Chapter Introduction
Why Do We Sleep and Dream?
CLINICAL FOCUS 9-
SENSORY RECEPTORS
NEURAL RELAYS
SENSORY CODING AND REPRESENTATION
PERCEPTION
STRUCTURE OF THE RETINA
THE BASICS VISIBLE LIGHT AND THE STRUCTURE OF THE EYE
PHOTORECEPTORS
CLINICAL FOCUS 9-
TYPES OF RETINAL NEURONS
VISUAL PATHWAYS
DORSAL AND VENTRAL VISUAL STREAMS
CODING LOCATION IN THE RETINA
LOCATION IN THE LATERAL GENICULATE NUCLEUS AND REGION V1
VISUAL CORPUS CALLOSUM
SEEING SHAPE
SEEING COLOR
RESEARCH FOCUS 9-
NEURONAL ACTIVITY IN THE DORSAL STREAM
INJURY TO THE VISUAL PATHWAY LEADING TO THE CORTEX
INJURY TO THE WHAT PATHWAY
CLINICAL FOCUS 9-
INJURY TO THE HOW PATHWAY
9-1
Migraines and a Case of Blindsight
D. B.’s recurring headaches began at about age 14. A visual aura warned of a headache’s approach: an oval area of flashing (scintillating) light appeared just left of center in his field of vision. Over the next few minutes, the oval enlarged. After about 15 minutes, the flashing light vanished, and D. B. was blind in the region of the oval.
D. B. described the oval as an opaque white area surrounded by a rim of color. A headache on the right side of his head followed and could persist for as long as 48 hours. D. B. usually fell asleep before that much time elapsed. When he awakened, the headache was gone and his vision was normal again.
D. B. was subject to severe migraine, a recurrent headache usually on one side of the head. Migraines vary in severity, frequency, and duration and are often accompanied by nausea and vomiting. Migraine is perhaps the most common of all neurological disorders, affecting some 5 to 20 percent of the population at some time in their life.
Auras may be auditory or tactile as well as visual and may result in an inability to move or to talk. After an aura passes, most have a severe headache caused by a dilation of cerebral blood vessels. The headache is usually limited to one side of the head, just as the aura is on one side of the visual field. Left untreated, migraines may last for hours or even days.
D. B.’s attacks continued at intervals of about 6 weeks for 10 years. After one attack, he was left with a small blind spot, or scotoma, illustrated in the accompanying photographs. When D. B. was 26 years old, a neurologist found that a collection of abnormal blood vessels at the back of his right occipital lobe was causing the migraine attacks—
By the time he was 30, the migraines had begun to interfere with his family life, social life, and job. No drug treatment was effective, so D. B. had the malformed blood vessels surgically removed. The operation relieved his pain and generally improved his life, but a part of his right occipital lobe, deprived of blood, had died. D. B. was blind in the left half of his visual field: as he looks at the world through either eye, he is unable to see anything left of the midline.
Lawrence Weizkrantz (1986) made a remarkable discovery about D. B.’s blindness. D. B. could not identify objects in his blind area but could very accurately tell whether a light had blinked on there and even where the light was. Apparently, D. B.’s brain knew when a light blinked and where it appeared. This phenomenon is called blindsight. D. B.’s brain knew more than he was aware of consciously. D. B.’s case provides an excellent example of the parallel streams of visual processing in the cortex. His system for processing objects was impaired, but his system for locating objects in space was not.
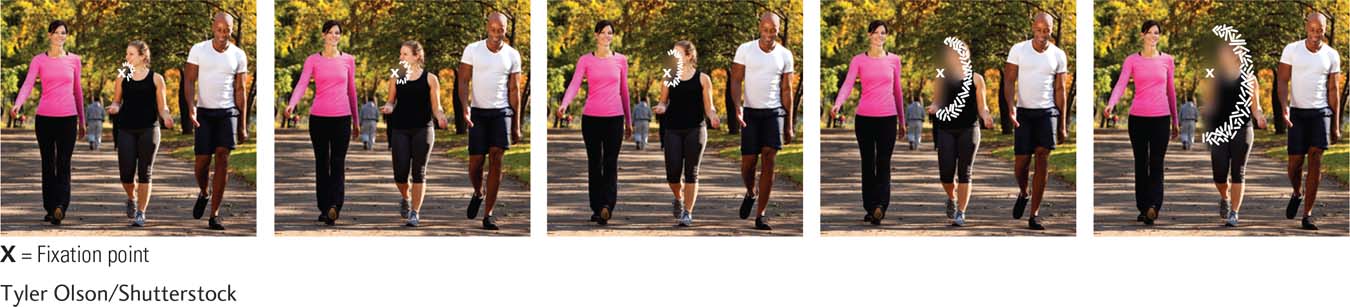
As you look at the photograph in Clinical Focus 9-1, Migraines and a Case of Blindsight, you see three people—
But how could the nervous system do this? There is no viewing screen in the brain. Instead, the nervous system must construct the image from bits of information, such as shape and color. Then the brain must put it all together to form what we perceive as a complete image. The neural reconstruction is not a passive image such as a TV screen projects. Rather, the brain continuously employs memories, both to interpret moment-
D. B.’s case demonstrates that we are consciously aware of only part of the visual information our brain is processing. This selective awareness is an important working principle behind human sensation and perception. Weizkrantz, a world-
Vision is this chapter’s main topic; hearing is Chapter 10’s. Section 11-4 covers body senses and balance. Section 12-2 explains smell and taste.
We are in fact unaware of much of the sensory processing that takes place in the neural pathways for vision, hearing, touch, taste, and smell. All our senses convert energy into neural activity that has meaning for us. We begin this chapter with a general summary of sensation and perception that explores how this energy conversion takes place.
The ability to lose conscious visual perception while retaining unconscious vision, as D. B. did, leads us to the chapter’s central question: How do we see the world? We begin by overviewing visual system anatomy. Next we consider the connections between the eyes and the sections of the brain that process visual information.
Turning to the perceptual experience of sight, we focus on how neurons respond to visual input and enable the brain to perceive features such as color, shape, and movement. At the chapter’s end, we explore vision’s culmination: understanding what we see. How do we infuse light energy with meaning to grasp the content of written words or to see the beauty in a painting? Read on.