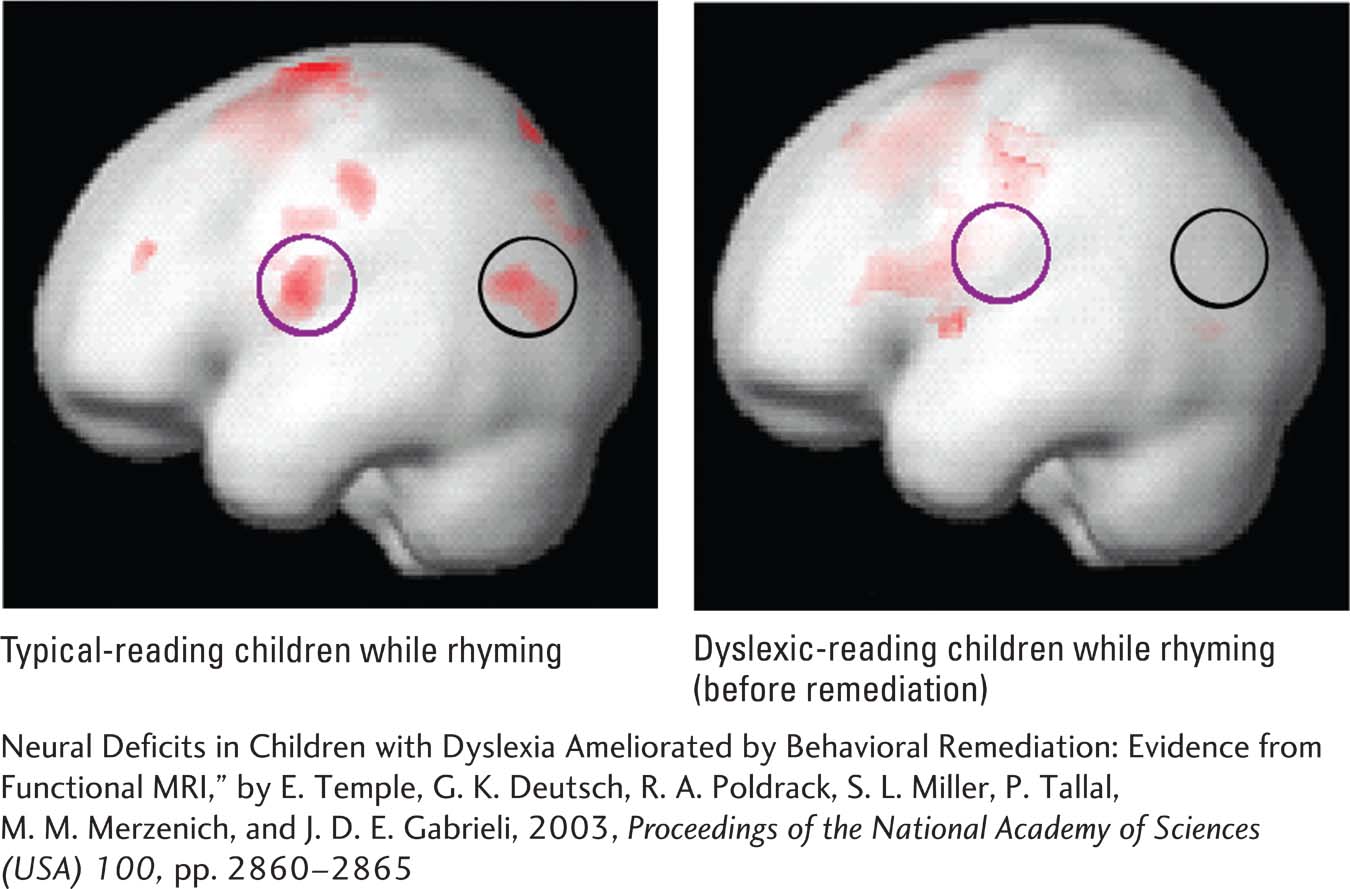
Michael Merzenich and his colleagues designed a remedial treatment program based on the assumption that the fundamental problem in learning disabilities lies in auditory processing, specifically of language sounds (e.g., Temple et al., 2003). Remediation involves learning to make increasingly difficult sound discriminations, for example, discriminating ba and da.
When the sounds are spoken slowly, discriminating between them is easy, but as they grow briefer and occur faster, discrimination becomes more difficult. Previous studies using rats and monkeys showed that discrimination training stimulates neural plasticity in the auditory system, making it capable of discrimination of sounds that previously was not possible.
The representative fMRIs shown here reveal decreased activation in many brain regions in untreated dyslexic children compared with typical children. With training, dyslexic readers can normalize their brain activity and presumably its connectivity.
The extent of increased brain activation in the language-
Neuroplasticity is the nervous system’s potential for physical or chemical change that enhances adaptability.
The brain is plastic. It changes throughout life, allowing us to modify our behavior, to adapt and learn, and to remember. If we reflect on our own lives, we can easily compile a list of experiences that must change the brain:
Profound changes during development
Acquisition of culture
Preferences among foods and beverages, art and music, and other activities and experiences
Ability to cope with the neurodegeneration of aging and to accommodate neurological injury or disease at any age
Learning is common to all these experiences. Understanding how the brain supports learning is fundamental in neuroscience. At the level of the neuron, synapses change with experience—
We can investigate neuronal changes that support learning specific types of information by describing changes in cells exposed to specific sensory experiences. Or we can look at the neural changes that mediate brain plasticity—